
Abstract
A 75-year-old man presented with an abdominal enlarging painless tumor of the skin evolving over the last 30 years. His past medical history was unremarkable. Physical examination revealed a brownish pedunculated cutaneous mass which had an irregular keratotic warty surface with no discharge or ulceration. The mass was clinically presumed to be a melanocytic tumor, or a verrucous carcinoma. A monoblock excision of the mass was performed with a good outcome. The specimen was then sent to our pathology department to rule out malignancy. Macroscopic examination revealed a brownish tumor of 7.5 × 7 × 1.5 cm which had fissures and cauliflower-like appearance. Final histological report concluded to a giant seborrheic keratosis.
Keywords
Introduction
Seborrheic keratosis (SK) is a common benign epidermal tumor that typically affects elderly people. 1 In dermatological routine practice, the diagnosis is easily established when SK presents with typical clinical features such as brown plaque with a warty surface. 2 However, atypical presentations may occur resulting in diagnostic difficulties, especially among general surgeons and primary care physicians. Large SK is quite rare and has not been sufficiently documented in the literature so far.3 -6
Herein, we report a case of a 75-year-old man with a giant abdominal SK.
Case Report
A 75-year-old man presented to the general surgery department with an enlarging painless tumor of the skin evolving over the last 30 years in the upper right quadrant of his abdomen. The lesion started as a small pigmented papule which gradually increased in size to become a large mass. There were no other associated symptoms such as pain, itching, or bleeding. The patient was in a good health and his past medical history was unremarkable. There was no family history of skin disease. Physical examination revealed a brownish pedunculated cutaneous mass which had an irregular keratotic warty surface with no discharge or ulceration. The mass was attached to a short stalk of 4 mm. There was no evidence of inflammatory changes of the skin around the lesion. The mass was clinically presumed to be a melanocytic tumor, a verruca vulgaris, or a verrucous carcinoma.
Subsequently, a monoblock excision of the mass was performed under local anesthesia. The procedure was uneventful. The specimen was then sent to our pathology department for histopathological examination and to rule out malignancy.
Macroscopic examination revealed a brownish tumor of 7.5 × 7 × 1.5 cm which had fissures and cauliflower-like appearance (Figure 1).

Grossly, the mass was brownish, measured 7.5 × 7 × 1.5 cm and had warty surface with cauliflower-like appearance.
The specimen was formalin-fixed, paraffin-embedded, and then entirely analyzed.
Histologically, there was proliferation of basaloid keratinocytes with no dysplasia. The epidermis showed extensive acanthosis with papillomatosis, hyperkeratosis, and pseudohorn cysts formation. Microscopic findings were consistent with seborrheic keratosis (Figure 2).
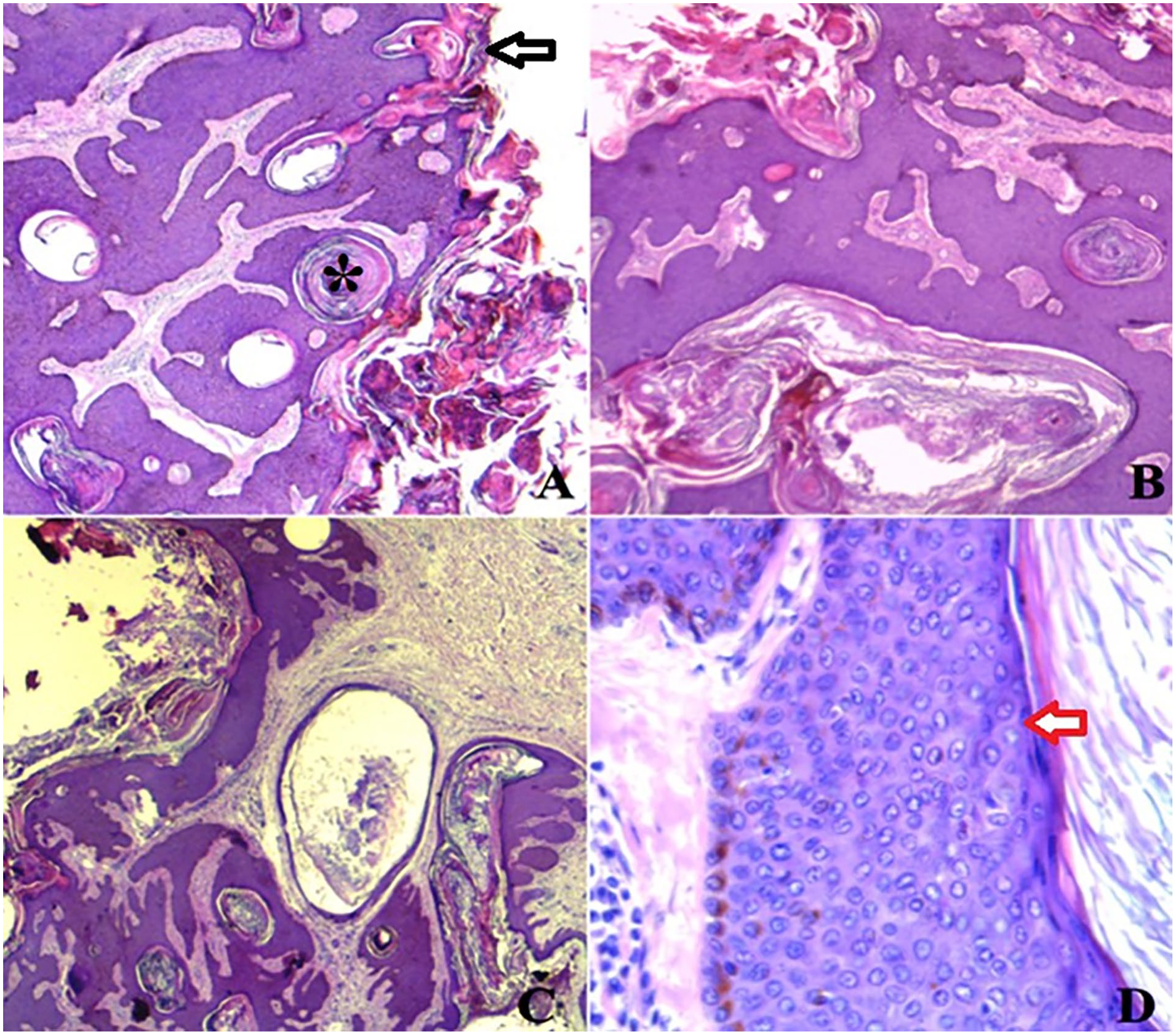
(A, B and C) Histopathological examination of the lesion revealed acanthosis of the epidermis with hyperkeratosis (black arrow) and horn pseudo-cysts (asterisk) (H&E stain × 40). D) Microscopic examination showed basaloid cell proliferation (red arrow) with hyperpigmentation of the basal layer (H&E stain ×200).
At 3 months of follow-up, the patient was doing well. The surgical site was well healed and no recurrence was observed.
Discussion
Seborrheic keratosis (SK) is the most common skin lesions seen by dermatologists in routine practice.7,8 It is usually encountered in the elderly population. 1 Men and women are equally affected.7,8
Usual clinical features, unusual clinical features, and clinical misdiagnosis
SK can occur anywhere on the body with predilection of the back, chest, head, and neck. Palms, soles, and the mucus membranes are generally not affected.7,8
SK is usually asymptomatic. 8 However, trauma or irritation may result in itching and pain. 7 Lesions are typically sharply demarcated and presented as stuck on verrucous plaques with variable thickness.7,9 Their color may be yellowish, gray-brown, or black. 7 Clinical variants of SK include stucco keratosis, dermatosis papulosis nigra, lichen planus-like SK, inflammatory SK, large cell acanthoma, flat SK, inverted follicular keratosis, and Leser-Trelat syndrome.7,8,10 The latter is a paraneoplastic syndrome characterized by a sudden onset of numerous SK and it is associated with an internal organ malignancy. 7 The size of SK ranges from a few to many millimeters with an average diameter of 0.5 to 1 cm.7,8,11
In our case, SK reached 7.5 cm in greatest dimension which warranted histopathological examination.
Large SK is in fact an unusual presentation and it is rarely documented in the literature (Table 1).3 -6,12 -25 Giant SK have been notably described in genital areas.4 -6,17 -20,22 -24 The size of reported giant SK varies from 4.5 to 25 cm in greatest diameter with an average size of 9.8 cm.3 -6,12 -21,23,25 These lesions develop over a long period ranging from 1 to 40 years with an average of 14 years.3 -6,12 -15,17 -25 Giant SK may be complicated with ulcerations and unpleasant smell.5,12,13
Clinical and pathological features of reported cases of giant seborrheic keratosis (1964-2020) (PubMed search).

Abbreviations: F, female; M, male; NA, not available; SK, seborrheic keratosis.
In addition to giant size, unusual clinical features of SK may include serpiginous presentation, target-like pattern, and unusual location such as the external ear canal, and subungal location.26 -29
Clinical misdiagnoses of SK include melanoma, invasive squamous cell carcinoma, and basal cell carcinoma. 2 In addition, Mochizuki et al reported the case of a giant irritated SK of the back simulating verrucous carcinoma. 14 Genital giant SK may mimic condyloma acuminata, acrochordons, Bowenoid papulosis, and extramammary Paget’s disease.4,6,17 -20,23,24
Usual dermoscopic features, unusual dermoscopic features, and dermoscopic misdiagnosis
The main limitation of our work is that dermoscopy was not performed. Truth to say, dermoscopy is the preferred non-invasive diagnostic method especially in distinguishing pigmented SK from other pigmented tumors. 1
Typical dermoscopic features of SK include fissures and ridges imparting a cerberiform appearance, hairpin vessels with white halo, milia-like cysts, and comedo-like openings. 2 Dermoscopy of giant lesions appears to show typical features of SK.4,20,23 Moreover, Alapatt et al, 21 described a case of a giant SK of 7 × 6 cm with dermoscopy showing a “parched paddy field appearance.” Zhang et al 25 reported the case of giant SK of the head with dermoscopy showing irregular brown and bluish pigment and “fat finger” structure.
Furthermore, in a review of 161 excised difficult-to-diagnose SK, 10 repetitive global dermoscopic patterns were identified: multicomponent (32; 19.9%), reticular (24; 14.9%), bowenoid (21; 13.0%), hairpin (19; 11.8%), keratoacanthoma-like (16; 9.9%), blue-nevus like (15; 9.3%), lichenoid (6; 3.7%), hyperkeratotic (6; 3.7%), clonal (5; 3.1%), and spitzoid (5; 3.1%). In addition, 12 SK (7.5%) were not included in any of such patterns (not classified). 30
These unusual dermoscopic patterns reflect the variability of a common cutaneous benign disease.
Dermoscopic misdiagnosis of SK include SCC, melanoma, and BCC.31 -33
Dermoscopic features of SCC include dotted vessels, branched linear vessels, white structureless areas, and white circles surrounding follicles. 31 Dermoscopic distinctive features of melanoma include the presence of blue-white veil, pseudopods, streaks, and pigment network. 32 In addition, when a starbust pattern is dermoscopically present, a histopathological examination is indicated to rule out a spitzoid melanoma. 2 BCC is characterized by the presence of blue-gray globules, maple leaf-like areas, spoke-wheel areas, and arborizing telangiectasias. 33
Usual histological features, unusual histological features, and histological differential diagnoses
Histologically, SK is characterized by the presence of two keratinocytic components: basaloid cells and monomorphous squamous epithelial cells. In addition, there is epidermal acanthosis, papillomatosis, hyperkeratosis, and horn pseudocysts, which are the microscopic traduction of dermoscopic comedo-like openings.2,7
Histological variants of SK include acanthotic, hyperkeratotic (verrucous), adenoid, clonal, irritated, and melanoacanthoma. 7
Acanthotic SK is the most common variant. This subtype involves pronounced acanthosis with moderate papillomatosis and hyperkeratosis. Horn pseudocysts are numerous. The hyperkeratotic subtype is characterized by marked papillomatosis with saw-tooth appearance, hyperkeratosis, and moderate acanthosis. Adenoid SK is typified by reticular proliferation of basaloid cells arising from the epidermis. Hyperpigmentation is not uncommon. In the clonal subtype, there is proliferation of sharply demarcated intraepithelial clusters of basaloid cells, which is known as the Borst-Jadassohn phenomenon. Irritated SK has an inflammatory cell infiltrate in the dermis and it is characterized by numerous squamous eddies. Therefore, this variant has to be distinguished from SCC. Melanoacanthoma refers to a very heavily pigmented acanthotic SK.1,7,34,35
Unusual histological features of SK include sebaceous differentiation, basal clear cells, in addition to adamantinoid pattern and pseudorosette formation.35 -37
In addition to SCC, histological differential diagnoses include epidermal nevi, confluent and reticulated papillomatosis, acanthosis nigricans, and acrokeratosis verruciformis.1,2,7
The pathogenesis of SK
Despite being so common, the etiology of SK remains not clearly elucidated. 8 The pathogenesis is suggested to be related to skin aging and chronic ultraviolet (UV) exposure.1,7 Moreover, genetic predisposition and Human Papilloma Virus infection may represent a risk factor for SK. 8 Besides, it has been postulated that SK may be linked to the accumulation of amyloid-associated protein. 10
Clonality analyses demonstrated that SK is monoclonal representing therefore a true neoplasm rather than a simple epidermal hyperplasia. 7 Cytogenetic alterations include FGFR3, PIK3CA, TERT promoter, and DPH3 promoter mutations. 1
SK and malignancy
SK is a benign condition. However, reports of associated Bowen’s disease, invasive squamous cell carcinoma, basal cell carcinoma, and melanoma arising within SK have been described.9,11,38 -40 Nevertheless, whether these lesions represent collision tumors or can develop directly from SK is still debatable.7,9,11,40
In our case, the specimen was entirely analyzed and there was no histological evidence for associated malignancy.
Treatment
Due to the benign nature of SK, treatment is usually not required. 41 However, patients with SK are often motivated to get treated for physical irritation or cosmetic reasons.1,7
Therapeutic modalities of SK include shave surgery, cryosurgery, laser-assisted removal, and topical therapies.1,41 Complete surgical excision remains the treatment of choice of giant SK providing both diagnostic confirmation and therapeutic benefit.3 -5 As per reported cases, in addition to surgical treatment, therapeutic approaches of giant SK may encompass topical fluorouracil, dermabrasion, liquid nitrogen cryotherapy, electrocoagulation curettage, carbon dioxide laser ablation, and aminolevulinate photodynamic therapy.4,5,13,15,16,18,19,25
Conclusion
Seborrheic keratosis (SK) is a benign common skin lesion. Accurate diagnosis is usually straightforward based on quite distinctive clinical features. However, clinical appearance may be equivocal resulting in diagnostic difficulties. Giant lesions represent a rare occurrence. In this regard, histopathological examination is essential to confirm the diagnosis, rule out malignancy, and guide appropriate management. Surgical excision of giant (SK) remains the standard of treatment providing both diagnostic confirmation and therapeutic benefit.
Footnotes
Acknowledgements
None.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations
SK: seborrheic keratosis
SCC: squamous cell carcinoma
Author Contributions
Drafting of the manuscript: Bahaeddine Lahbacha and Abir Chaabane. Acquisition, analysis, and interpretation of data: Bahaeddine Lahbacha, Salwa Nechi, Amina Bani, and Majdi Kchaou. Critical revision and literature review for important intellectual content: Fadhel Chtourou, Mohamed Karim Mfarrej, Amel Douggaz, and Emna Chelbi. Study conception and design: Salwa Nechi, Abir Chaabane, Fadhel Chtourou, Mohamed Karim Mfarrej, Amel Douggaz, and Emna Chelbi. All authors approved the final version.
Ethical Approval
Not applicable.
Consent
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
All data generated or analyzed during this case are included in this article. Further enquiries can be directed to the corresponding author.