
Abstract
Low-income children are among the most affected by unintentional injuries. Although these injuries are preventable, outreach to low-income families in Hispanic and rural communities can be challenging. Community Health Workers (CHWs) are effective partners in reaching these populations. This study sought to determine whether a CHW-led intervention would reduce common hazards that increase the risk of unintentional injuries in low-income rural Hispanic homes along the Texas–Mexico border. CHWs conducted home visits to assess for injury hazards and distribute safety devices to 47 families with children ages 0 to 5 in five low-income rural border communities. CHWs provided follow-up assessments and support 30 days later. Analyses examined changes in the proportion of hazards from visits 1 to 2, with relative risks estimating the impact of safety devices on hazard reduction. Findings showed a 26.2% reduction in the total number of common hazards present in homes from visit 1 to visit 2 (p < .001). There was a 70% reduction in the overall risk of a hazard being present at visit 2, relative to visit 1 (relative risk = 0.30, 95% CI [0.28, 0.33], p < .001). This study suggests that tailored CHW interventions can reduce home safety hazards. CHWs are well suited to inform hard-to-reach Hispanic and rural populations, addressing feelings of distrust and promoting acceptance of recommended environmental changes. More rigorous evaluations of this intervention strategy are needed.
Unintentional injuries continue to be the leading cause of mortality and morbidity among children ages 0 to 19 in the United States, with a child dying every hour and more than 9 million children treated annually in emergency rooms (West et al., 2021). Additionally, the estimated annual combined cost of fatalities, hospitalizations, and emergency room visits related to the five leading causes of unintentional child injuries—falls, poisoning, drowning, fire/burns, and motor vehicle accidents—was over 300 billion dollars in 2019 alone (Centers for Disease Control and Prevention [CDC], 2021). Most unintentional child injuries result from common and preventable hazards in the home, where children spend most of their time (O’Donnell & Canares, 2021). Young children ages 5 and under are particularly vulnerable as they learn to crawl, walk, and explore their surroundings (CDC, 2012).
Socioeconomic status often impacts unintentional child injuries, as low-income communities are more likely to live in environments with increased hazards (Mahboob et al., 2021). These communities are affected differently, especially in rural areas such as those along the Texas–Mexico border where poverty, lack of health insurance, low English proficiency, cultural differences, and limited understanding of the healthcare system are common (Slemaker et al., 2017). Furthermore, staffing shortages in rural clinics limit access to medical attention, and commuting to the nearest health services can prove difficult due to unreliable transportation as well as poor road conditions (Rural Health Information Hub, 2019).
The Texas–Mexico border region, with a predominately Hispanic population (89%) of 3.4 million people, has some of the poorest and most vulnerable counties in the United States (United States Census Bureau, 2021). Over the last 10 years, the Texas border region has outpaced national growth trends with a population growth of 13.4%, likely driven by immigration and higher birth rates (Texas Department of State Health Services [DSHS], 2020).
Hispanic children in rural Texas border communities have a significantly higher risk for unintentional injuries (Flores et al., 2005). Injury rates might even be higher than reported, given that Hispanic mothers may be less inclined to report their child’s injuries due to distrust of family outsiders or fear of the child being removed from the home (Hendrickson, 2008; Mull et al., 2001). Added to this are government actions regarding immigration that create new barriers for hard-to-reach populations that feel particularly exposed or vulnerable (Smith, 2020). These barriers might be mitigated by gaining the community’s trust through connections that share the language, cultural values and beliefs, and an understanding of the realities of their situations (Smith, 2020).
Although unintentional child injuries remain a crucial public health concern, most injuries are preventable. Parents are generally mindful of the importance of removing hazards, although some may not be fully aware of the risks certain hazards pose or underestimate their child’s vulnerability (Ablewhite et al., 2015). Others perceive injuries as normal, believing the child should adapt to their surroundings through hands-on experiences or teaching the child to discriminate safe from unsafe (Bhatta et al., 2021). However, when parents rely mainly on teaching instead of removing hazards or following recommended safety practices, they might increase the risk of injuries, particularly for young children who may be incapable of or unwilling to follow safety rules (Morrongiello et al., 2004).
Given the role that parental safety behavior plays in preventing injuries to young children, addressing these behaviors is essential (Glanz et al., 2008). Past research suggests that home safety education for parents and caregivers increases positive safety behaviors, resulting in fewer hazards and ultimately fewer injuries (Children’s Safety Network, 2019). Among low-income Hispanic parents, interventions with clear messages and cultural considerations have shown positive results in reducing child injury risks (Garza et al., 2012; Hendrickson, 2005; Setien et al., 2013).
Educating parents on simple home modifications plays an essential role in moderating child injury risks (American Academy of Pediatrics, 2017). For instance, safely storing medications and cleaning supplies out of a child’s reach lowers the potential for poisoning (American Academy of Pediatrics, 2017). The appropriate use of safety devices has also been found effective in improving home safety, such as smoke alarms, outlet covers, nightlights, and drawer latches (Garza et al., 2012; Setien et al., 2013). Usage rates of these devices are suboptimal, however, especially in rural areas where low-income households face difficulties acquiring or implementing such devices (Pressley et al., 2009). Additionally, foreign-born immigrant families may lack experience with certain safety devices in their home country (e.g., smoke alarms or cabinet locks) possibly due to cost or availability, further reducing the likelihood of using them (Gallagher et al., 2009; Hendrie et al., 2004; Mock et al., 2003).
Educational interventions for parents have shown improvements in hazard awareness (Garza et al., 2012; Hendrickson, 2005; Pressley et al., 2009; Setien et al., 2013). Nevertheless, interventions offered outside the home are not tailored to specific needs or environments (Nansel et al., 2007) and tend to rely on participants’ self-reporting, lending to inconclusiveness on the actual removal of hazards and whether safety devices, if offered, are correctly installed or used (Garza et al., 2012; Pressley et al., 2009; Setien et al., 2013). Although self-reporting requires less effort and resources, response accuracy can be unreliable (Hatfield et al., 2006).
Home visits and assessments help parents better understand their home environment and the challenges they face (Garza et al., 2012), and evidence suggests that such interventions reduce injury rates over the longer term (Kendrick et al., 2013). Home visits among low-income Hispanic communities in other parts of the country resulted in significant improvements in safety behaviors (Forster-Cox et al., 2010) and up to 88% reduction in the number of hazards post-intervention (Slemaker et al., 2017), although multiple visits were typically carried out and in some cases weekly over 9 to 15 months (Slemaker et al., 2017). In contrast, home visits were not effective in improving parental safety practices in a low-income, inner-city setting; however, changes could not be measured adequately, as resources constrained the study to one visit. Furthermore, generalizability to other audiences, such as non-English speakers and rural communities, was limited as the lack of culturally adapted materials restricted participation to English-speaking families only (Gielen et al., 2002). For hazard prevention programs to succeed along the Texas–Mexico border, materials may benefit from cultural adaptation to the priority population and geographical location (Hendrickson, 2005).
Community Health Workers
Community health workers (CHWs) are valuable in connecting with low-income populations and closing the gap in health disparities (Uriarte et al., 2014). CHWs are volunteer or paid frontline public health workers who are trusted members of and/or have an unusually close understanding of the community they serve and typically live in (American Public Health Association, n.d.). Their interaction with a community is enhanced through shared beliefs, language, and cultural identity that, in turn, increase the community’s recognition of the CHW and the health issues at hand (Katigbak et al., 2015). To be certified in Texas, CHWs must meet specific requirements (e.g., age 16 or over and completion of a state-certified 160-hr training program) and be recertified every 2 years by completing 20 hr of state-approved continuing education credits (DSHS, 2022).
As trusted members of the community, CHWs have served in diverse programs throughout the United States to inform low-income and minority populations of health risks and connect them with local health services. For instance, a university–public health department partnership in El Paso, Texas hired CHWs to help low-income Hispanic immigrants access breast cancer screenings and address barriers, leading to a 54% completion rate over 15 months (N = 514) confirmed through follow-up phone calls by CHWs (Brown et al., 2018). Another similar partnership in New Mexico worked with CHWs to provide food and fire safety education to low-income Hispanic homes along the New Mexico–Mexico border, resulting in a 73% increase in homes with functioning smoke alarms during the 3-year study (Forster-Cox et al., 2010).
Given the economic, social, and geographic challenges rural communities face—compounded by staffing shortages in rural clinics—CHWs can improve health outcomes by serving as health educators and promoting healthy behaviors (Exemplars in Global Health, 2023). Carefully matching CHWs’ characteristics to program goals and the target population’s values, such as the importance of family in the Hispanic culture, may prove essential (García et al., 2017). Despite the need to reach underserved populations and the unique opportunity CHWs provide, however, there are few culturally and geographically focused home-visit-oriented interventions to increase awareness among low-income parents on child injury risks. Studies carried out among similar populations in the Texas–Mexico border region provide evidence of improved self-efficacy for home safety behaviors (Hendrickson, 2005) and increased hazard awareness, but no evidence of effectiveness in reducing the number of home hazards other than participant self-reports (Garza et al., 2012; Setien et al., 2013).
A needs assessment conducted in 2019 by the DSHS found that child home safety programs led by CHWs were lacking in the Texas–Mexico border region (Office of Border Public Health, 2019). Thus, a partnership was formed between the Office of Border Public Health of the DSHS and the University of Texas Health Science Center School of Public Health (UTHealth) to develop a child home safety intervention.
Theoretical Framework
The health belief model (HBM) (Becker, 1974) provides a conceptual framework to approach injury prevention. HBM suggests that increasing a person’s perceived injury susceptibility and severity leads to preventative actions if the benefits of taking recommended actions outweigh the barriers. Increased participant awareness and knowledge of the seriousness of child injuries and associated hazards can contribute to hazard reduction behaviors. Through an extensive home assessment, CHWs (i.e., trusted individuals) are able to highlight hazards that make the child susceptible to injury and to provide information on the seriousness of the injuries associated with each hazard. CHW-delivered education on the actions required to remove those hazards can then increase participants’ perceptions of the benefits of behavior changes. By providing the skills and tools to remove injury risks, participants would have the self-efficacy to overcome barriers and to achieve a safer environment for their children. Drawing from these HBM concepts, this study sought to evaluate whether CHW-led home assessments coupled with informative materials and prevention strategies would reduce hazards that pose a risk for unintentional child injuries in low-income rural Hispanic homes along the Texas–Mexico border.
Methods
Study Design
This was a non-randomized, one-group intervention consisting of two visits to participating homes: visit 1 was to conduct the initial home assessment, and visit 2 served as a follow-up to assess changes in hazards present at visit 1 and to continue supporting environmental modifications. The intervention was conducted between June and August 2021 in five low-income rural communities along the Texas–Mexico border in El Paso and Hudspeth counties. The population in these areas is 96% Hispanic with 37% of the population living below the poverty level (United States Census Bureau, 2021). Study procedures were approved by the author’s Institutional Review Board.
Participants and Procedures
Fifty homes were recruited as per the study protocol and budget constraints. Of these, three homes dropped out of the study before visit 2 due to work or personal issues, resulting in a 94% retention rate. To be eligible, homes had to be located in one of the five communities and have at least one child 0 to 5 years of age living in the home (Phelan et al., 2011). The majority (59%) had one child 0 to 5 years of age, 29% had two children, and 12% had three children. The mean child age was 2.5 years (SD 1.5 years; range 1 month to 5 years). Participants had to be the child’s mother, father, or caregiver (e.g., grandparent), reside in the home, speak Spanish or English, and be willing to participate in the two-visit assessment. All participants (N = 47) were Hispanic women (45 mothers; 2 grandmothers) from rural, low-income communities. Specific demographics were not collected to avoid resistance from potential participants, as many expressed concern about immigration status or were fearful they had been reported for some wrongdoing. To reduce these concerns, study personnel visited locations that convey trust and respect (e.g., daycares) to explain the study and distribute flyers (García et al., 2017). In addition, CHWs used their connections to inform and recruit participants at local establishments, including health clinics, community centers, churches, and by word of mouth through family or friends, an important practice in Hispanic culture (García et al., 2017). Participants gave written consent to take part in the study; all visits were conducted in Spanish.
Measures
Bilingual study personnel developed a checklist for the home assessment and an educational pamphlet in English and Spanish using a simple, attractive layout and visuals to help communicate the message, aiming for a sixth-grade reading level (CDC, 2009). The materials were based on an extensive literature review, as well as input from sources in the Texas border region including the El Paso Department of Public Health, El Paso Fire Department, Safe Riders Traffic Safety Program, and West Texas Regional Poison Center.
The checklist included common home hazards associated with 13 hazard topics: poisoning, electrical safety, household fires, falls, burns and scalds, drowning, choking, strangulation, child passenger safety, sleep safety, mosquitoes, abandoned items outside the home, and firearms (Table 1). The checklist was divided into hazards typically found in seven predefined high-exposure, high-risk areas of the home (Phelan et al., 2011): kitchen (29 hazards), family room (20 hazards), child’s bedroom (23 hazards), bathroom the child typically uses (10 hazards), halls/stairs/balconies (4 hazards), other and external areas (19 hazards), and the car the child generally rides in (5 hazards). Some hazards overlapped among the areas assessed.
Total Hazards Present From Visit 1 to Visit 2 by Hazard Topic and by Related Hazards, and the Proportion Present at Each Visit
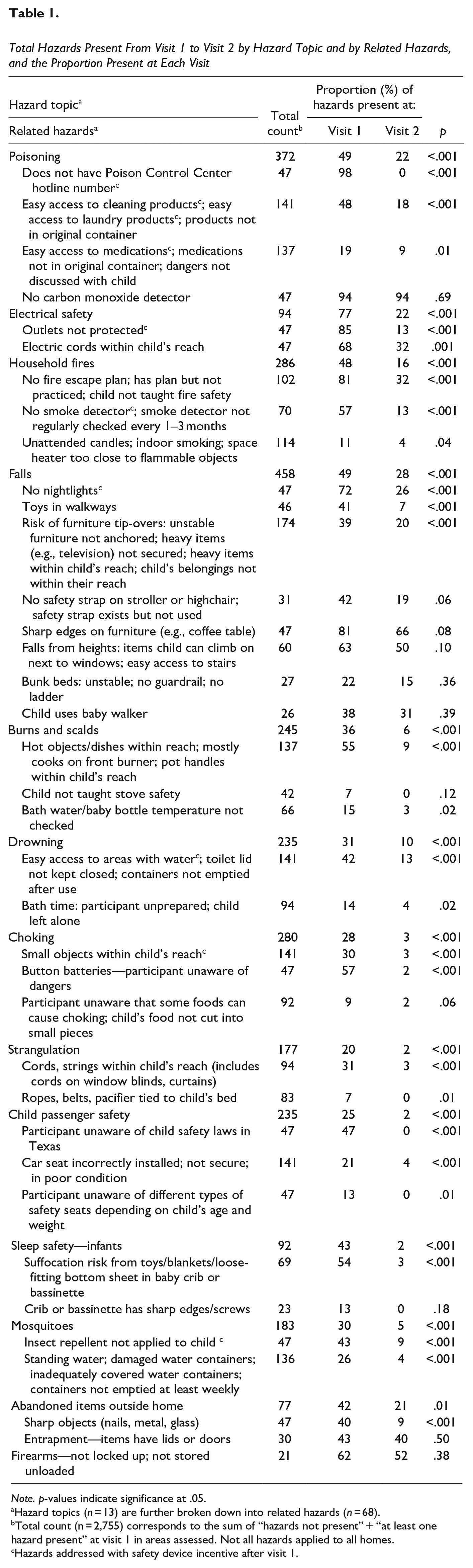
Note. p-values indicate significance at .05.
Hazard topics (n = 13) are further broken down into related hazards (n = 68).
Total count (n = 2,755) corresponds to the sum of “hazards not present” + “at least one hazard present” at visit 1 in areas assessed. Not all hazards applied to all homes.
Hazards addressed with safety device incentive after visit 1.
The assessment listed color-coded response options to characterize whether the hazard was present (red) or not present (green). For instance, infant sleep hazards were assessed by observing the conditions of the baby’s crib or bassinet as well as loose or extra items in the crib that could cause suffocation. Response options for “Crib or bassinette has sharp edges or loose screws” were “no” (green) to indicate no hazard was present that the child could cut themselves on or “yes” (red) to indicate the hazard was present. An additional number column on the checklist coincided with the number on the educational pamphlet for easy reference.
The pamphlet was divided by hazard topics (e.g., falls, poisoning, etc.). Each topic provided a short description of the injury risks, followed by common hazards associated with the topic, and recommended safety practices to address the hazard. Safety practices included simple, no-cost strategies (e.g., keeping the toilet lid closed) as well as recommended safety devices, if applicable. The educational pamphlet also included information on helpful resources, such as car seat programs, no-cost smoke alarms, and food pantries.
Three certified CHWs with ample experience in community outreach reviewed all materials to ensure the contents were easily understandable and aligned with Hispanic cultural values, beliefs, and language (García et al., 2017). They also verified the various terms were those most commonly used in the region. Materials were also reviewed by a certified CHW instructor and mother of a young child. A pilot training was then held with an additional four CHWs from the target area before finalizing the materials. All materials, including the CHW training curriculum, were certified by the DSHS (2021).
Home Assessments
UTHealth hired five certified CHWs who lived in or had prior outreach experience with the target communities and had previously collaborated with the university on other health promotion projects. UTHealth trained the CHWs using the DSHS-certified curriculum developed by study personnel in English and Spanish on common home hazards, safety practices, and the steps to complete a home assessment (O’Brien et al., 2009). These CHWs received DSHS-certified continuing education credits for their role in the project. It should be noted that the training was offered to any state-certified CHW interested in continuing education credits (N = 48). Changes in CHWs’ knowledge of home hazards and child injury risks as a result of the training curriculum were measured by comparing pre- and post-test responses using a paired t-test on the composite score, resulting in a statistically significant increase of 1.54 points (N = 48; p < .001). In addition, CHWs were highly satisfied with the training, as was evident in the training evaluation scores and feedback. Results are not shown.
At visit 1, lasting approximately 1 to 1.5 hr, the CHW visually assessed the home using the checklist and circled the appropriate responses. Participants were asked to accompany the CHW throughout the visit. If a hazard was unobservable, the CHW asked specific questions, for example, Are you familiar with Texas laws for child passenger safety? or Do you put your child in a baby walker? If the CHW observed something different from the participant’s response, the CHW circled what they observed and explained the reasoning to the participant. The CHW also circled the reference number on the checklist next to each hazard or marked it not applicable when appropriate (e.g., not all children used a baby crib). Once completed, the CHW circled the corresponding reference numbers on the educational pamphlet and then used the checklist and pamphlet to discuss the identified hazards with the participant and to make recommendations to reduce those hazards. All participants received the same safety incentive devices regardless of hazard status: outlet protectors, doorknob covers, drawer latches, mosquito repellent, nightlights, a smoke detector (with extra battery and screwdriver to facilitate installation/maintenance), a Poison Control Center magnet card, brochures on poisonous insects and plants in the region, and an educational coloring book for the child. At the end of the visit, the CHW answered any questions and left the educational pamphlet and a copy of the completed checklist with the participant indicating which home safety issues should be addressed.
At the 30-day follow-up visit, which lasted 30 to 45 min, the CHW (together with the participant) used the original checklist to evaluate whether hazards identified at visit 1 were still present. For each hazard circled at visit 1, the CHW circled the appropriate response—green (hazard not present) or red (hazard still present)—in the visit 2 column. The CHW and the participant then discussed any changes, resolved questions or concerns, and reviewed the safety practices on the educational pamphlet to address any hazards still present. Participants received a second incentive package containing a carbon monoxide detector, cabinet locks, a foam pad to cover sharp edges on furniture, and a tote bag.
During both visits, CHWs informally noted anecdotal information and participants’ comments, which served to inform some of the data interpretation in the discussion section.
Data Analysis
Each hazard was treated as a dichotomous variable, 0 = not present and 1 = present. The total count of potential hazards (Table 1) was calculated by taking the sum of hazards not present at visit 1 plus those in which 1 or more hazards were present at visit 1. The proportion of hazards among the 47 homes at each visit was computed as the number of hazards present divided by the total count. Hazards marked as “N/A” were not counted. Hazards found multiple times were only counted once (e.g., two or more unprotected outlets). Total counts and the proportion of hazards at each visit were computed for the hazard topic and each type of associated hazard, as shown in Table 1. Considering the extensive number of hazards assessed (68), 15 hazards were not included in the current analysis either because they no longer apply (e.g., specific requirements during the COVID-19 pandemic) or depended on another item. For instance, only one home had a carbon monoxide detector. We therefore focused on the presence of these devices, or lack thereof, in our analysis but not on whether they functioned correctly, as was instructed in the checklist. The one-sided Fisher’s exact test determined if a statistically significant reduction was observed in the proportion of hazards present from visit 1 to visit 2. Data were analyzed using STATA version 15.1 (StataCorp, 2017). A p-value threshold of .05 determined significance.
Relative risk assessed the impact of the safety devices on hazard reduction from visit 1 to visit 2. The total population consisted of all hazards identified at visit 1. Exposure was whether or not the identified hazard was addressed by a safety device after visit 1, and the outcome event was whether the hazard was still present at visit 2. Safety devices included in this analysis were outlet protectors, doorknob covers, drawer latches, mosquito repellent, nightlights, smoke detector, and Poison Control Center magnet card. Hazards associated with these devices are indicated in Table 1.
Results
Findings showed statistically significant reductions in hazards related to 12 of the 13 hazard topics (Table 1) from visit 1 to visit 2. Overall, of the total hazard count (N = 2,755 hazards present + not present across all homes), 39.6% were present at visit 1 (n = 1,090), whereas only 13.4% (n = 369; p < .001) were still present at visit 2, indicating a 26.2% reduction in hazards from visit 1 to visit 2 (p < .001). There was a 70% reduction in the overall risk of a hazard being present at visit 2, relative to visit 1 (relative risk = 0.30, 95% CI [0.28, 0.33], p < .001). No significant reductions were found in hazards related to firearm safety, carbon monoxide detection, bunk bed safety (unstable when lightly pulled on, no guardrails, no ladder), baby walkers, window screens, or entrapment in abandoned items.
Relative risk analysis (Table 2) indicated that hazards present at visit 1 and addressed with a safety device incentive (n = 254) had an absolute risk of 17.7% of still being present at visit 2. Hazards identified at visit 1 but not addressed with a safety device (n = 836) had an absolute risk of 38.8% of still being present at visit 2. Thus, hazards addressed with a safety device after visit 1 were 0.46 (95% CI [0.35, 0.60], p < .001) times less likely to still be present at visit 2 compared to hazards not addressed with a safety device.
Relative Risk of Hazards Addressed With Safety Device Incentives Relative to Hazards Not Addressed With Safety Incentives
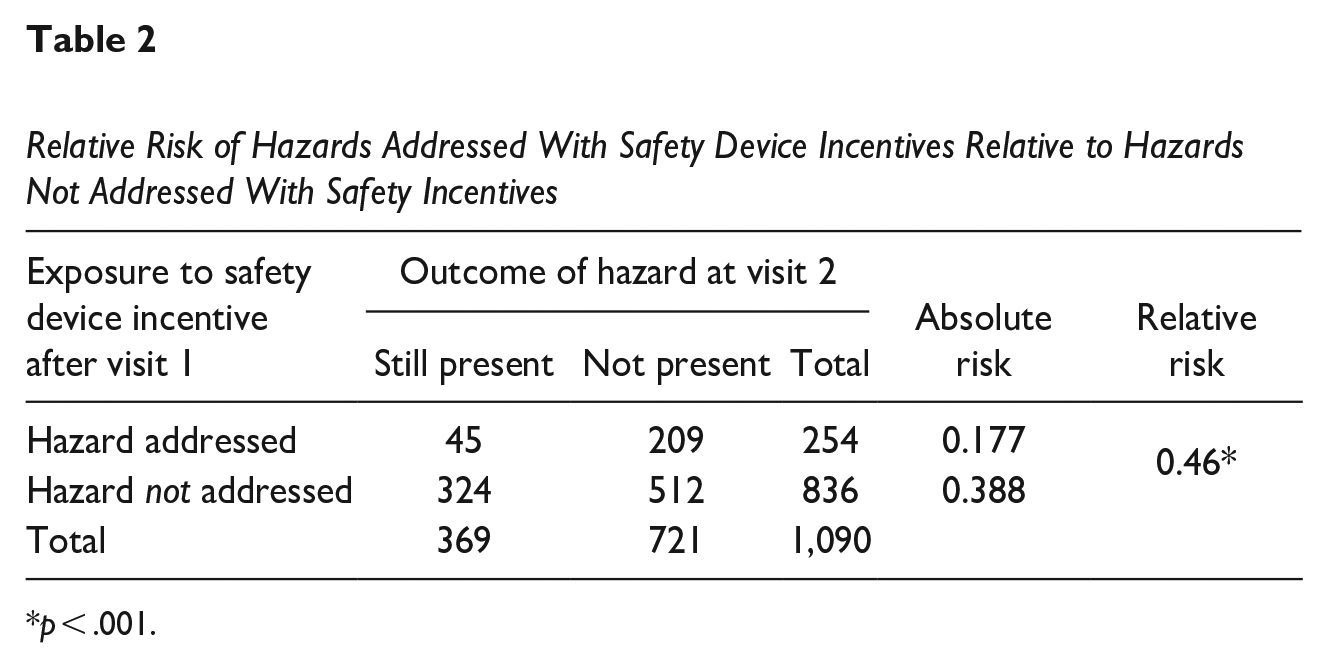
p < .001.
Discussion
This study achieved its intended outcome of reducing common hazards that pose a risk for unintentional injuries to children ages 5 and under in low-income rural Hispanic homes along the Texas–Mexico border. Consistent with past research, our results suggest that prevention education delivered by CHWs to parents and caregivers is an effective approach to increase awareness of child injury hazards (Garza et al., 2012; Hendrickson, 2005; Setien et al., 2013). Unlike other studies (Garza et al., 2012; Hendrickson, 2005; Setien et al., 2013), pre- to post-intervention changes in knowledge were not measured in this study. More importantly, however, our findings provide evidence that CHW-led home assessments coupled with culturally appropriate informative materials and prevention strategies actually reduce the number of child injury hazards in the home, thereby reducing the risk for child injury. To our knowledge, no studies among similar populations along the Texas–Mexico border conducted sequential home visits to measure changes in hazard risks, and no studies included such an extensive number of hazards. A study among low-income households in South Texas reported improvements in home safety behavior at 2-month follow-up, although findings were based solely on phone calls with participants and not in-person visits (Setien et al., 2013). Home assessments offer a more tailored method to identify hazards and recommend appropriate safety practices, and future research among hard-to-reach populations should be carried out to determine the impact of home assessments on injury rates.
Our findings suggest that more information on common home hazards may help reduce injury hazards. Some hazards were not as present as others, possibly indicating that parents may be more vigilant or aware of the risks certain hazards pose. For instance, participants seemed aware that food should be cut into small pieces to prevent choking, and access to areas with water should be restricted. Flammable objects were not an issue, although carrying out the intervention during the summer months likely had an impact. Overall, however, common hazards assessed in this study were widely present in all homes, as was found in other studies among similar households (Garza et al., 2012). In addition, unobservable hazards that relied on participant input may have been present at higher rates than what was found. Nonetheless, we are confident that the intervention increased awareness of home safety, and we expect that participants will continue to address hazards to some degree. Future research should consider assessing the sustainability of hazard reductions over a longer period of time.
Child injuries can be a sensitive topic for parents, especially when a home assessment is involved. Having a stranger in their home who then identifies injury risks is often intimidating and upsetting. Effective outreach strategies require skills to communicate and gain trust of hard-to-reach populations, as well as cultural considerations (Hendrickson, 2005; Setien et al., 2013; Slemaker et al., 2017). CHWs are well suited to address feelings of distrust and influence the acceptance of these types of programs, particularly when using materials in the language and cultural context of the target population. Our findings provide evidence that low-income Hispanic families living in rural communities are likely receptive to culturally appropriate interventions (Garza et al., 2012), especially if they fully understand the usefulness and purpose of the intervention (Hendrickson, 2005).
Participants indicated that the intervention increased their understanding of home hazards, and they were grateful for the recommendations despite an initial leeriness or disbelief of learning anything new. Most were young mothers, many single, who were unaware of or ignored the potential for injury, whereas older participants overlooked or had forgotten about certain dangers and readily accepted the reminders and new information. All participants agreed it is easy to forget how “little things can prevent bigger problems.” The simplicity of the educational pamphlet was appreciated, some saying that it made it easier to convince their partners and other family members of the importance of home safety practices.
Similar to other studies (Borse et al., 2008; Children’s Safety Network, 2019; Slemaker et al., 2017), the safety incentives likely served as motivation to remove hazards, particularly if instructions were provided on the proper installation and use as well as any tools (e.g., batteries, screwdriver) necessary for correct implementation. Even so, poverty-related stress can make safety devices less of a priority (Pressley et al., 2009). Participants in this study stated the no-cost recommendations (e.g., keep toilet lids closed) were more practical and sustainable due to other more pressing needs, such as diapers, medications, and food (Hendrickson, 2005). Access to and actual use of safety devices is an ongoing hurdle and should continue to be evaluated. Evidence suggests that free distribution or voucher systems have increased device ownership among Hispanics, although sustainability has proven problematic (Pressley et al., 2009). Future interventions that plan to include safety devices should take into consideration that families have limitations, and the intervention may risk negative outcomes if correct implementation and proper use of safety devices is not communicated or if families do not have access to such devices.
The newly certified CHW training curriculum developed for this study also achieved the intended outcome of increasing knowledge of home hazards and unintentional child injuries. This suggests that curriculum and intervention cover information not widely known.
The intervention also had its challenges. Residents were initially reluctant to participate due to safety concerns or fear of having been reported in some way (e.g., child abuse, immigration status), the invasiveness of the visits, and disbelief of learning anything new. Yet once participants realized its usefulness, they spread the word to others, which was central to our recruitment success. Working within existing trusted networks was critical for outreach success, given the intrusiveness of the intervention.
Some safety practices presented difficulties, even the no-cost recommendations. For instance, small homes with reduced space made it difficult to remove some hazards, such as moving furniture to prevent access to a window if there was no other place to put that furniture. The CHW training, therefore, included creating conscientiousness to make recommendations gently and with sensitivity to the home conditions.
Overall, the positive results in the reduction of hazards, in addition to participants’ comments, provide support for culturally focused, bilingual home safety interventions and for the HBM. The intervention provided participants with knowledge of the risks specific hazards pose and the skills to reduce or address those risks to achieve a safer home for their child. Perhaps most importantly, the intervention provided participants with the resources necessary to address many hazards. Findings suggest that home safety programs are useful to increase parental awareness of hazards that pose a risk to children, which, in turn, may lead to actions to reduce such hazards, especially when the resources to address such hazards are available. This study also highlights the challenges these communities face to protect their children and the need to expand opportunities to all population groups.
Given the observational nature of the findings and the absence of a control group, the association between the assessments and improvements cannot unequivocally be attributed to the intervention. Results may provide evidence of change but do not exclude other possible explanations for the observed changes, including altering the home immediately before each visit. Another limitation was the small sample size, which limits the precision of the risk reduction estimates. Nonetheless, it seems reasonable that an intervention that identifies hazards and provides recommendations to reduce those hazards would lead to the observed results. Evidence for the effectiveness of this intervention would be enhanced by future research involving a randomized control design.
Relying on participants’ input to identify unobservable hazards may have resulted in higher reductions. Future studies should consider methods that do not require participants to self-report hazards. Pre- to post-intervention levels of participant knowledge of hazards or current practices were not measured but would be an important aim for future studies. Similarly, more research is needed to assess the impact the intervention has on sustainability of hazard reduction over time and its effect on child injury rates, which may require extending the study timeframe, analyzing visits to emergency rooms and local clinics, including a randomized control group, and assessing current practices.
Conclusions
Unintentional child injuries caused by common hazards in the home are generally predictable and preventable. This study contributes to designing culturally and geographically focused home safety educational programs to increase parental awareness among low-income populations. Given the expected growth of Hispanic populations, more inclusion and opportunities for these communities are needed. CHWs represent an effective strategy to address feelings of distrust and promote acceptance of these programs in hard-to-reach populations.
Footnotes
Acknowledgements
We are grateful to the community health workers who participated in this project for their excellent work on this sensitive topic and for reviewing all materials to ensure appropriateness and understandability.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Department of State Health Services under contract number HHS000775700001. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of State Health Services.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.