
Abstract
The current study evaluated work- and client-related burnout, perceived stress, and race-based stress with a focus on Black, Indigenous, or Persons of Color (BIPOC) mental health providers. An online survey (n = 82) was distributed in the United States between July 17, 2020, and November 5, 2020. Demographic variables, racial discrimination during coronavirus disease 2019 (COVID-19), perceived stress, and the coping variables were assessed. The majority of respondents were women (85%), BIPOC identifying (72%), aged 25 to 34 years (43%), psychologists (50%), and had been practicing for 9 years. In total, 68% and 27% of providers reported moderate to severe work- and client-related burnout, respectively. Another 87% reported moderate to high stress. Factors associated with a higher level of burnout include being younger, having fewer years of experience, and being a social worker or family therapist. Among BIPOC providers, greater experiences of racial discrimination were associated with higher work-related burnout and stress. Greater use of maladaptive coping was associated with higher burnout and stress, yet we found no associations with the use of adaptive coping. Racial discrimination during COVID-19 was significantly associated with work-related burnout and perceived stress within a sample of predominantly BIPOC mental health providers. These findings reinforce the need for more focused support for mental health providers to ensure a healthy and resilient future workforce.
The novel coronavirus disease 2019 (COVID-19) has had an unprecedented impact on the provision of mental health services. The unparalleled nature of the pandemic highlighted glaring racial disparities for those who identify as Black, Indigenous, or Persons of Color (BIPOC) through healthcare inequities (Tai et al., 2021), higher mortality due to systemic racism (Rossen et al., 2020; Tai et al., 2021), and race-based violence against Black and Asian people (Liu & Modir, 2020). Consequently, while navigating systemic and institutional barriers, BIPOC mental health providers may be practicing in spaces that exacerbate burnout or more specifically, spaces that induce emotional exhaustion, depersonalization, and reduced personal accomplishments (Morse et al., 2012; O’Connor et al., 2018). BIPOC mental health providers experienced pre-pandemic exposure to burnout, systemic racism, racial discrimination (Clark, et al., 1999; Jones, 1997); race-based stress or trauma (Bryant-Davis, 2007; Comas-Díaz et al., 2019; Utsey, 1999; Williams, 2018); increased diversity, and equity-related service responsibilities (Turner et al., 2008); and mentorship of BIPOC trainees who were also burdened by pandemic stress (Nocco et al., 2021). Thus, the combination of two pandemics—COVID-19 and the racial unrest of 2020—poses unique challenges to BIPOC mental health provider wellness.
In general, mental health providers are prone to burnout due to demanding therapeutic relationships, administrative job demands, stigma of the profession, and variable patient outcomes (O’Connor et al., 2018; Posluns & Gall, 2020). Less is known about how BIPOC mental health providers cope with burnout and race-based stress. For Black mental health providers, race-based stress predicts both burnout and secondary traumatic stress (Driscoll et al., 2015; Shell et al., 2021); however, Black therapists’ constant appraisal and perceptions of race-based stress may complicate coping. Therapists who identify as women of color have reported that expectations to perform emotional labor, defined as the need to repress or induce certain feelings to accomplish one’s job professionally as part of their roles, experience accompanying feelings of burnout and exhaustion (Siddique, 2018). Factors related to increased burnout among mental health providers, including increased job demands (Sklar et al., 2021), lack of job control (O’Connor et al., 2018; Ray et al., 2013), and demanding caseloads (O’Connor et al., 2018) were all directly impacted by the pandemic (Sklar et al., 2021). Therefore, even before the COVID-19 pandemic, BIPOC therapists were often assisting their clients and colleagues through both race-based stressors and burnout that were exacerbated by the inequities produced by the pandemic.
Although there is a scarce amount of research on the experience of race-related stress and coping among BIPOC mental health providers during the COVID-19 pandemic, racial trauma is known to increase both the occupational burden and the vulnerability to burnout for this group (Meyer & Young, 2021; Miu & Moore, 2021; Shell et al., 2021). Taken together, BIPOC providers are bearing a uniquely heavy psychosocial load during the COVID-19 pandemic that could have long-term implications for mental health service provision for the traditionally underserved communities that these providers are more likely to serve (Miu & Moore, 2021).
Current Study
This study examined risk and protective factors for burnout and perceived stress among predominantly BIPOC mental health providers during the COVID-19 pandemic. Our aim was to increase our understanding of provider experiences during this unprecedented time and specifically, explore how racial discrimination experienced by BIPOC providers contributes to burnout and stress.
Method
This was a prospective, observational study of a convenience sample of mental health providers. The study was conducted in 2020, with data collection happening over a 4-month time frame within the first 9 months of the COVID-19 pandemic—from July to November 2020. The authors were intentional about capturing data during the societal unrest after the murders of George Floyd, Breonna Taylor, and Ahmaud Arbery, given the likelihood that BIPOC mental health providers may be asked to provide support for their colleagues during this time (Miu & Moore, 2021). The central source of data came from self-report surveys of respondents. The survey asked a variety of questions related to experiences of racial discrimination, stress, coping, and burnout, which are further elaborated in the Measures section. This study was approved by the Baylor University College of Medicine Institutional Review Board.
Participants
Mental health professionals who were at least 18 years old and residing in the United States were eligible to participate. Participants ranged from graduate trainees to doctoral professionals. As this was an exploratory study, a power analysis was not completed prior to data collection. A total of 150 survey responses were collected; 43 participants were excluded due to incomplete responses, and a further 25 participants were excluded because they were not currently practicing mental health providers. This resulted in a final sample of 82 participants, 59 of whom identified as BIPOC. The inclusion of non-BIPOC providers allowed us to include race as a variable in analyses. Work environment and occupation varied and included license-eligible mental health fields (counseling, psychology, psychiatry, and social work; see Table 1).
Demographic Characteristics and Descriptive Statistics Among the Study Sample
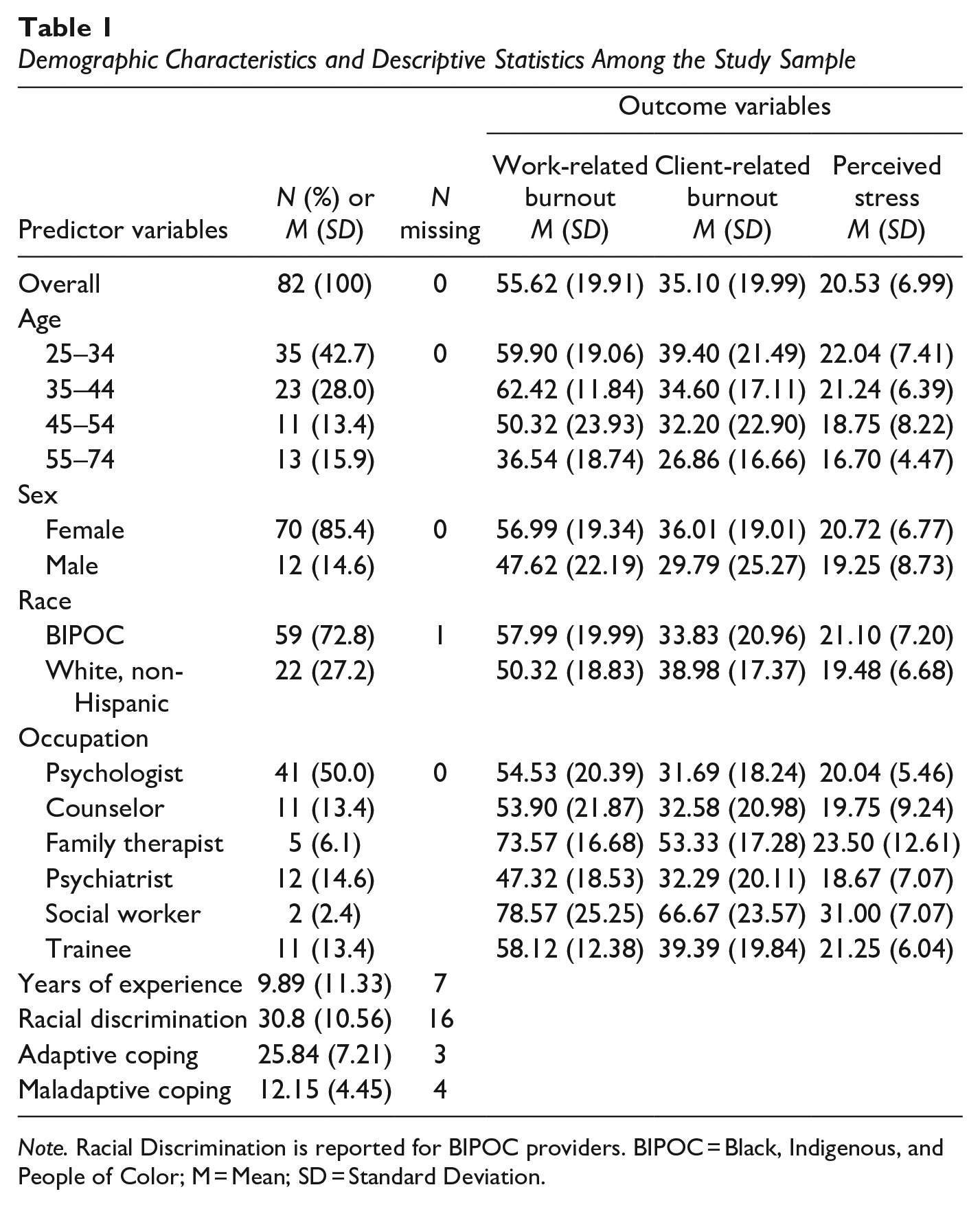
Note. Racial Discrimination is reported for BIPOC providers. BIPOC = Black, Indigenous, and People of Color; M = Mean; SD = Standard Deviation.
Procedure
An anonymous survey was distributed online, on social media accounts, and through mental health listservs. Recruitment emails were intentionally sent to listservs associated with mental health providers. Recruitment using social media was done by distributing an electronic invitation-to-participate flyer through the authors’ personal accounts on Instagram and Facebook. The same electronic flyer was sent to national mental health provider listservs affiliated with mental health professional organizations. Responses were collected between July 17, 2020, and November 5, 2020. Participants consented to participate by clicking the survey link and advancing. Incomplete responses were recorded but not used in analyses.
Measures
Demographic Questionnaire
We asked respondents to self-report their age (18–24, 25–34, 35–44, 45–54, 55–74 years), sex (dichotomized to male or female), occupation (psychologist, psychiatrist, social worker, family therapist, counselor, and trainee), and the number of years of experience as a mental health care provider. Respondents reported their race from a list of options (e.g., Black or African American, Hispanic or Latino, and White) and could also self-describe their race. We used these responses to dichotomize race into BIPOC and non-Hispanic White categories for analyses.
Racial Discrimination
We adapted the 18-item Schedule of Racist Events (SRE; Landrine & Klonoff, 1996) to assess racial discrimination among BIPOC identifying providers during COVID-19. Respondents indicate if several discriminatory events have happened to them during COVID-19 because of their race on a six-point scale (1 = “Never happened to you,” 6 = “Happened all the time [more than 70% of the time]”). Responses are summed with higher scores indicating greater experiences of racial discrimination during COVID-19 (ɑ = 0.90).
Coping
We used the 28-item Brief coping orientation to problems experienced inventory (Brief- Cope, Carver, 1997) to measure two types of coping (Moore et al., 2011): adaptive coping (active coping, use of emotional support, use of instrumental support, positive reframing, planning, humor, acceptance, and religion, a = 0.65) and maladaptive coping (self-distraction, denial, substance use, behavioral disengagement, venting, and self-blame, a = 0.79). Each subscale uses a four-point scale (0 = “I haven’t been doing this at all,” 3 = “I’ve been doing this a lot”), and we summed items in each subscale with greater scores indicating greater use of those coping strategies.
Burnout
We used the seven-item work subscale and the six-item client subscale of the Copenhagen Burnout Inventory (CBI); (Kristensen et al., 2005) to assess burnout (we did not focus on personal burnout in this study). Each subscale uses a five-point scale (some items 0 = “To a very low degree,” 4 = “To a very high degree”; some items 0 = “Never/almost never,” 4 = “Always”), and we multiplied each item by 25 and then averaged items in the work (a = 0.89) and client (a = 0.89) subscales. Higher scores indicate greater burnout and in each subscale an average score <50 = no or low burnout, 50 to 74 = moderate burnout, 75 to 99 = high burnout, and 100 = severe burnout (Creedy et al., 2017).
Perceived Stress
We used the 10-item perceived stress scale (PSS); (Cohen et al., 1983) to measure the degree to which situations in one’s life are appraised as stressful on a five-point scale (0 = “Never,” 4 = “Very often”). We summed scores, with higher scores indicating greater perceived stress (α = 0.91). Total scores ranging from 0 to 13 = low stress, 14 to 26 = moderate stress, and 27 to 40 = high stress (Swaminathan et al., 2016).
Data Analysis
We conducted analyses using R version 4.0.4 (R Foundation for Statistical Computing, 2021). We performed Pearson correlations to evaluate associations between burnout and perceived stress. We performed independent samples t-tests, one-way between-subjects ANOVAs, and linear regression to evaluate how dichotomous, categorical, and continuous demographic factors, respectively, were associated with burnout and stress. In the analyses of burnout and stress, we included both White and BIPOC providers with racial identity as a potential correlate. We conducted unadjusted linear regressions to evaluate how racial discrimination (specifically among BIPOC providers) and coping (in the full sample) were associated with burnout and stress. If a model was significant, we conducted adjusted models with demographic variables as covariates. No data were missing for the CBI subscales. Two participants were missing responses from one or more adaptive and maladaptive coping items and were removed, from those analyses. The 18th item of the SRE was missing from all respondents, so we imputed scores for this item using the average of the other 17 items. We removed 16 participants from the racial discrimination analyses because they were missing one or more items on the SRE. We considered hypothesis tests statistically significant using an alpha level of .05.
Results
Participant Characteristics and Descriptive Statistics
A total of 150 participants responded to the survey, 82 of whom were currently practicing mental health providers and included in the analyses (see Table 1). The majority of participants were 25 to 34 years old (42.68%), female (85.37%), and had been practicing as a mental health professional for an average of 9.89 years (SD = 11.33 years). The breakdown of self-identified races in this sample was: 31 Black or African American (38.2%), 22 White (27.2%), 8 Asian (9.9%), 7 Hispanic or Latino (8.6%), 7 Multiracial or Multiethnic (8.6%), 2 Native American or Alaska Native (2.5%), and 4 self-described (1 Arab, 1 Multiethnic, identify as Black, 1 Pakistani American, and 1 South Asian, first generation immigrant to the United States, from India; 4.9%). After dichotomizing the race variable, 59 identified as BIPOC (72.8%) and 22 identified as White, non-Hispanic (27.2%). A total of 68.29% and 26.83% of participants reported moderate to severe work- and client-related burnout, respectively, and 87.1% reported moderate to high perceived stress. Work- and client-related burnout were positively associated with each other (r = .62, p < .001) and with perceived stress (r = .66, p < .001 and r = .55, p < .001, respectively).
Demographic Risk Factors
Work-related burnout (see Table 1) was negatively associated with years of experience, b = −0.75, SE = 0.19, 95% CI [−1.13, −0.38], R2 = .17, p < .001, and differed by age, F(3, 78) = 6.91, p < .001, with providers 55 to 74 years old reporting significantly lower work-related burnout than 25 to 34 and 35 to 44 years old. There were no differences in work-related burnout by sex, t(80) = 1.52, p = .13), race, t(79) = −1.56, p = .12, or occupation, F(5, 76) = 1.94, p = .10. Client-related burnout was negatively associated with years of experience, b = −0.46, SE = 0.20, 95% CI [−0.85, −0.07], R2 = .07, p = .02, and differed by occupation, F(5, 76) = 2.46, p = .04, with social workers and family therapists reporting significantly higher client-related burnout than psychologists, counselors, and psychiatrists. There were no differences in client-related burnout by age, F(3, 78) = 1.38, p = .26, sex, t(80) = 0.99, p = .32, or race, t(79) = 1.03, p = .31. There were no differences in perceived stress by age, F(3, 58) = 1.71, p = .18, sex, t(60) = 0.55, p = .58, race, t(59) = −0.83, p = .41, occupation, F(5, 56) = 1.27, p = .29, or years of experience, b = −0.13, SE = 0.08, 95% CI [−0.30, 0.04], R2 = .04, p = .13.
Racial Discrimination Among BIPOC Providers
BIPOC providers’ experience of racial discrimination during COVID-19 (see Table 2) was a significant correlate of higher client-related burnout in the unadjusted, b = 0.66, SE = 0.30, 95% CI [0.06, 1.26], R2 = .11, p = .03, but not adjusted model, b = 0.35, SE = 0.38, 95% CI [−0.44, 1.14], R2 = .35, p = .37, and a correlate of work-related burnout and perceived stress in both models (all ps < 0.05). After adjusting for demographic covariates, racial discrimination accounted for an additional 9% of the variance in work-related burnout and 15% of the variance in stress. Accordingly, for every one-point increase in racial discrimination, providers’ work-related burnout increased by 0.75 points, and their stress increased by 0.36 points.
Summary of Linear Regression Analyses for Racial Discrimination During COVID-19 Among BIPOC Providers as a Predictor of Work-Related Burnout and Perceived Stress
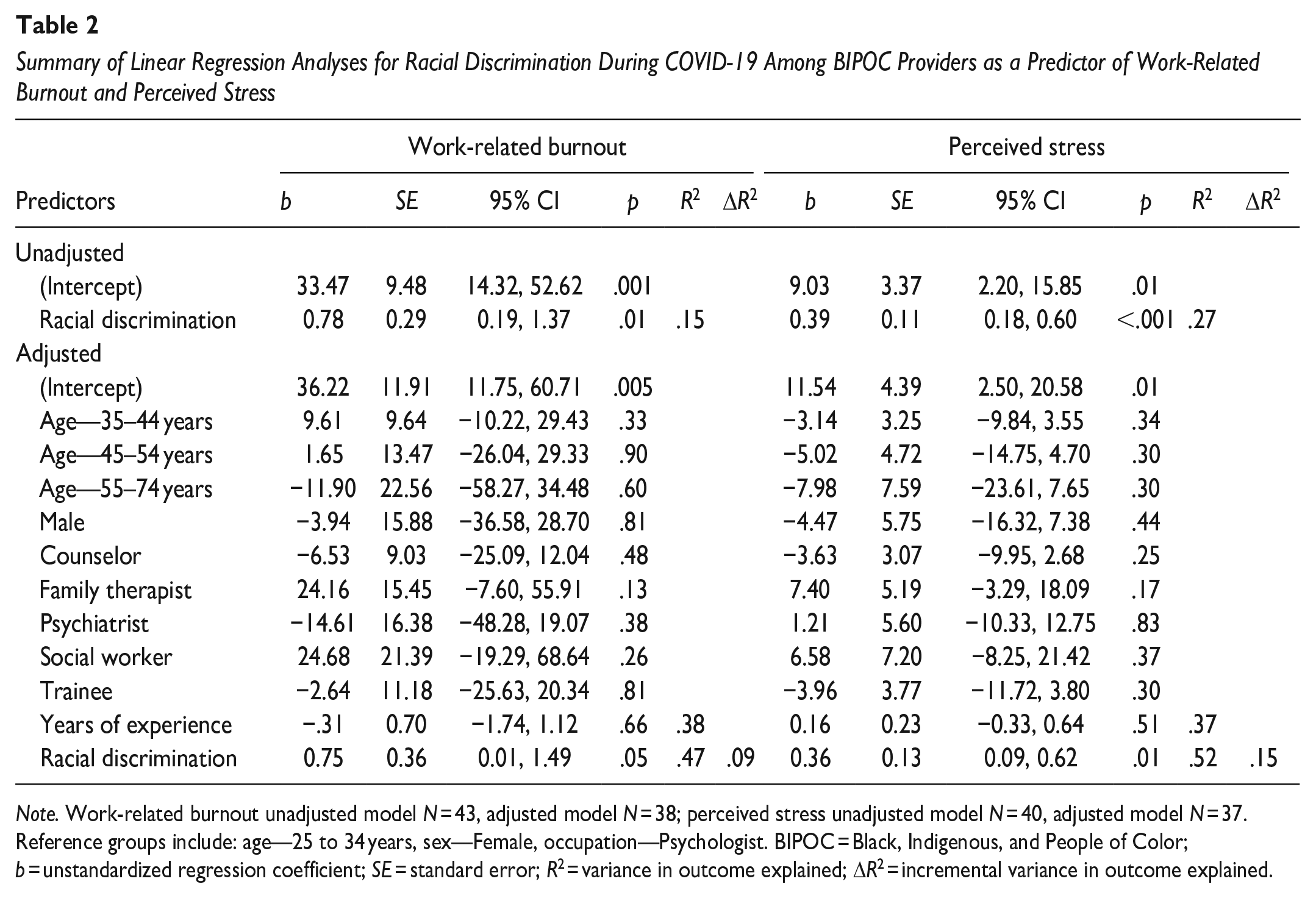
Note. Work-related burnout unadjusted model N = 43, adjusted model N = 38; perceived stress unadjusted model N = 40, adjusted model N = 37. Reference groups include: age—25 to 34 years, sex—Female, occupation—Psychologist. BIPOC = Black, Indigenous, and People of Color; b = unstandardized regression coefficient; SE = standard error; R2 = variance in outcome explained; ΔR2 = incremental variance in outcome explained.
Adaptive and Maladaptive Coping
Adaptive coping was a significant correlate of stress in the unadjusted, b = −0.27, SE = 0.12, 95% CI [−0.51, −0.02], R2 = .07, p = .03, but not adjusted model, b = −0.22, SE = 0.15, 95% CI [−0.52, 0.07], R2 = .23, p = .14 (see Table 3). Adaptive coping was not a significant correlate of work-related, b = −0.29, SE = 0.31, 95% CI [−0.92, 0.33], R2 = .01, p = .35, or client-related burnout in unadjusted models, b = −0.46, SE = 0.32, 95% CI [−1.08, 0.17], R2 = .03, p = .15. Maladaptive coping (see Table 3) was a significant correlate of higher work- and client-related burnout and perceived stress in both models (all ps < 0.05). After adjusting for demographic covariates, maladaptive coping accounted for an additional 19% of the variance in work-related burnout, 10% of the variance in client-related burnout, and 42% of the variance in stress. Accordingly, for every one-point increase in maladaptive coping, providers’ work-related burnout, client-related burnout, and stress increased by 2.14 points, 1.52 points, and 1.13 points, respectively.
Summary of Linear Regression Analyses for Maladaptive Coping as a Predictor of Provider Burnout and Perceived Stress
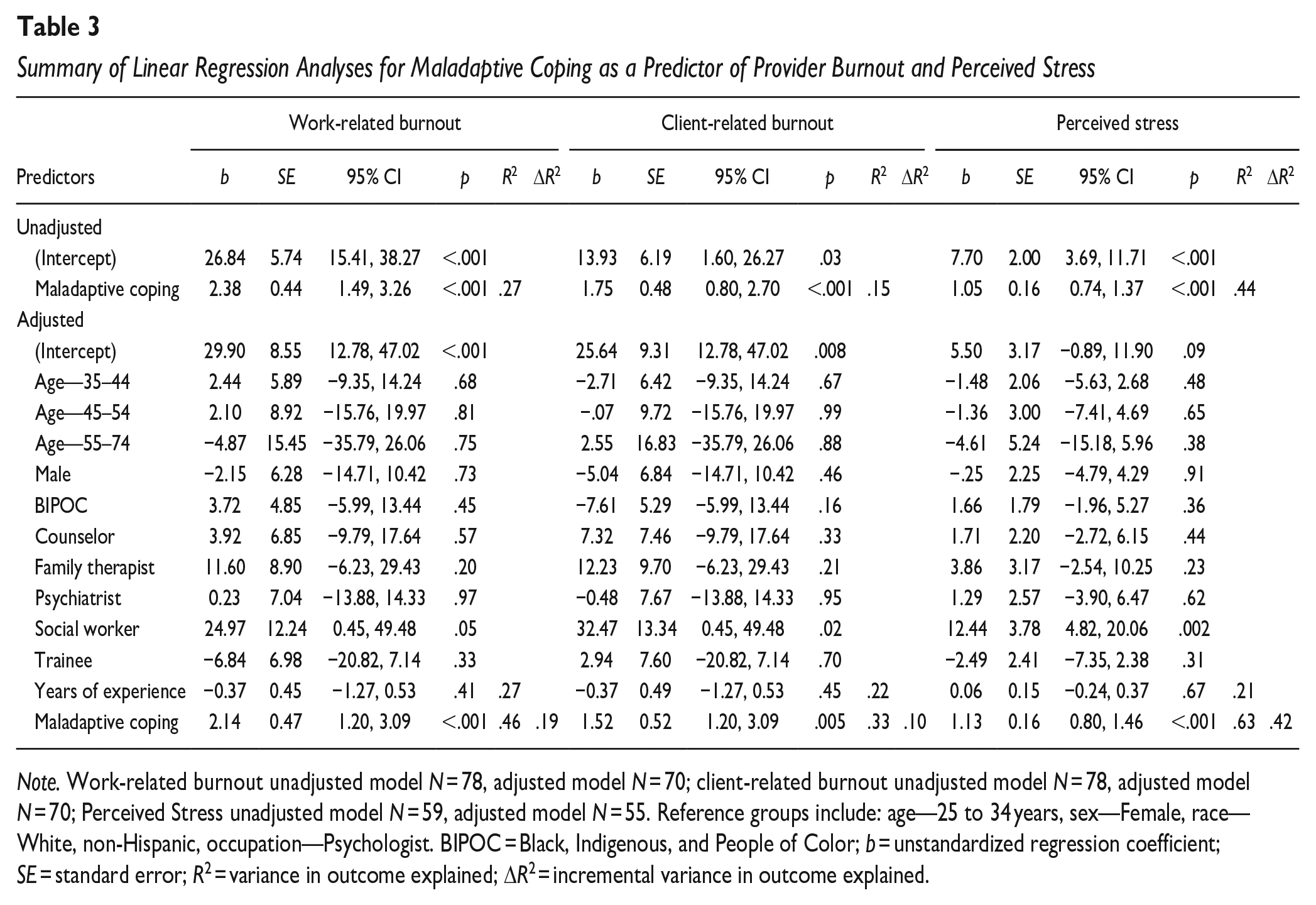
Note. Work-related burnout unadjusted model N = 78, adjusted model N = 70; client-related burnout unadjusted model N = 78, adjusted model N = 70; Perceived Stress unadjusted model N = 59, adjusted model N = 55. Reference groups include: age—25 to 34 years, sex—Female, race—White, non-Hispanic, occupation—Psychologist. BIPOC = Black, Indigenous, and People of Color; b = unstandardized regression coefficient; SE = standard error; R2 = variance in outcome explained; ΔR2 = incremental variance in outcome explained.
Discussion
This study explored burnout, perceived stress, and experiences of race-based discrimination among predominantly BIPOC mental health providers during the COVID-19 pandemic. The first aim of this study was to explore if experiences of racism influenced levels of burnout for BIPOC providers during this unique time. The second aim of this study was to increase understanding of coping and protective factors that help mitigate burnout for predominantly BIPOC mental health clinicians.
In a predominantly BIPOC identifying sample of mental health providers, 68% reported moderate to severe work-related burnout during COVID-19, while 27% reported moderate to severe client-related burnout. These data support qualitative reports of increased work responsibilities for BIPOC clinicians due to the disproportionate effects of COVID-19 in communities of color and increased responsibility to lead anti-racism efforts (Miu & Moore, 2021). Furthermore, greater experiences of racial discrimination were associated with higher work-related burnout and perceived stress among BIPOC providers. These results suggest racial discrimination during COVID-19 contributes to increased burnout and stress. While these factors were examined during the pandemic, it is important to note that these stressors are not isolated from the pandemic and existed prior to the outbreak of COVID-19. BIPOC mental health providers represent a relatively small proportion of mental health providers in the United States (Lin et al., 2018; National Association of Social Workers, 2011; Wyse et al., 2020); therefore, the demand for these providers far outweighs available resources (Health Resources & Services Administration, 2017). Findings from this study highlight the urgent and ongoing need to address race-related stressors and the effects of race-related stress on BIPOC mental health providers to prevent this limited resource from continuing to dwindle.
Additionally, this study found that provider age and years of experience were the protective factors, while certain occupations like social work (that may serve complex patient populations) tended to experience greater burnout. Older providers had lower work-related burnout compared to younger providers, and providers with more years of experience had lower work- and client-related burnout compared to those with fewer years of experience. This aligns with earlier work that found that starting in training, BIPOC counseling students in graduate school report higher levels of personal exhaustion, cynicism, and efficacy as a result of discrimination-related stressors (Basma et al., 2021). Understanding the mechanisms that help BIPOC mental health professionals cope and remain in their careers will be crucial to graduate training programs.
Among all providers, greater use of maladaptive coping strategies, as opposed to the use of adaptive coping strategies, was associated with higher work- and client-related burnout and perceived stress. This indicates that the use of maladaptive coping strategies exacerbates burnout and stress. Recent research examining coping strategies of mental health providers during the COVID-19 pandemic has found trainees have more adaptive coping strategies due to access to supervision (Reilly et al., 2021). This finding is not consistent with current study results, given that years of experience was a protective factor to burnout. This could be explained by the timing of data collection since data was collected within the first 6 to 8 months of the pandemic. Mental health providers may have experienced more stress and uncertainty during the early days of the pandemic, but having more experience may have helped providers navigate pandemic uncertainty.
Implications
Taken together, these findings have several implications for the mental health field. The primary implication is the need to escalate ongoing anti-racism efforts to protect the mental health of BIPOC mental health professionals. Miu and Moore (2021) explored the experiences of mental health professionals of color and provided recommendations to help BIPOC providers combat burnout and racism. They emphasize the importance of individual, institutional, and system-level change to truly address this issue. Practices such as self check-ins, provision of external healthcare resources, and policy changes that include the perspectives of BIPOC mental health professionals are a few of the suggestions presented by the authors.
Furthermore, it will be critical to equip BIPOC trainees and early career mental health professionals with support and adaptive coping strategies to support stress management and counter burnout. The protective and risk factors found in our study are indicative of potential disparities in workload burden among different types of mental health professionals. More research is needed that examines specific factors influencing higher levels of burnout among subfields, especially social workers and family therapists.
Limitations
The small sample size may limit the generalizability of results to mental health providers, particularly those who identify as Black, Indigenous, or People of Color. Furthermore, different mental health providers were represented and different terminal degrees obtained. It is documented that disparities in burnout, stress, and coping vary by type of mental health profession; however, more research is needed to determine the specific causes of this difference and provide sustainable intervention to mitigate burnout among BIPOC providers. This was also a cross-sectional survey, so we cannot establish causality. Additionally, as data were collected within the first 9 months of the COVID-19 pandemic, our ability to generalize the findings beyond pandemic conditions are limited. The next steps would include more research on work-related contributors to burnout, race-related stress, and coping that were both brought on by the COVID-19 pandemic and transcend this unique point in history, specifically for BIPOC mental health clinicians. The unique challenges presented by the intersections of a public mental health crisis and racial unrest require immediate attention to ensure that the mental health field is able to train and successfully retain BIPOC mental health providers for the future.
Conclusions
Findings suggest that more research must be conducted to address the nuances of BIPOC mental health provider’s burnout and experiences with race-related stress. The results have implications for mental health education, given that both non-BIPOC and BIPOC mental health providers and supervisors need to be aware of how to appropriately intervene when providers or trainees are experiencing race-based stress and burnout. Further research exploring race-based stress, perceived stress, and coping mechanisms among different mental health subfields may illuminate disparities among providers that are worthy of more attention. BIPOC mental health providers are not exempt from the racial injustices and health disparities that their communities have experienced. We need to determine ways to best support BIPOC groups to ensure that they are able to remain in mental health practice to serve and support the race and ethnicity groups that they are already more likely to serve.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.