
Abstract
Breastfeeding has a direct impact on the health of individuals and communities. Despite the implementation of diverse health promotion and education strategies, global breastfeeding rates remain relatively low. Predominantly, these strategies are implemented during the prenatal period and focus on individual-level education and behavior change, with less attention paid to the structural and contextual resources necessary for breastfeeding support and education. Breastfeeding experiences are contextually shaped by social, cultural, economic, and political factors. In addition, breastfeeding education, support, and rates are influenced by complex structures such as policy. Thus, a health equity approach to guide the planning and implementation of prenatal breastfeeding education can contribute to improving breastfeeding rates for diverse individuals and populations. Drawing from critical theoretical and health equity concepts, we present an equity approach with the potential for direct application to educating parents about breastfeeding. We discuss how a health equity approach could guide policymakers and perinatal healthcare providers to ensure culturally, emotionally, and psychologically safe learning spaces to reduce access barriers to breastfeeding education. Also, the approach could tailor the learning of parents to accommodate the unique contexts of their lives, thereby optimizing their breastfeeding experiences and outcomes.
Breastfeeding contributes to positive health benefits for the mother, the baby, and the public and includes improving the chances of the most basic, essential aspect of child health: survival (World Health Organization, n.d.). The myriad benefits range from individual-level gains in human health to the larger-scale economic and environmental effects associated with breastfeeding but not the use of artificial breastmilk (Rollins et al., 2016). Therefore, improving breastfeeding rates has been the focus of health promotion strategies since as early as the late 19th century (Wolf, 2021). Despite the historical and ongoing attention to breastfeeding education and support, rates of breastfeeding around the world remain relatively lower than expected (Rollins et al., 2016).
More recent strategies have been largely focused on individual-level behavioral change through education of formula risks versus benefits of breastmilk. These strategies are rooted in biomedicine and neoliberalism (Hausman, 2012). A well-known example of the behavioral change focus is the “breast is best” campaign. This dominant narrative about breastfeeding has been the focus of critique. Specifically, a tendency to morally frame breastfeeding as the best choice may disregard the necessity of social support and the critical role of learning the technical aspect of position and latch for optimal outcomes (Francis et al., 2020; Groleau et al., 2017; McIntyre et al., 2018). Authors who critique the dominant behavioral approach argue for a more holistic one that accounts for the social, cultural, political, and emotional aspects related to breastfeeding (Brockway et al., 2020; Francis et al., 2020; Greene et al., 2015; Groleau et al., 2017; McFadden & Erikson, 2020). A holistic approach in which contextual factors of parents’ lives are considered relevant to breastfeeding education is critical for ensuring that families have multi-level support to reduce the multigenerational effects of lower breastfeeding rates (Rollins et al., 2016).
As is widely documented, the prenatal period is a crucial time to educate individuals about breastfeeding. Breastfeeding education reflects the core principles of health promotion that emphasize the importance of tailoring educational content to individuals to accommodate the unique social, economic, and cultural context of their infant feeding goals. For the most part, breastfeeding education is provided during prenatal classes. In the classes, the educational challenge is to navigate the tension between framing breastfeeding as both a natural process and a highly skillful task (Locke, 2009).
In the findings from their integrative review of Canadian breastfeeding health promotion studies, Deo et al. (2023) indicate that parents feel under-prepared for breastfeeding as they navigate the new lived realities of doing so while balancing their prenatal expectations. The review findings indicate how the “breast is best” culture has ideological power that contributes to feelings of guilt, shame, and failing parenthood. It also undermines the self-efficacy of parents in breastfeeding. This review also highlights the emotional impacts of not meeting expected breastfeeding outcomes with parents of lower socio-economic status. Notably, these parents have a higher risk of “failing” at breastfeeding (Deo et al., 2023).
While behavioral breastfeeding education is relevant to breastfeeding success, an equity approach can expand the analysis of how intersecting structures and contextual factors impact breastfeeding outcomes. This means that for specific populations of individuals who face barriers in accessing personal resources, such as social support that are critical for breastfeeding, an equity approach emphasizes the need to mobilize support for increasing breastfeeding rates and promoting self-efficacy during the overall experience. For example, in a study conducted by Dietrich Leurer and Misskey (2015), participants typically had higher income and education levels than those of the general population of Canada. These parents had overall positive experiences and described their personal journeys with specific challenges (e.g., nipple pain). However, in a study conducted by Francis et al. (2020), parents of lower income and education referenced their social context as limiting their resources for sufficient time and energy to focus on breastfeeding.
In this paper, we argue that breastfeeding education approaches based on individualism and behaviorism lack the critical, contextual, and structural analysis of breastfeeding experiences necessary for successful infant feeding outcomes. Within the prenatal breastfeeding education literature, limited research and discussion exist to integrate equity concepts necessary for implementing strategies that account for the social determinants of health (SDoH) and differential access to resources, contexts, and support for successful breastfeeding. We propose and discuss how a health equity approach can address these limitations. In addition, we consider how the approach can more effectively tailor breastfeeding health promotion for all individuals, families, and communities, thereby achieving higher breastfeeding rates at the population level. We also integrate critical theory and social justice perspectives to provide a roadmap for designing teaching and learning approaches for perinatal care providers, including nurses, lactation consultants, doctors, mental health professionals, and policymakers. The purpose of doing so is for the design and implementation of prenatal breastfeeding education in countries such as Canada, Australia, the United States of America, and the United Kingdom.
Existing Frameworks and Models
Current frameworks and models for breastfeeding education and health promotion provide a basis from which to explore how a health equity approach can contribute to higher rates of breastfeeding within diverse communities and populations. Working to expand behavioral approaches are socioecological models, such as Revai’s (2021) relational framework, Hector et al.’s (2005) breastfeeding conceptual framework, and Busch et al.’s (2014) tri-core breastfeeding model.
The socioecological model and relational frameworks presented by Revai (2021) center on the socio-emotional connection within the parent/infant dyad, moving beyond the technical aspects of breastfeeding to integrate multiple contexts of support required for breastfeeding success. These contexts include partners; friends/family; community; healthcare organizations; and cultural, economic, and societal conditions. The relational model is concerned with the post-partum encounter of the dyad with the healthcare provider, emphasizing talking, listening, understanding, reflecting, and collaborating for history-taking, feeding, learning, and documenting. The approach involves partnering with the client while focusing on their strengths rather than using an approach that is focused on a problem or a deficit. This context-focused and strengths-based learning approach aligns with an equity orientation to breastfeeding education, which is discussed more fully in the following section.
Hector et al. (2005) focus on the individual-, group-, and society-level factors that influence the breastfeeding experience. The individual level includes the parent, infant, and dyad. It is affected by group-level factors, which address the context of a person’s environment. Examples include the home/family, community, hospital, work, and public policy environments. Further interplay includes the social-level factors, which feature social, cultural, and economic environments. Examples include cultural norms, gender roles, and food systems. Hector et al. (2005) apply this framework toward the goal of determining interventions for improving breastfeeding rates and duration. The authors highlight the importance of seeing individuals as embedded within their families, communities, and social contexts, where all levels are relevant to any successful breastfeeding experience. This multi-level context analysis reflects an understanding that we describe further using health equity concepts relevant to our proposed approach.
The tri-core breastfeeding model by Busch et al. (2014) presents three concepts required to support the parent–baby dyad: self-efficacy, lactation education, and lactation support. This model is focused on the technical aspects of breastfeeding, which include the importance of parents having confidence in their ability to breastfeed, with assistance from care providers in the form of lactation education and support. Self-efficacy is focused on the importance of social support and potential social barriers to breastfeeding, such as workplace demands. However, the social factors are not as widely addressed as the previous models that include policy, social and cultural norms, or gender roles. These models and frameworks have contributed to expanding the behavioral approach to better account for the multiple contexts impacting breastfeeding experiences and outcomes for health that promote breastfeeding education. We now focus on extending these approaches to posit how health equity can turn attention to the role of social and structural factors that impact breastfeeding and breastfeeding education. The purpose of doing so is to reduce unfair differences or inequities in successful breastfeeding outcomes.
Equity Theoretical Orientation
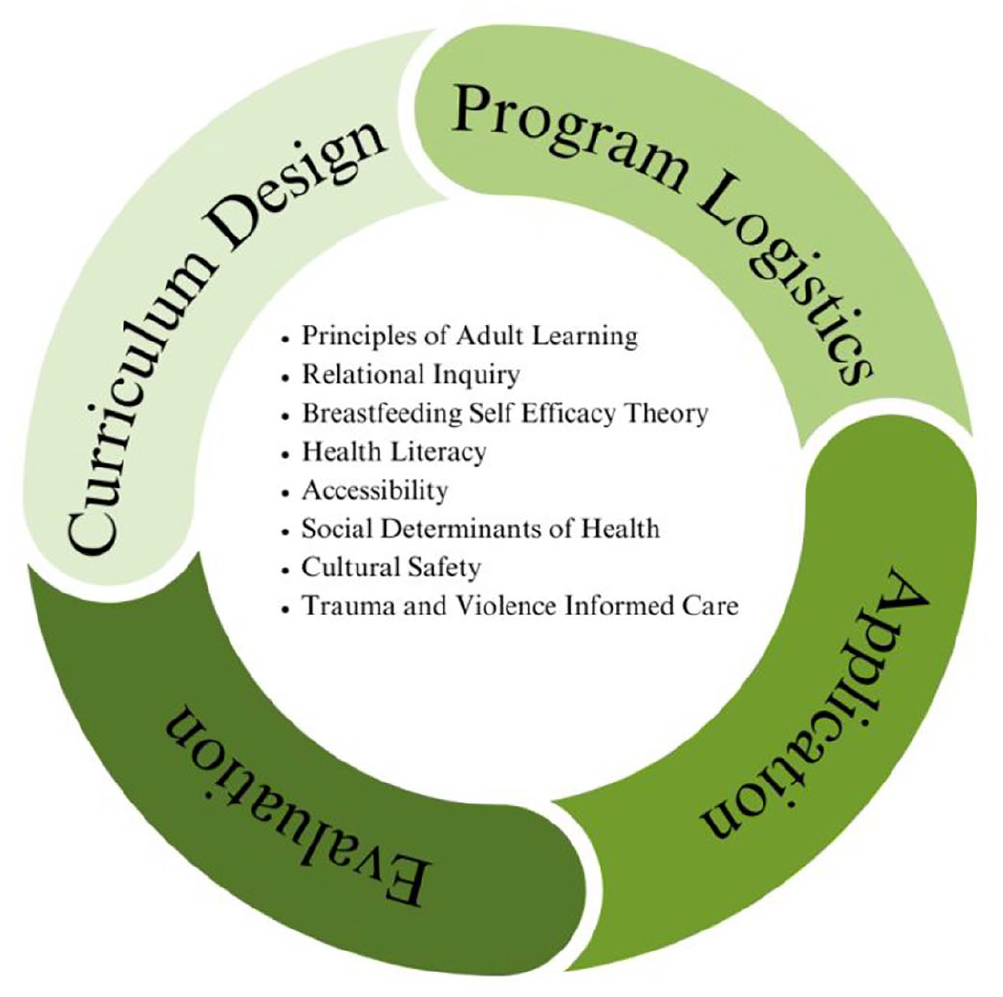
Jones and Donovan (2004) highlight the disconnect that often exists in health promotion initiatives, which occurs between the theories presented by health promotion researchers and the application of the theories in practice by health promotion practitioners. The authors highlight the importance for any health promotion approach to be grounded in theory, where the goal is meaningful and relevant translation to practice. The equity approach presented here (Figure 1) is centered on principles of adult learning, relational inquiry, and breastfeeding self-efficacy (BSE) theory; health literacy; accessibility; SDoH; cultural safety; and trauma and violence-informed care (TVIC). We outline how these theoretical principles and concepts are collectively utilized in the curriculum design, program logistics, application, and evaluation of overall prenatal education programs.
Prenatal Breastfeeding Education: A Health Equity Approach
Defining Equity
The need for an equity-based framework goes beyond the call for equality. Inequality simply indicates the presence of differences, while inequity is defined by Baum et al. (2009) as “unjust and avoidable inequalities” (p. 1967). By focusing on being fair and equal, the factors that derive from deeply rooted differences in social positioning cannot be adequately addressed. Thus, an equity-based approach is better suited to remedying such differences. Varcoe et al. (2014) recognize the reality that although nurses may believe they have committed to practicing fairness, the result of their actions may actually be a form of unfair discrimination. A commitment to equity requires the understanding that different groups and individuals have a greater need for support than others and then adapting the provided care or education based upon those needs.
Principles of Adult Learning
Adult learning principles have been developed through diverse theoretical approaches. An equity framework for adult learning aligns with the works of Freire (1970). Key considerations include the role of culture, the importance of dialogue, the educator as a facilitator, and education as a means of liberation from oppression (Lucio-Villegas, 2018). These principles can be applied to prenatal breastfeeding education in several ways.
First, the curriculum must be designed by acknowledging the diverse cultural contexts of breastfeeding and valuing this diversity among the different populations that attend the classes. Understanding how differing cultural views can create unsafe learning spaces also demonstrates the relevance of cultural safety as a learning principle for anti-racist health promotion education. Dialogue between learners and the educator can democratize the classroom setting rather than reinforce unequal power relations that can arise from didactic lectures and “banking” approaches to education, where, as described by Freire (1970), the educator “delivers” knowledge to the learners. The educator’s role ought to be facilitating learning through a collaborative process, which is realized through group discussions, interactive activities, and flexibility in course content to meet the needs of the learners in different contexts (in-person or virtual settings).
Awareness of unequal power relations between the educator and learner and of the subsequent action to create safety through the empowerment of learners can mitigate the negative effects of power dynamics often present in teaching and learning. For example, an important learning moment often not discussed in prenatal education is the impact of social norms that place higher moral value on parents who breastfeed. Deviating from this moral standard means that individuals face stigma and judgment about their parenting abilities. It also involves erasing their agency for autonomous decision-making as it concerns infant feeding (Groleau & Sibeko, 2012). An equity lens draws attention to the impact of dominant discourses and is aimed at mitigating the harmful impacts of unjust and unfair differences in health and health outcomes that are created through structural arrangements, such as poverty, racism, barriers to employment, disability, rural geography, and other systemic factors that determine health and well-being.
Relational Inquiry
Relational inquiry is described as a critical process of unpacking the interplay between the contextual, intrapersonal, and interpersonal factors surrounding an individual’s experience within healthcare (Doane & Varcoe, 2021). This iterative process of questioning and seeking to develop a deep understanding of the different factors at play is applied in the setting of the prenatal breastfeeding class, in the design of the class itself, and by the educator while teaching the class. In the design of breastfeeding health promotion education strategies, the variability in the health literacy of learners, the ability of all learners to access the course, and the intersection of the SDoH with the experience of breastfeeding all need to be considered. The educator can engage the class through relational inquiry by considering the concepts of cultural safety and TVIC. Promotion of this form of safety in an environment “requires actions that recognize, respect, and nurture the unique cultural identity of people/families and safely meet their needs, expectations, and rights” (Doane & Varcoe, 2021, p. 269). In addition, the application of TVIC requires the educator to understand the links between social inequities and the increased risk of experiencing trauma and violence. They must also recognize the additional barriers to safety that individuals typically face when interacting with healthcare services (Browne et al., 2015).
Cultural Safety
The concept of cultural safety refers to the recognition of differences in individuals and groups based on a variety of factors, such as their social positioning and historical events affecting their identity, values, ways of living, and relationships with one another (Parisa et al., 2016). In the prenatal breastfeeding class, critical self-reflection is required on the part of the educator. This reflection seeks to uncover potential biases that may be operating in the background and that relate to assumptions about cultural differences that contribute to social stigma, discrimination, and racism and create both interpersonal and structural barriers to care.
An equity model aims to promote socially just learning spaces where the life contexts of learners are considered for their breastfeeding education. Actively countering racism and discrimination is listed as a strategy that advances the implementation of equity-oriented healthcare (Browne et al., 2015). One example specific to the health promotion of breastfeeding can be seen in a study conducted by McFadden and Erikson (2020), which reveals racially discriminative practices from public health nurses toward Chinese mothers. According to the researchers, nurses held the belief that Chinese mothers were more likely to formula feed than breastfeed due to their cultural views. Subsequently, the nurses provided fewer breastfeeding services to these mothers. An important finding reflected the view that certain nurses held regarding the care that they provided. That is, the nurses were aware that they were changing their practice for Chinese individuals but did not see themselves as being discriminative. Instead, they believed they were providing culturally competent care due to their understanding of Chinese culture, which included the belief that parents would need to provide formula to their infant.
Cultural safety encourages health providers to have critical discussions regarding potential areas of inequity embedded within their practices. Through the deliberate application of this concept with educators of prenatal breastfeeding classes, we argue that the prevalence of such discriminatory practices would decrease. This example highlights the importance of resisting cultural essentialism and stereotyping that can happen when a curriculum is developed for specific cultural groups. Any curriculum design changes should be made by considering the lens of cultural safety and its specific meaning to the target population. Integrating cultural safety into a curriculum means inviting experiences from diverse parent learners within diverse ethnocultural contexts to enhance the relevance and learning for specific communities, such as newcomers to Canada. The partnership can include requesting that the staff at community centers gather suggestions about meaningful curriculum content. A staff member can also be present to promote a safe environment to ensure culturally safe learning spaces. Indigenous-specific cultural safety can be guided by Elders and Knowledge Holders to inform all aspects of curriculum design, logistical planning, and consideration for the specific social contexts of the learners.
Trauma and Violence-Informed Care
TVIC involves recognizing the potential of past trauma and violence, both interpersonal and structural, to impact one’s health (Browne et al., 2015). TVIC requires the understanding by the educator or healthcare professional “that people impacted by social inequities often experience multiple forms of violence” and that “the structural conditions of their lives often place them at greater risk of interpersonal violence, and of experiencing challenges in accessing supports to improve their physical and emotional safety” (Browne et al., 2015, p. 4). In practice, this means that the educators of the prenatal breastfeeding classes have undergone training in this concept and are also aware of the prevalence of trauma and violence commonly experienced by perinatal individuals. Training would also include the relevance of TVIC to childbearing individuals and the potential for retraumatization within the healthcare system. Application of TVIC does not include the collection of trauma histories from individuals or any form of sharing of trauma experienced by them. Instead, the facilitator of the class operates with the understanding of the potential for trauma and violence histories being present in the class.
Cultural safety and TVIC work together simultaneously to promote a psychologically safe learning environment. Building on the previous example of Chinese mothers who did not receive equal access to breastfeeding support from public health nurses, a TVIC approach would recognize the potential for unequal support received as a form of structural violence. Then, it would seek to have individuals review their own biases, which may cause further discrimination against others. These biases may include the assumption that Chinese mothers need more education on the health benefits of breastmilk over formula use, a topic that can become the focus of the class. Instead, the equitable approach would involve asking participants in the class about the topics they are most interested in learning, which may include the benefits of breastmilk. However, they may also state a preference to focus on different positions or potential challenges of breastfeeding.
Another example of a TVIC lens is the awareness of the systemic violence against Indigenous populations, including the attempted erasure of their cultural practices. Partnering with community leaders in Indigenous communities is especially important to prevent retraumatization through prenatal breastfeeding education. The healthcare workers providing this education may be well-intentioned, but without a careful and purposeful approach to applying relational inquiry, cultural safety, and TVIC, there is a risk of causing further harm and undermining successful breastfeeding education and learning.
BSE Theory
BSE theory builds on Bandura’s (1986) social cognitive theory (SCT) of learning. SCT incorporates practice, observational learning, modeling, and self-efficacy, which contribute to developing the knowledge, attitudes, and behaviors that can lead to self-efficacy. Self-efficacy is defined as “the confidence individuals have in their ability to enact behaviors or complete a task, a manipulable concept that targeted interventions can affect and explain changes in one’s behavior” (Campbell, 2021a, pp. 37–38). BSE principles can be integrated to enhance the confidence of mothers and empower their ability to breastfeed (Dennis, 1999). If prenatal breastfeeding classes are considered a tool to empower perinatal individuals to meet their infant feeding goals, the BSE principles can orient the educator to integrate demonstration, participation, and role-playing that highlight the technical act of breastfeeding (Locke, 2012). Integrating discussion of the potential challenges that may arise in the breastfeeding journey is critical and can contribute to disrupting social discourses about breastfeeding as a natural skill. BSE differs from the previously mentioned theories of adult learning and relational inquiry and may even appear contradictory due to its behavioral nature. Breastfeeding, however, is both a health behavior that is learned at the individual level and a health outcome affected by structural factors. A health equity approach weaves the different threads of breastfeeding education together to ultimately provide quality health teaching that is socially just, relevant, and effective for improving breastfeeding outcomes.
Health Literacy
Health literacy is defined as “the wide range of skills, and competencies that people develop to seek out, comprehend, evaluate and use health information and concepts to make informed choices, reduce health risks and increase quality of life” (Zarcadoolas et al., 2005, p. 196). It is further delineated by Zarcadoolas et al. (2005) into the domains of “fundamental literacy, science literacy, civic literacy and cultural literacy” (p. 197). All these domains should be considered when developing prenatal breastfeeding education. Fundamental literacy refers to the ability to read, write, and speak. For example, the learners need to know how to read the language being used for course materials. Science literacy relates to the ability to understand the medical and pathophysiology of breastfeeding needed, for example, to teach the role of hormonal or physical changes in the body to produce breastmilk. Civic literacy involves an understanding of the relationship between health behaviors and government-level policies.
Educators should be aware of policies that may affect the ability of individuals to reach their breastfeeding goals. Cultural literacy sheds light on the potential for different worldviews, beliefs, and social trends to affect the interpretation of messages being received, such that different individuals interpret the same message in different ways (Zarcadoolas et al., 2005). Such social trends and beliefs can become dominant and reinforce social norms in ways that are harmful and contribute to unequal power relations (Varcoe et al., 2014). Thus, a critical view of health literacy requires an understanding of this phenomenon. Dawkins-Moultin et al. (2016) raise the concern that dominant health promotional campaigns are primarily concerned with the behavioral and individual aspects of health literacy, lacking engagement with its critical aspect. Nutbeam (2000) describes critical health literacy as “the cognitive and skills development outcomes which are orientated towards supporting effective social and political action, as well as individual action” (p. 265).
Critical health literacy requires conceptualizing health at the societal level in addition to the community and the individual/interpersonal levels (Dawkins-Moultin et al., 2016). Increasing critical health literacy can facilitate individual agency that is shown to improve health outcomes. An equity approach to breastfeeding education helps to bring awareness of how the context of individuals’ lives and the SDoH are relevant for breastfeeding success and can thereby be considered by educators and health professionals to help mobilize needed resources to reduce unfair differences in breastfeeding outcomes. Educators focusing from an equity perspective might then ask the following questions: Is this education accessible? Does this approach have relevance, and is it a culturally safe learning space? How can I support learning that optimizes the success of those facing systemic and structural barriers to breastfeeding success? How are certain individuals marginalized from accessing community lactation support? What about new immigrants and other specific populations where language barriers exist? Promoting equitable access to positive breastfeeding experiences and outcomes requires accounting for access and the SDoH.
Accessibility
Accessibility refers to the ability of learners to access prenatal breastfeeding classes. This is a key component in the logistical phase of planning the educational programs. Promoting access involves a variety of ways for learners to attend the class, either physically or virtually. When scheduling physical classes, learners should have access to a variety of times and locations, including evenings, weekends, and inclusive community spaces such as libraries and community or health centers. Virtual options should be available to individuals who are unable to attend physically. Different methods of promoting and signing up for classes should be utilized to allow for full reach to all prenatal individuals. For example, when in-person classes are held only in urban centers where accessible transportation is not possible, this prevents access for many persons who could benefit from positive breastfeeding education. A consideration during the logistical planning can be to have several classes held near transit hubs within a short walking distance of train/bus stations. Of note, it is important to prioritize the accessibility of in-person classes over a virtual option. Breastfeeding is a technical skill that should include demonstrations and interactive practice with the use of dolls for correct positioning. In addition, it should not be assumed that everyone has access to computers and the internet to attend virtual sessions. Handouts or online resources should also be provided to the learners at the end of the class to ensure they have access to education from the course beyond their notes/memory.
Social Determinants of Health
Campbell (2021b) posits the need to situate frameworks for the health promotion of breastfeeding that are in line with the SDoH. Breastfeeding experiences, outcomes, and rates are influenced by social, historical, economic, and contextual factors, such as the cultural and economic location, gender, ability, and living conditions of individuals. Consideration of how the SDoH affect the health of groups and individuals ought to be the starting point for designing prenatal breastfeeding curricula and programming. SDoH include but are not limited to the “effects of gender, poverty, trauma, race, status (immigrant, refugee), sexual orientation, and health literacy on one’s ability to attain health and general wellbeing” (Campbell, 2021b, p. 134). The application of the SDoH overlaps with other equity concepts mentioned thus far, such as the civic and cultural components of health literacy, accessibility, cultural safety, and TVIC. For example, it is well documented that both systemic and interpersonal racism act as determinants of health by creating unfair barriers to meeting the needs of people seeking healthcare across diverse contexts.
In their scoping review, Robinson et al. (2019) highlight how the experiences of African American women in healthcare settings are shaped by racism, bias, and discrimination and have negative effects on their breastfeeding initiation and duration. Not unlike the experiences of Chinese women in Canada that were previously mentioned, African American women were denied referrals and regarded as a lower priority for breastfeeding support due to the assumption by healthcare staff that they were more likely to formula feed. These assumptions are discriminatory and contribute to racist attitudes that act as a barrier to equitable access to breastfeeding education.
A key feature of redressing racism in healthcare settings is to engage healthcare providers in unconscious bias awareness training, a health promotion intervention that is relevant across all healthcare contexts (Hagiwara et al., 2020). Furthermore, understanding how food insecurity and poverty impact breastfeeding success is necessary so that these SDoH can be addressed in breastfeeding education and resources allocated for successful breastfeeding rates. It is not enough to focus only on healthy eating during breastfeeding education without a more critical understanding of food insecurity and poverty as structural barriers to adequate nutrition for breastmilk production. Educators can focus on providing access to resources such as dieticians, community gardens, and community food co-ops. This content specific to food security ought not to be based on individuals having to disclose the need for such resources. Instead, they should be provided as part of the regular curriculum to ensure equitable access through trauma-informed and culturally safe assessment of the social and community contexts of individuals.
Evaluation
A health equity approach for prenatal breastfeeding education also requires ongoing evaluation for impact in diverse and varied communities. Program evaluation is defined by Chen (2015) as “the process of systematically gathering empirical data and contextual information about an intervention program—specifically answers to what, who, how, whether, and why questions that will assist in assessing a program’s planning, implementation, and/or effectiveness” (p. 6). The data gathered should include both quantitative and qualitative methods, with attention paid to how, when, and from whom the data are collected (Saunders et al., 2005). Fidelity, doses delivered and received, reach, context, and recruitment should all be assessed as part of the evaluation process.
The first step in program evaluation, as described by Saunders et al. (2005), is to describe the program. The theoretical basis and equity concepts discussed in this paper provide the foundation for this description. Once these theories and concepts have been integrated into practice and once prenatal education is underway, feedback should be sought from educators and learners in the class. For obtaining feedback, various methods such as questionnaires at the end of the class or online surveys can be used. Summative feedback can be collected from both the educators of the class and the participants. Potential ways of facilitating this feedback could include a working group of health educators teaching the class to discuss and review the sessions every few months to determine whether changes need to be made.
Prompts for these discussions could include the following: What went well? What challenges did you face? How did you respond to those challenges? Did the learners appear engaged? Did you receive feedback from learners? Were there parts of the course material that the learners wanted a greater focus on? Or less focus? How were the concepts of equity, relational inquiry, adult learning, health literacy, accessibility, SDoH, cultural safety, and TVIC integrated throughout the class? Was the course material sufficient? Was the full curriculum reviewed in the class as planned? Did the learners demonstrate an understanding of all the components taught in the course? Leadership should also be involved in these working groups to gather and share information regarding the overall rates of breastfeeding among the parents within the health region and further insights into the experiences of the parents coming into the health unit for breastfeeding support. For example, have public health nurses noticed an increase or decrease in specific challenges such as poor latch? Or have the nurses noted an increase in confidence among breastfeeding parents?
In addition, the demographics of the individuals attending the course should be reviewed to measure the accessibility of the course. An equitable health promotion initiative should be accessible and welcoming for all members of the community, especially those at the highest risk of poorer breastfeeding outcomes. If the classes are not being attended by people facing structural barriers (such as poverty), further exploration should be undertaken to guarantee that the program planning occurs to ensure that equity is being realized. Learners should also be provided with questionnaires to fill out after the class (either online or paper) that do not require sharing their names. This should include questions regarding the overall learning environment, such as the following: Did you feel this course allowed for an environment to ask questions without judgment? Why or why not? Are there topics you wish could have been covered in this class, and if so, which ones? How confident do you feel to breastfeed once your baby is born?
The outcomes of the classes should also be measured by assessing whether there has been a change in breastfeeding rates in the areas where they are taught. Did the participants go on to breastfeed at a higher rate compared to the rest of the population? Did the rates decrease? Or did they stay relatively the same? A unique but key characteristic of program evaluation is the need to holistically assess such outcomes (Chen, 2015). This means that the breastfeeding rates cannot be taken as the sole indicator of whether the class was or was not successful. Other factors that may have influenced breastfeeding rates also need to be considered. For example, was returning to work a cause of ceasing breastfeeding earlier than expected? If so, this ought not to be an indicator that the program failed but rather that it is an associated factor worth addressing through other public health campaigns to advocate for improved breastfeeding support for working parents.
Conclusion
Figure 1 presents the health equity approach described in the paper for the design and delivery of prenatal breastfeeding education. This approach draws from applicable theories and aims for practical application in a health education environment. Critiques of current discourse and trends in breastfeeding health education have been discussed, with the potential of equity concepts introduced to advance breastfeeding education and breastfeeding experiences, rates, and outcomes. These elements are represented visually in Figure 1. The equity approach can guide policymakers, perinatal care providers, and educators to create accountability structures for culturally, emotionally, and psychologically safe learning spaces for breastfeeding education that are accessible, relevant, and effective for diverse individuals and populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.