
Abstract
Complicated grief is both a cause and a consequence of health inequities in Native (American Indian/Alaska Native [AI/AN]) communities. Given disproportionately high rates of physical (e.g., cancer, diabetes, and heart disease) and mental health problems (e.g., substance use disorder, posttraumatic stress disorder) in Native communities, it is common for AI/AN people to suffer many losses each year. Experiences of traumatic or repeated losses may lead to the development of maladaptive grief, often known as complicated grief. The aim of the current study was to understand the perspectives of community members on grief and its connection with health inequities among AI people who have experienced the loss of a person with whom they were close. Using a community-based participatory research framework, we conducted semi-structured interviews with 12 AI adults from a rural reservation community. The ages of the participants ranged from 32 to 80 years (M = 54.33, SD = 14.46) and women (n = 7, 58.3%) and men (n = 5, 41.7%) were included. The participants reported many barriers to healthy grieving and linked chronic, complicated grief with the development of multifaceted health problems, which were seen as exacerbating health disparities and leading to additional losses and grief. While coping with loss was difficult, many people were able to heal from extraordinary losses through community support and cultural practices. Future research with AI/AN communities is needed to develop, implement, and evaluate culturally responsive therapeutic grief treatments. There is also a pressing need to address current physical and mental health inequities to reduce the mortality rate and, thus, complicated grief in AI/AN communities.
American Indian/Alaska Native (AI/AN) communities experience disproportionally high mortality rates associated with suicide, accidents/injuries, drug overdoses, alcohol-induced illnesses, and other chronic health problems (e.g., cancer, diabetes, and heart disease) (Indian Health Service, 2018). Additionally, during the COVID-19 pandemic, AI/AN people were 3.8 times more likely than White non-Hispanic populations to die from the virus (267 vs. 71 deaths per 100,000; Williamson et al., 2021; Wong et al., 2022). According to epidemiological data, the average life expectancy for AI/AN people in the United States is 73 years, which is 5.5 years shorter than that of non-Native populations (78.5 years) in the same country (Indian Health Service, 2018). Also, AI/AN people between the ages of 25 and 44 have the highest early mortality rates of all racial/ethnic groups (Espey et al., 2014). While the leading causes of death are similar for AI/AN people living in urban and rural areas, mortality rates are higher among the latter group (Jacobs-Wingo et al., 2016). The life expectancy for the estimated 40% of AI/AN people living in rural areas is 2 years less than that of their urban counterparts (Cromer et al., 2019; Singh & Siahpush, 2014; Villarroel et al., 2020).
Inequities in mortality and health outcomes experienced by AI/AN people are attributed to environmental and social determinants of health, including poverty, unhealthy physical environments, lack of access to healthcare, and discrimination (Prüss-Ustün et al., 2017; Sequist, 2017). For example, in accessing healthcare services, AI/AN people encounter many barriers, which are even greater for those living in rural areas. These barriers include limited doctor/clinician availability, inadequate health insurance, and logistical problems (e.g., lack of childcare, time off work, and transportation; Cromer et al., 2019; Sequist, 2017). In rural communities, it is not uncommon for people to travel over 100 miles for healthcare (Sequist, 2017). Higher poverty rates in AI/AN communities may prevent them from receiving chronic disease management and medical care for acute illness, leading to greater mortality risk (Cromer et al., 2019).
Due to the high mortality rates among AI/AN people, many are left to grieve the loss of a loved one. Grief refers to the emotional, psychological, behavioral, social, and physical reactions that people experience due to a loss (Boerner et al., 2015). As AI/AN populations are highly heterogeneous, grieving practices differ among tribal groups. Among certain AI/AN tribes, it is customary to enter into a one-year grieving period after the loss of a loved one (Gameon, 2021). During this year of grieving, a person may cut their hair and take part in prayer groups or sweat lodge ceremonies. They also may avoid certain social activities during this time. At the end of the year of mourning, a Wiping of the Tears ceremony commemorates the conclusion of the grieving period and signifies an acknowledgment that a loved one has passed on to the next life. Additionally, cultural customs on the appropriate waiting period for burial exist, giving a loved one an Indian name, and holding a memorial feed for the community. Also, spiritual ceremonies are used to help a loved one’s spirit move on. In addition to these traditional cultural practices, many AI/AN people seek support from Christian churches or other spiritual traditions (Rollings, 2002).
Grief and loss are ubiquitous in Native communities. Among AI/AN people, grief is not limited to recent losses. It also includes unresolved grief inherited from the trauma inflicted upon previous generations. Historical loss in AI/AN populations stems from government-sanctioned genocide policies that forced them to leave traditional lands and removed their children from their families to place them in boarding schools designed to eradicate AI/AN cultures (Bombay et al., 2014; Brave Heart & DeBruyn, 1998). Many policies that inflicted historical trauma on AI/AN people are ongoing. Current discriminatory systems continue to harm AI/AN families and communities (Evans-Campbell, 2008). This is demonstrated by disproportionately high incarceration rates and the loss of children to foster care, among other social injustices that perpetuate grief and affect health (Daniel, 2020; Jacobs et al., 2018; Maguire-Jack et al., 2020).
Historical trauma is conceptualized as a collective psychological stressor that appears in communities and can amplify psychological distress when new adversity is encountered (Evans-Campbell, 2008; Walters & Simoni, 2002). It has been associated with adverse mental health outcomes, including greater depressive symptoms, substance use, and suicidal ideation (Brockie et al., 2015; Gameon & Skewes, 2021; McQuaid et al., 2017; Tucker et al., 2016). Walters and Simoni (2002) proposed the Indigenist Stress Coping Model (ISCM) to explain the influence of current and historical stress on health outcomes for AI/AN people. In this model, risk factors (e.g., historical trauma, discrimination, and contemporary traumatic experiences) contribute to psychological stress that increases the risk of poor mental and physical health outcomes. Protective factors include cultural buffers (e.g., spiritual practices and cultural identity), which are theorized to lessen the impact of these risk factors on health.
Just as historically unresolved grief impacts health, grief from current losses can also have far-reaching health effects. After the death of a loved one, many people go through a painful grieving process in which the intensity of grief-related distress decreases over time (Jordan & Litz, 2014). Experiences with grief are shaped by cultural norms, religious and spiritual practices, and personal experiences of loss (Cable, 1998; Clarke et al., 2003). While most people will experience a difficult mourning period, some may experience an abnormal grieving process that leads to debilitating psychological distress, which is known as complicated grief (Prigerson et al., 2009). Complicated grief represents a deviation from cultural and societal norms for grieving, either in the length or intensity of the symptoms experienced (Lichtenthal et al., 2004; Prigerson et al., 2009). Symptoms of complicated grief include a persistent yearning for or difficulty accepting the death of a lost loved one, isolation from social situations, and reduced ability to experience positive emotions (American Psychiatric Association, 2013). The risk of developing complicated grief is highest for individuals who have provided palliative care for a loved one, parents who have lost a child, and people who have experienced the sudden or traumatic loss (e.g., suicide, homicide, and accident) of a loved one (Lundorff et al., 2017; Shear & Gribbin Bloom, 2017). Due to high rates of premature mortality and the sudden or traumatic loss of life experienced by many AI/AN people, complicated grief may be a pressing health concern. However, it is unknown whether the symptoms of complicated grief shown in other populations also apply to those in AI/AN communities.
In reviews of bereavement-associated health problems, elevated rates of chronic illness and pain, chronic illness, and mental health problems such as depression, posttraumatic stress disorder (PTSD), insomnia, suicidal ideation, and addiction were found in people experiencing complicated grief symptoms (Kristensen et al., 2012; Stroebe et al., 2007). The health-related outcomes of complicated grief are especially concerning, as they closely align with many of the top causes of death in AI/AN communities. It is important to note that many negative health outcomes (e.g., depression, suicidal ideation, and substance use) associated with complicated grief and historical trauma overlap. Historical trauma may increase the risk of developing complicated grief from a recent loss. This is because new losses may serve as reminders of collective losses and contribute to greater distress. While this relationship has not yet been studied, research on other mental health conditions revealed that people with depression are more likely to develop PTSD if they experience a traumatic event (Nichter et al., 2019; O’Donnell et al., 2004). Therefore, people with underlying historical grief may be more likely to develop complicated grief if they experience the sudden or traumatic loss of a loved one. In context with the ISCM, both historical trauma and complicated grief contribute to psychological stress in AI/AN communities, potentially leading to poorer health outcomes associated with elevated stress levels (Walters & Simoni, 2002).
The collectivist cultural orientation common in Native communities may also influence experiences with grief. Kinship-based relationships expand the bounds of familial relationships to include not only those based on biological connections but also communal and cultural ties (Mohatt et al., 2004). Therefore, the loss of one person may have far-reaching effects on the entire community. As posited by the ISCM, extended kinship networks can provide increased social support and connection to cultural practices to help buffer against the negative effects of grief (Walters & Simoni, 2002). However, for AI/AN people, having a larger network of relatives also translates to additional losses of loved ones. For example, it is estimated that AI/AN people experience one to two significant deaths each year. In contrast one to two deaths occur every 10 years in non-Native populations (Dankovchik et al., 2015). This is not to say that the risks of wide-reaching social connections outweigh the benefits; in fact, social support is crucial for coping with stress and promotes improved mental health (John-Henderson & Ginty, 2020; Roh et al., 2015; Stumblingbear-Riddle & Romans, 2012). It does mean, however, that AI/AN people with large social networks of loved ones are at increased risk of experiencing numerous significant losses and, therefore, of developing complicated grief symptoms.
Current Study
The current study was conducted with the aim of understanding both the perspective of AI community members on grief and its connection with health inequities. This study was conducted at the request of AI community partners working with the research team on a longstanding community-based participatory research (CBPR) project focused on substance use and resilience (Skewes & Blume, 2019). When assessing drug and alcohol use among people with current substance use problems, community partners identified the death of a loved one or the anniversary of a death as a relapse risk. Further, they viewed grief and repeated losses related to death as having a significant negative impact on individual and community wellness. Thus, the community partners suggested adding a measure of complicated grief to our team’s assessment protocol. Upon conducting a literature search to locate an appropriate measure of grief, we found none that were developed or tested with AI/ANs. While the concept of complicated grief resonated with the community, our partnership determined that existing measures were not culturally appropriate. Therefore, we decided to develop a new measure of complicated grief to be used in research on health disparities involving AI/AN people. The current study, which adopts a qualitative interview framework, represents the first phase of our measure development project. We conducted interviews with 12 AI adults from a rural reservation community to understand normative grieving patterns, symptoms of complicated grief, and respondents’ views on the link between grief and health.
Method
Participants
Participants were recruited by the third author, a tribal member of the community. Due to her extensive social connections in the community, she was familiar with the prospective participants and knowledgeable about their experiences with loss and grief. Inclusion criteria included self-identifying as AI, being at least 18 years old, and having experienced a significant loss with a difficult grieving process. Participants were not screened for complicated grief symptoms. However, all participants reported experiencing difficult or prolonged grief that may reflect complicated grief. Participants were encouraged to share information about the study with family and friends, with additional recruitment occurring through word of mouth.
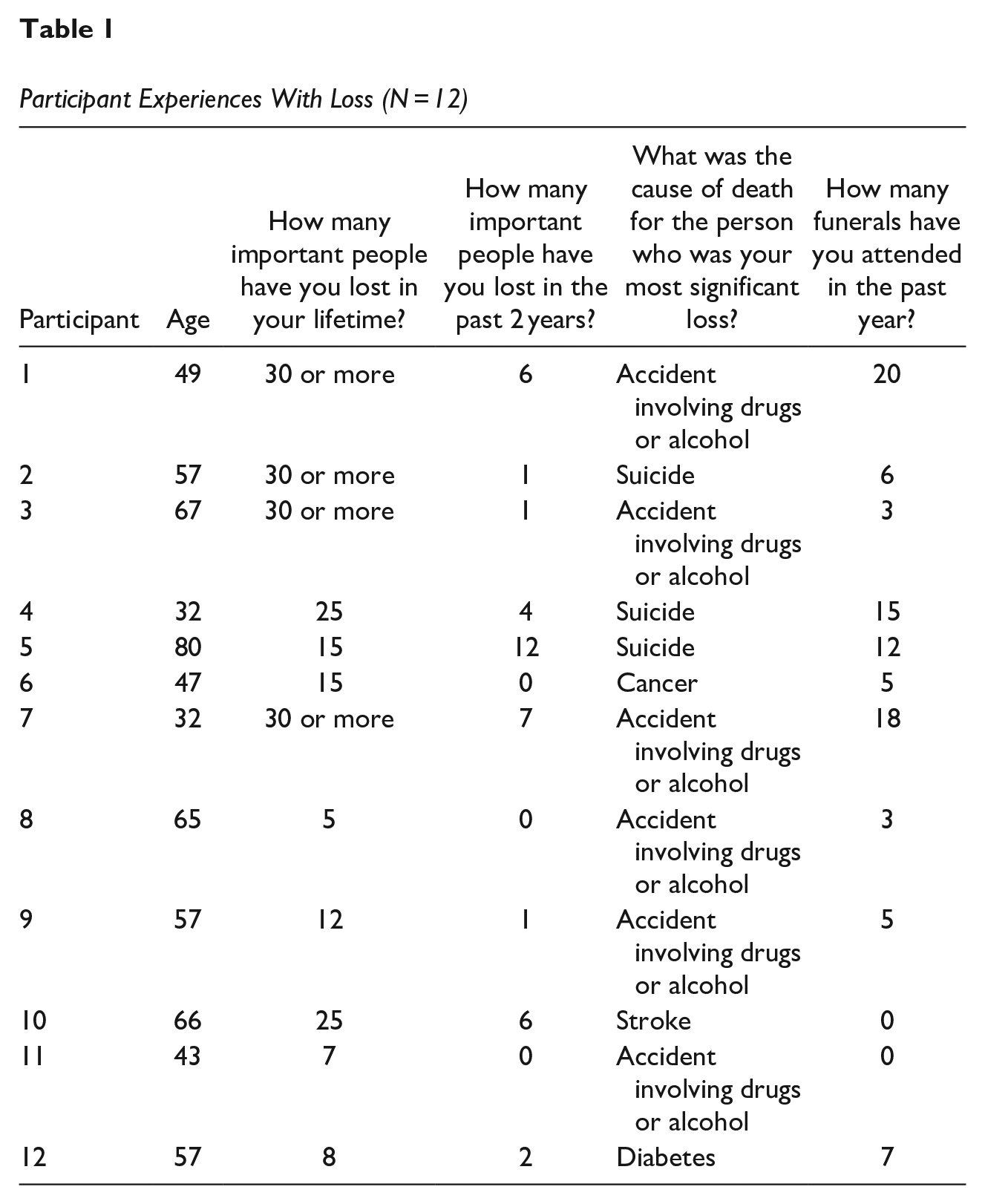
The final study sample included 12 AI adults from a rural reservation community in Montana. Participants ranged in age from 32 to 80 years (M = 54.33, SD = 14.46) and included women (n = 7, 58.3%) and men (n = 5, 41.7%). Education attainment in this group was high, as participants reported having some college education (n = 3, 16.6%) or a college degree (n = 9, 75.1%). Participants had extensive experience with grief and loss (see Table 1). Most of those in the sample (n = 9, 75%) reported that in the past 2 years, they lost at least one person with whom they were close. Participants also reported having a strong connection to their culture, participating in traditional spiritual ceremonies at least once a month (n = 10, 83.3%), and relying on their Native culture for guidance in times of uncertainty or distress (n = 10, 83.3%).
Participant Experiences With Loss (N = 12)
Materials
The first and fourth authors developed the semi-structured interview protocol based on their knowledge of the research topic and the extant literature on complicated grief. They worked with the third author to edit the protocol based on her lived experience as a tribal member who had endured many significant losses. Participants were first asked general questions about their experiences with loss, including the number of people they had lost recently (e.g., “How many important people have you lost in the past two years?”), the impact of these deaths (e.g., “Of these people, whose death has been the hardest for you to deal with?”), how many recent losses they had grieved within their community (e.g., “How many funerals have you gone to in the past year?”), and the impact of COVID-19 on their grieving process (e.g., “How has COVID affected proper grieving?”). Information was gathered about cultural beliefs and practices surrounding grief and loss. Specifically, participants were asked general open-ended questions about loss (e.g., “What are [your culture’s] traditions and rituals for honoring someone who passes?”) and more specific questions about grief (e.g., “What cultural strengths/traditions help people handle grief?”). Participants were asked about health problems associated with grief (e.g., “How does grief affect your health?”). They were also asked about the healthy and unhealthy strategies used to cope with loss and grief (e.g., “What makes grief harder to cope with?” and “How do people express/experience grief in a good way?”).
Procedure
Before data collection, all study materials were approved by the Tribal Institutional Review Board (IRB) and that of the university. Participants were invited to participate in one-on-one Zoom interviews about their perspectives on grief and loss. As they occurred in the fall of 2020, the interviews were conducted via Zoom to reduce the risk of COVID-19 exposure both for community partners and the research team. All participants were informed that the interviews would involve discussions about death and grieving and, thus, that they should participate only if they wanted to discuss these sensitive topics. Participants reviewed an informed consent form and authorized video and audio recordings of the discussions, which were later transcribed verbatim and de-identified by trained research assistants. Participants provided verbal consent for the interviews, which lasted approximately 1.25 hr (M = 1 hr 11 min, SD = 19.86 min). At the end of the interview participants were debriefed and compensated with a $35 gift card.
Positionality and Trustworthiness
Interviews were conducted by the first author, a non-Native female graduate student researcher who was raised in a rural Montana community and had worked on previous research projects on this reservation. The interviewer was trained in CBPR methods and ethics, as well as clinically relevant and culturally appropriate interviewing techniques (e.g., reflective listening using the spirit of motivational interviewing; Venner et al., 2006). The interviewer was supervised by the fourth author, a non-Native health disparities researcher who had a longstanding relationship with and ongoing collaborations in this Native community (Skewes & Blume, 2019; Skewes et al., 2019, 2020). The third author, an AI female Elder, provided a Native perspective to the research team while helping to develop the interview protocol, recruit participants, and critique and approve the codes generated by the coding team. Additionally, the research team included five advanced undergraduate psychology research assistants, all of whom were women of European descent.
As the coding team comprised six non-Native individuals, it was important to educate coders on the history and manifestation of social and health inequities in AI/AN communities as well as Native resilience. This was accomplished through assigned readings and weekly discussions across one academic year before the team engaged with the data. The team members also discussed how their privilege as White, educated females could shape their perspectives as researchers, leading to potential biases as coders. They also considered how their identities and positions as outsiders may shape their interpretation of the data. The coders engaged in memo writing to record their reactions to the data and information that influenced the way they viewed it. When coding was completed, the third author reviewed the themes to ensure the data were handled respectfully and that it accurately represented the participants’ experiences with grief.
Data Analysis
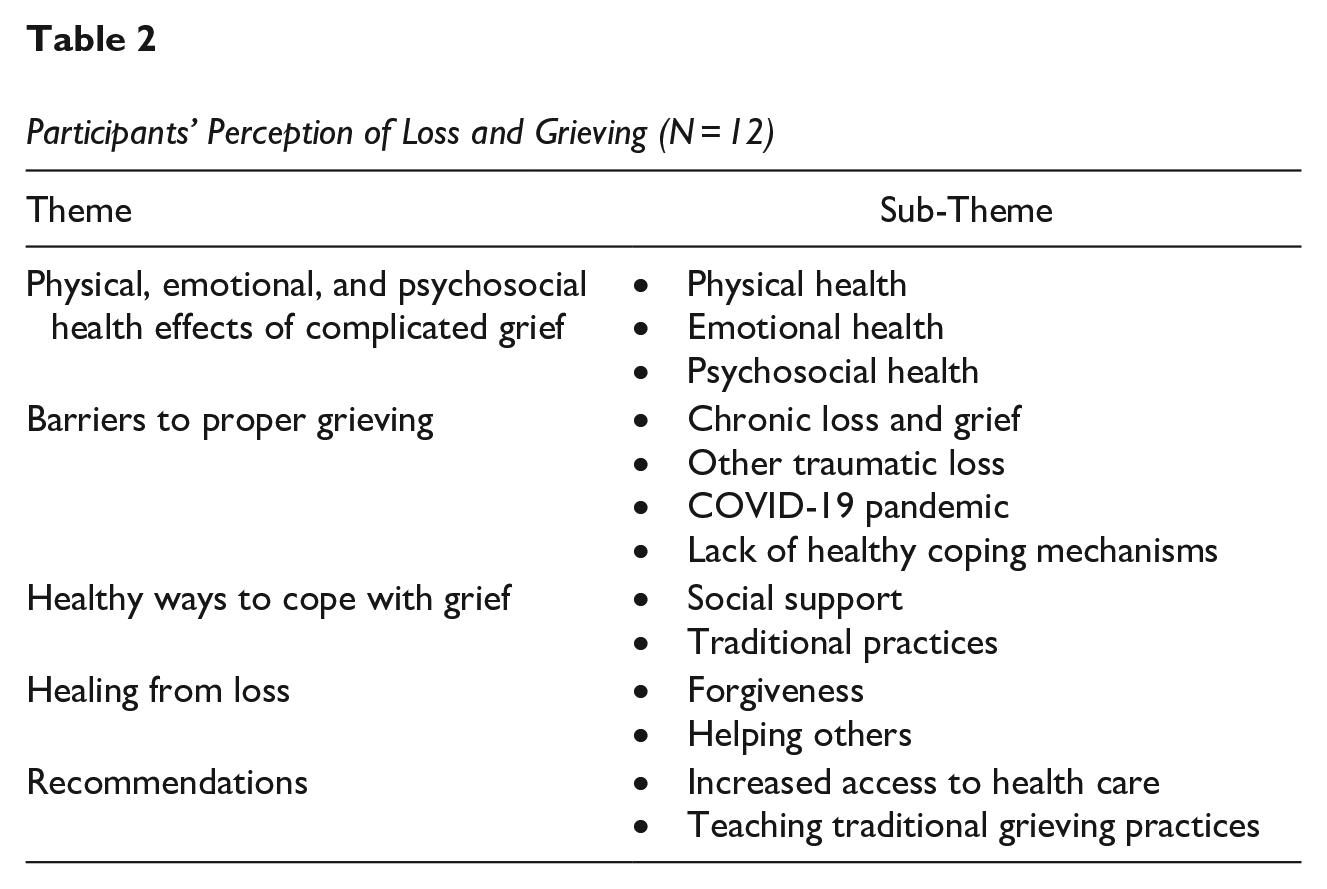
Thematic analysis techniques, which emphasize identifying, analyzing, and interpreting patterns within qualitative data, were used to identify themes related to the experience of grief and the association of complicated grief with health outcomes (Braun & Clarke, 2006). The coding team did not use software to code the data. Instead, coding was performed by hand. The team met weekly over two academic semesters to conduct the coding. First, the team members worked to familiarize themselves with the data by transcribing the interviews and reading each transcript. Coders were then assigned the same two interviews and performed line-by-line coding; then, they generated an initial list of thematic categories. They were encouraged to memo any thoughts or feelings that the interviews had invoked, similarities and differences noticed between the interviews, and similarities or differences found between the data and the research articles read and discussed in the previous year. In the next phase of analysis, our team collaboratively refined the initial thematic categories for use. Research assistants reviewed the remaining transcripts using the initial code list. They noted when codes needed revision or when new ones were needed. Through weekly meetings, our team revised the code list until we reached an agreement. Team members then used this final list to code each interview line-by-line and to identify quotes that best reflected the thematic ideas. Coding discrepancies were rare; when they occurred, they were discussed by the team and resolved by consensus. Final themes were approved by community partners as being accurate representations of experiences with grief. See Table 2 for the final theme list.
Participants’ Perception of Loss and Grieving (N = 12)
Results
Participants described the effects of grief, including physical, emotional, and psychosocial effects. They also discussed ways in which grief contributes to negative health outcomes. Barriers to proper grieving were also identified and were perceived to exacerbate complicated grief symptoms and amplify the negative health effects experienced after a loss. Despite the burden of repeated losses and barriers to proper grieving, participants could identify signs of healthy coping and healing. Participants also provided suggestions for ways to address complicated grief in their communities. Emergent themes are presented in Table 2.
Physical, Emotional, and Psychosocial Health Effects of Complicated Grief
Participants reported experiencing grief-related symptoms that had a negative impact on their physical, emotional, and psychosocial health. This is reflective of findings in the literature showing that people who experience complicated grief symptoms are more likely to require medical care for chronic physical health problems (e.g., hypertension, heart disease) and mental health problems (e.g., depression, PTSD; Kristensen et al., 2012; Stroebe et al., 2007).
Physical Health
Participants described grief as manifesting in acute physical aches and pains, loss of appetite, feelings of heaviness or a weight on the body, memory loss, difficulty breathing, and other somatic symptoms (e.g., rashes). For example, participant six stated, “It [grief] feels like a huge weight on your chest, like it’s hard to breathe. It’s a physical feeling. It’s a physical weight. You lose sleep; you lose train of thought.”
Participants linked complicated grief symptoms with other health problems and chronic illnesses affecting their communities, including insomnia, hypertension, heart disease, diabetes, and cancer, saying, “When we grieve, we might turn to substances, maybe it’s in food, or we stop being physically active. We become heart-diseased people, or we become diabetic people. It has a long-term effect; you can see a distinct physical difference” (P12). This is especially concerning, as illnesses related to diabetes and heart disease are several of the leading causes of death in AI/AN communities.
Participants also discussed the role of substance use as a contributing factor to the deaths of their loved ones as well as a health concern for grieving relatives. They expressed frustration with what seemed to be a perpetual cycle of loss, grief, and substance use. Participant eight stated the following: Just like my nephew, they all started drinking. . .I was just so mad. I said, “No! You guys quit drinking!” That’s why he is gone. . . It’s no good for you, physically. And I got so mad at my son when he started drinking ‘cause of this. I said, “Think about what you are doing; [my nephew] died because he was drinking.”
Emotional Health
Participants also described intense emotional effects of grief, including depression, anxiety, loneliness, guilt, numbness, anger, aggression toward others, feelings of “going crazy,” and hopelessness. Participant nine discussed how her feelings of grief overwhelmed her and how she feared for her well-being due to the rapid deterioration of her mental health following the sudden loss of a loved one, saying, “I felt like something very serious was going to happen. So, I went to my husband; I said, ‘I’m going to lose it; I’m going to go nuts.’”
Feelings of anger and aggression from the participants toward a person who passed and their family or community members who tried to help them grieve were frequently reported. When discussing the loss of his brother, participant one said the following: I’m pissed at him for doing exactly what I told him was going to happen: drinking and driving. We went about three weeks without saying a word to each other, and that kills me. I am just pissed and bitter and just want to tell him, “You left us all here, you know, in this hell.”
Participants also discussed feelings that were similar to survivor’s guilt. They also experienced guilt over the state of their relationships with loved ones who passed, saying, “I feel guilty that my brother passed the way he did. I sometimes feel guilty, like maybe I should have done more; maybe. . . I should have been more involved with his life. . . I could have helped (P7).”
Psychosocial Health
In AI/AN communities, close kinship networks create wide-reaching social support groups outside one’s biological family. This social support system helps people manage grief; however, certain participants reported disengaging from this support when experiencing extreme distress and grief. This disengagement from community support provided notable psychosocial effects, including fear of relying on others and a feeling of being unsure how to function in healthy relationships. Participant two discussed how the loss of her son to suicide changed the way she engaged with cultural practices such as funerals and supporting grieving community members: In our culture, you are supposed to bring food, and we sit with families. You don’t have to talk. You just sit there to share their grief, and let them know you care. Because of my son, I try to avoid funerals. If it is somebody that I know, and it hurts me badly, I try to avoid them. I won’t even go through the process of taking food.
This can lead to more isolation and loneliness. Participant six described becoming “ultra-independent” after losing the person who had been their primary source of support: I don’t want to depend on anybody now like I depended on Grandma for everything. I don’t want to deal with that anymore, so I don’t. That’s a bad thing. I think growing up, I was, I was solo, ultra-independent—like, I’m not going to depend on you for anything, and that just puts up a lot of barriers. Because of this, loneliness stuck around for a long time.
After a significant loss, this person refrained from seeking social support from other community members to avoid further pain from additional potential losses. Thus, the fear of losing someone close again led them to isolate themselves from community support sources, contrary to cultural traditions and practices and potentially prolonged their grief.
In sum, participants viewed symptoms of complicated grief as having a negative impact on existing physical, mental, and social health. Grief-related distress was also viewed as contributing to social dysfunction by creating distance between individuals and their community and culture following the loss of a loved one.
Barriers to Proper Grieving
Participants described experiences and circumstances that made the grieving process more difficult and increased the likelihood of health-related issues. These factors included chronic grief from repeated losses: unresolved trauma related to violent and/or premature deaths, loss of children or experiencing loss at a young age, cultural loss and historical trauma, disrupted cultural and spiritual practice due to the COVID-19 pandemic, and a lack of healthy coping mechanisms.
Chronic Loss and Grief
Participants had extensive experiences with grief and loss (see Table 1). Notably, 75% reported at least one significant loss in the past 2 years. Chronic grief was viewed as an extremely common experience in this community, which made processing repeated losses challenging: I think grief is compounded here because we have so much of it. . . . Our communities and our families are so large and interconnected that oftentimes, we have just constant grief. . . You know, culturally, we have that year where we process that [grief], and sometimes that year, there are four or five deaths that you are trying to process [at one time]. (P4)
Experiencing frequent losses of important people was common in this sample, half of which reported losing more than 20 important people in their lifetimes (n = 6; 50%). Loss was so pervasive in the community that participant seven said, “It’s sad to say, we’re almost like professional mourners.”
Participants expressed a great deal of emotional fatigue attributed to continually grieving the loss of people in their community. Many described being in a constant state of grief, lacking the proper time or space to process feelings, and thoughts related to a loss before another occurred. Participant six described becoming numb to the pain of additional losses: Like, I talked at five funerals this year; those are not even my relatives. I’ve become so immune to it, and it’s hard to cry for these people anymore. Like, I know they’re in pain; I know they’ve lost the love of their life. . . I’ve become hardened to it.
Other Traumatic Loss Experiences
In the discussions about the loss of a loved one, participants often brought up losses not directly connected with death. They spoke of the loss of children to the foster care system and the loss of their people to addiction—both of which are tied to historical trauma within this population. When speaking about a family member, participant seven said the following: Her [cousin’s] daughters are in foster care. Then, she has one living somewhere that’s got severe disabilities, and she’s probably lost, like, three to SIDS (sudden infant death syndrome) or miscarriage. She gets sent to [substance use] treatment for 28 days; and, you know, she’s been to treatment, I think, twelve times. . .We have a lot of people going to treatment for 28 days and coming back and using again.
With the disproportionately high incarceration rate of AI/AN populations (Daniel, 2020; Jacobs et al., 2018), participants and their families were often left grieving a loved one lost to the prison system. For example, participant nine said, “There are a lot of other losses I’ve experienced. I have a daughter in federal prison right now, and she’s incarcerated. I grieve the loss of my granddaughter’s mother.”
Historically, AI/ANs have experienced high rates of losing children to foster care and boarding schools (Bombay et al., 2014; Evans-Campbell, 2008; Maguire-Jack et al., 2020). Removal may also leave children alone to grieve without the support of their families or communities. Participant five, who spoke of her time in boarding school, said the following: Most people my age and maybe ten years younger have been in boarding schools and maybe lost someone while we were there and not be able to come home and have the community to grieve with or comfort you. So, I learned to just kind of freeze my feelings.
These experiences appear to be common in older generations of AI/AN people and demonstrate that grief is not limited to current experiences. Rather, it can also manifest as historically unresolved grief from past events.
COVID-19 Pandemic
It is important to note that these data were collected during the COVID-19 pandemic, which caused the deaths of many tribal members and prevented people from gathering as a community to perform the traditional ceremonies needed for a proper funeral. Specifically, participant 12 said the following: We can’t have proper funerals the way that we usually do as our culture. You know, you can’t have the wakes or a lot of the ceremonies that go with the funerals, the moving of the spirit to the next world. . . It’s hard to do those while this [COVID- 19] is going on.
Restrictions implemented during the pandemic greatly affected the community and prevented traditional ceremonies from occurring. Ceremonies are an important component of grieving in this community, as they bring peace to family members and are thought to prepare the deceased’s soul for the afterlife. Therefore, the community’s inability to participate in these ceremonies was thought to exacerbate complicated grief.
Lack of Healthy Coping Mechanisms
When participants were asked to reflect on things that made coping with grief more difficult, many identified substance use as a significant barrier to healing in their community. Participants reported that coming together with friends and family to drink was common after funerals. Using substances to cope was seen as a replacement for healthy coping mechanisms. Participant six relayed the following: I just thought that’s what you did, you know. When I was in my late teens, early 20s, when we lost someone, we all got together and drank and cried and talked about them, and you know, that’s really not healthy.
Participants believed that using alcohol to cope with loss prolonged the grieving process. As a result, a perpetual cycle of loss, grief, and substance use would ensue, making it difficult to process grief and heal: [Being] under the influence allows you to feel good for a minute, but the minute that drug or that alcohol is gone, then it’s intensified, and so, what do you do? Go right back to it again because you don’t want to feel. I think that’s the hardest piece. (P9)
Participants also discussed other behaviors, such as using food, self-harm, or risky sex to numb the pain of grief, as barriers to healing. When asked about healthy ways to cope with grief, participants had greater difficulty identifying healthy coping strategies than unhealthy ones. As participant eleven shared, “As far as mourning and coping, I don’t know if people even know how to mourn; they don’t know how to cope, and you don’t know how to mourn the loss of somebody.”
Another participant indicated that people need a “grief guide” to help them navigate grief and mourning. It was seen as the responsibility of those who had experienced and coped with their loss to help others who were struggling. The participant suggested that Elders or other cultural and spiritual leaders in the community would be well suited for the role of grief guide or mentor. These people could teach traditional ceremonies around grief and tell stories of the afterlife to comfort those who are grieving.
In sum, participants discussed grief as it related to death as well as historical trauma, incarceration, and loss of children to foster care or boarding school. These experiences can compound grief from new losses and make coping with distress more difficult. The COVID-19 pandemic made coping with grief even more challenging, as it interfered with traditional ceremonies to honor the diseased and caused more losses. Due to the prevalence of loss and grief in this community, participants noted that most people did not know how to cope with grief healthily and often turned to substances to numb their pain.
Healthy Ways to Cope with Grief
When discussing healthy ways to cope with grief, participants stressed the importance of social support, finding healthy ways to express emotions, and participating in traditional cultural and spiritual practices. This community does have services, such as spiritual guidance offered by churches, Elders, and cultural leaders, as well as behavioral health assistance provided by the Indian Health Service (IHS) clinic, to help grieving people. However, these services are not utilized by those who experience extreme distress after losing a loved one.
Social Support
Participants stressed the importance of social support as a healthy coping strategy, suggesting that people should turn to Elders, friends, or other trusted individuals to discuss their grief. Processing and “sitting with” grief-related emotions with a trusted confidant was seen as one of the best ways to cope with negative feelings. For example, participant 6 said, “If you feel angry, sit with it. . .It can’t stay forever. You have to feel anger, feel sadness, feel loss. The more we don’t sit with it [grief], the more it stays. It just stays there forever.” However, participant four emphasized that when selecting a confidant, it was important to ensure that the person was able to emotionally handle the conversation: I think it’s important to find people you feel comfortable talking to. When I say that, that comes with a lot of heaviness, so it’s always, like, making sure that you ask permission to unload onto them. . . So just kind of talking through it, not really needing direction but just having a space to get out what’s inside.
To help with their day-to-day tasks certain participants relied heavily upon friends, family, and their community. After experiencing a loss, people reported feeling lost and helpless and struggled to function and care for their basic needs. Participant seven said, “I won’t do anything for days; I won’t clean my home. . .Sometimes, I won’t even cook. . . I have three daughters, so I’ll tell my mom, ‘Is it okay if the girls come over for dinner?’” Friends, family, and community members were seen as important sources of support, offering people the time to cope with their losses without worrying or feeling guilty about falling behind on other responsibilities or life tasks.
Traditional Practices
Finding comfort in traditional beliefs and stories about the afterlife was a common theme among participants. They believed that while grief could become all-consuming, it was important to remember that ancestors now surrounded the recently deceased and that the person’s absence in the life of the surviving loved one was temporary. Participant 8 said the following, I didn’t know that it [grief] was going to go away when I was going through it, but I knew the Creator reminds us there is happiness over there. Your time here on Earth is just a twinkling of the eye, and there is another place to go to be with your ancestors sitting around the other side of the camp. They are all probably up there joking around waiting for me.
Participants also felt that cultural practices served as a guide for grieving. Traditional cultural and spiritual ceremonies gave people instructions that they could follow to honor and grieve a loved one. The ceremonies include tangible steps to help prepare loved ones for the afterlife and guidelines for how the community should support a grieving family: Our cultural ways do help in grieving and walking through that loss. My brother, the night he passed away, didn’t have an Indian name. We had a naming ceremony for him that night and had a pipe ceremony for him. We leave food offerings just so they have nourishment and know that everything is okay. I had a ceremony where I cut my hair off, and our belief is that the hair signifies mourning but can also help them [deceased loved one] journey on the other side. We have memorial feeds for our family members and giveaways, and you honor him by giving stuff away to the people and feeding people in the community in his memory. It all brings comfort. (P4)
In sum, engaging with one’s social support network and culture was viewed as helpful in coping with loss. Using the available resources in their community or kinship networks gave people a sense of being supported in feeling, expressing, and processing their grief.
Healing From Loss
Despite identifying numerous barriers that made grieving the loss of a loved one difficult, participants were also able to recognize signs of healing within themselves. Signs of healing from grief included coming to terms with the loss and finding a way to live a “normal” life again. Participants felt they could slowly find joy in life and hobbies again after a loss, which reflected healing.
It doesn’t look like you get it all right, day one, but we begin to try, and we try to return, like, to sew, or you did beadwork or whatever it is—you like to golf, play guitar, play the music, you know. (P1)
Forgiveness
Participants stressed the importance of coming to terms with the anger or frustration that they felt toward the person they had lost. This could prove especially difficult for people who had lost a loved one to suicide or other circumstances perceived as self-inflicted. When speaking about the suicide of her son, participant two shared, “I, you know, I had to forgive him. I carry a rock. . .I just like to carry it around. And when I get upset, I hold it and just remember, okay, I forgave him.” Through forgiving a loved one who passed, participants reported focusing less on negative memories and more on positive ones about the person.
Immediately following a loss, participants experienced difficulty reflecting on memories of the loved one, which evoked feelings of extreme distress, anger, and hopelessness. Despite the negative feelings memories could evoke, participants stressed the importance of focusing on positive thoughts related to their loved ones. Participant three shared, “I think in the beginning, it’s hard. . . But you want to keep those happy memories forever because your memories fade. You know. . . you wish to go back to those happy times.”
Once they found happiness in memories and celebrated the person’s life, participants began the process of forgiveness and healing. Participant 8 said, “I didn’t dread the holidays. I didn’t dread [the anniversary of their death], you know. I celebrate their birthday, and I make it a happy thing.” Embracing forgiveness, returning to one’s normal activities, and finding it easier to reminisce on happy memories of a passed loved one were seen as signs of healing.
Helping Others
Along with returning to activities they had enjoyed prior to their loss, certain participants reported finding new purpose and meaning in life as they healed from grief. They felt a duty to help others in their community who were struggling with loss: I feel like [you are healing] when you’re able to be there for somebody else regardless of your own things. I am very thankful that I get to honor and help my loved ones grieve. I can sing [at funerals] . . .I can write obituaries. . .I know how to organize a funeral and how to plan a feed and can help them. (P4)
In sum, participants were able to identify inner healing once they returned to their previous ways of living before losing a loved one. For many participants, this return to normal included finding ways to forgive their loved ones and focus on happy memories. Participants also expressed that once they had processed their grief, they could help others in the community who were struggling with loss.
Recommendations
Throughout the interviews, participants stressed the need for tangible action to help AI/AN communities manage the health consequences of grief and to prevent early mortality. Participants also stressed the importance of providing culturally informed care to communities as traditional Western medical treatments were not always viewed in a favorable light.
Increased Access to Health Care
In many AI/AN communities, access to health care is limited, contributing to early deaths and leaving people without professional help for coping with loss. Participants in this study lived in a geographically isolated reservation with limited healthcare options: a small clinic operated by IHS; a small rural hospital; and the nearest hospital capable of managing complicated health conditions, which was located 5 hr away. Additionally, available mental health services for people struggling with grief were limited. Participant 12 said the following, We don’t have the mental health support here. You know, we have one or two providers, but they’re swamped. There’s no support for people grieving. You can’t just call up the grief counselor and say, can I make an appointment?
To receive formal mental health services, people in this rural community must drive over 300 miles. Participant 5 noted, “There is really good care available in other places, but not if you don’t have a good insurance policy.” In addition to needing insurance to receive services, community members must also be able to take time off work, have money for transportation, and for certain individuals, find childcare. Thus, traveling for mental health care is nearly impossible for most community members. This emphasizes the need for access to quality mental health services in AI/AN communities and for grief counseling on reservations.
Teaching Traditional Grieving Practices
In addition to a need for increased access to mental health care, teaching the traditional practices and ceremonies associated with loss and grieving is also important, as emphasized by participant 12: More people are coming to me to learn the traditional ways you know. They’re coming to me now because my mom and grandma passed on what we do when we bury them with feathers or not or how we bury them, or how we dress them. They’re coming for me more for that, some of the relatives, who opened my eyes a little. To realize that when the others move on, you know, take on those responsibilities [of educating] within the culture on some traditional ways around death, falls to us.
This highlights the need to learn and share traditional spiritual and cultural practices as a way of supporting healing from grief.
In sum, participants identified the need for greater access to mental health services in their community. They also noted that it was important to include traditional spiritual practices in treatments for complicated grief. Due to their high rates of premature mortality, AI/AN communities disproportionally carry the burden of complicated grief without having adequate services to support community needs. Action is required to address health inequities, which will involve increasing access to culturally appropriate care and ensuring that AI/AN communities have adequate resources to help their people cope with the loss of a loved one and heal from grief.
Discussion
The current study aimed to explore loss and grief as both a cause and a consequence of health inequities affecting Native communities. Given the high early mortality rates in AI/AN communities, it is common for their members to grieve the loss of someone close to them. We acknowledge that developing an emic view of the differences between normal and complicated grief is necessary. This will allow for a determination to be made about whether someone’s grief lies outside what is normative in the culture. It is important to develop a deeper understanding of the cultural norms surrounding grief to determine when someone may need extra support. This study is a first step in understanding the normative and complicated grieving experiences of AI people living in a reservation-based community. For example, among AI people in this community, a common facet of the grieving process included having visions of and talking with a deceased loved one. It was viewed as an honor to have a loved one appear in dreams or during traditional ceremonies. This differs from complicated grief research conducted with non-Native populations that view aspects of communication with the deceased as maladaptive (Kristensen et al., 2012; Stroebe et al., 2007).
Once there is an understanding of normative grieving practices, researchers can better identify abnormal grieving patterns among AI/AN people. In this study, participants reported experiencing high rates of loss, which they viewed as detrimental to their physical and mental health symptoms related to abnormal grief. Native communities are disproportionately impacted by high mortality rates associated with chronic illnesses (Indian Health Service, 2018). While grief interventions and mental health resources are greatly needed, it is also necessary to look upstream at the health inequities driving high mortality rates in AI populations (Sequist, 2017). This suggests a cyclical relationship between health inequities, high mortality rates, and complicated grief. Improvements in mental and physical healthcare systems are desperately needed in AI communities, especially those located in rural areas, to improve health outcomes and decrease mortality rates (Goodkind et al., 2010; Lillie-Blanton & Roubideaux, 2005).
The high rates of loss and the negative physical, emotional, and psychosocial consequences reported in this AI community indicate that grief-related therapeutic interventions are necessary. Empirically tested and supported treatments are available for complicated grief (Shear, 2010, 2015; Shear & Gribbin Bloom, 2017). However, these treatments have not been tested or validated with AI/AN people. To our knowledge, the only intervention designed to treat symptoms of grief among AI/AN people is the Oyate Ptayela: Return to the Sacred Path program developed by Brave Heart (1999a, 1999b). This intervention was originally designed to address symptoms of historical trauma and historically unresolved grief. Once participants were taught traditional grieving practices and connected with other people from their community, they reported a reduction in historical trauma and grief symptoms.
Participants in this study raised concerns about the preservation of traditional cultural and spiritual practices that surround celebrating the life of a loved one and coping with grief in a healthy way. Tribal communities were greatly impacted by the COVID-19 pandemic, seeing some of the highest mortality rates in the country (Williamson et al., 2021). This was especially true of people over the age of 65 and those with a preexisting chronic illness (Williamson et al., 2021). The loss of life associated with COVID-19 in AI/AN communities was especially devastating, as the loss of traditional cultural and spiritual knowledge coincided with the deaths of many Elders (Williamson et al., 2021). While there have been community-driven efforts to preserve Native cultures, concern exists that cultural knowledge is lost as Elders pass. Efforts are needed to develop culturally grounded interventions imbued with the lessons and knowledge of past generations, which can preserve the traditions and ceremonies around grieving and share traditional cultural knowledge, spirituality, and practices more broadly.
Limitations and Future Directions
The generalizability of this study may be limited, as only 12 people from a rural reservation community were interviewed. For example, AI people from other reservations or urban areas may have different experiences with loss and, therefore, different ideas about how to cope with and process their grief. The demographics of the sample also limit generalizability, as the mean age of participants was 50 years old. The ages of the participants could influence their experiences with loss as they may have experienced more loss than younger groups and had more time to learn to process and heal from grief. Furthermore, those who were included in the sample reported greater education attainment than is typical on studies in this community, which may have influenced the responses of the participants.
Additionally, these data were collected during COVID-19, which greatly impacted AI/AN communities. People may have experienced more recent losses due to COVID-19 than if the data had been collected before the pandemic. The fact that funerals and traditional ceremonies were disrupted by the pandemic was also on the minds of participants’, which may have influenced the way they discussed grief. Another possible limitation was the use of televideo for conducting interviews—a decision made to protect participants from exposure during the first wave of the pandemic. Most of the interviews took place in participants’ homes, which led to occasional internet connectivity issues and interruptions. While participants did offer important insights into their experiences with loss and grief, what they shared may have differed if the interviews had been conducted in person or outside the home.
The research team worked closely with AI community partners throughout the study. However, data collection and analyses were conducted by non-Native researchers who had been vetted by the community partners. Despite years of previous successful collaborations, the research team members were in the position of being seen as outsiders, which may have influenced the selection of participants in this study or impacted the knowledge they shared. In addition, it may have affected the data analysis and interpretation of findings. However, having the findings reviewed and vetted by the community partners and approved by the tribal IRB helps to mitigate some of this concern.
Future research should focus on recruiting samples of AI/AN people from different areas in the United States so that researchers can explore possible cultural or regional experiences with grief and loss. A greater age diversity in future samples will also allow researchers to understand experiences with grief across the age spectrum. Efforts are also needed to involve more Native researchers in data coding and analysis. More Native representation on the research team could improve the quality of data collection and analysis.
Further research on complicated grief with AI/AN people is needed to enhance understanding of the complex relationships between health inequities, complicated grief, and historical loss. A need also exists to assess the cultural appropriateness of existing complicated grief interventions to determine what, if any, cultural adaptations are required to reflect the experience of AI/AN people with loss and grief and to increase the acceptability and usefulness of these interventions for Native communities. In addition to therapeutic grief treatments, implementing a combination of interventions to address health inequities and grief in AI/AN communities could help mitigate the impact of grief and loss on an individual’s physical and mental health.
Conclusion
Disproportionately high mortality rates among AI/AN people leads to chronic, complicated grief in Native communities. Participants reported many barriers to healthy grieving and linked chronic, complicated grief with the development of multifaceted health problems, exacerbating health disparities and leading to more losses and grief. This suggests that the relationship between AI/AN health inequities, chronic grief, and barriers to proper grieving is cyclical and warrants further examination and intervention. A return to traditional cultural ways of grieving and supporting community members who experience loss has the potential to disrupt the cycle and improve health outcomes in Native communities. Future research is needed to implement and to evaluate culturally responsive, evidence-based complicated grief interventions.
Footnotes
Acknowledgements
The authors wish to thank the project’s Community Advisory Board and the study participants for their valuable contributions.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This manuscript includes findings presented in the first author’s doctoral dissertation but have not been disseminated elsewhere.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 5P20GM104417–02.