
Abstract
Histoplasmosis is an endemic infection caused by Histoplasma capsulatum, leading to a broad spectrum of disease from asymptomatic to severe disseminated disease. To diagnose Histoplasmosis, culture remains the gold standard for the laboratory diagnosis; however, this fungus grows slowly, taking a long time 2 to 3 weeks or may take up to 8 weeks. Therefore, some other methods such as bone marrow examination play an essential role in rapid identification and early diagnosis, especially in cases of severe disseminated disease. In this case, we report a 55-year-old man with a 1-year history of gout, self-medicating (including Medrol) who was admitted to the hospital because of persistent fever and swelling of his left arm. About laboratory investigation, there was a bicytopenia (RBC and PLT), blood and pus cultures many times were negative. On the slide of the bone marrow specimen, images of yeast suspected of Histoplasma capsulatum were observed. Therefore, the patient was treated with antifungal medication, and the culture was repeated with prolonged follow-up time and positive results with H. capsulatum after 16 days. In conclusion, bone marrow test plays a significant role in the diagnosis of some fungal infections, which can contribute to an early diagnosis, especially in cases of culture and serological tests are not available or cannot be performed. Patients who present with fever and bicytopenia or pancytopenia should be performed early bone marrow test, which can support the earlier diagnosis to have appropriate treatment.
Introduction
Histoplasmosis is an endemic infection caused by Histoplasma capsulatum, leading to a wide spectrum of disease from asymptomatic to severe disseminated disease.1 -3 Most patients usually only present with mild symptoms and self-limiting infection, but immunocompromised individuals (such as HIV infection, transplant recipients, immunosuppressive treatment, or neoplasms) may develop a severe and life-threatening illness by disseminated Histoplasmosis involving various tissues and organs of the body like bone marrow, liver, skin or mucous membrane.2,4
To diagnose Histoplasma infection, culture remains the gold standard for laboratory diagnosis but it often takes a long time 2 to 3 weeks or may take up to 8 weeks because of slow growth.5,6 Therefore, it leads to many cases are reported negative culture results and missed diagnosis because the follow-up period of culture specimen is usually only 1 week. In this issue, some other methods such as serology or bone marrow tests play an important role in rapid identification and early diagnosis, especially in cases of severe disseminated disease.
In Vietnam, the reported cases of Histoplasmosis are rare. 7 Thus, we report this case, a patient with persistent fever and swelling of the left arm, which was suggested Histoplasma infection by bone marrow analysis and confirmed by culture with prolonged follow-up. The patient was explained, agreed to participate, and signed a written consent form.
Case Presentation
A 55-year-old male patient was referred to the Center of Tropical diseases of Bach Mai Hospital with a month history of persistent high fever and swelling of his left arm. The patient had a year history of gout, and self-medicating with drugs (including Medrol). A month ago, the patient had a fever (38°C) and swelling in his left arm. He was admitted to the local hospital, and treated with an antibiotic (Clindamycin) for about 4 to 5 days, but the symptoms decreased and then relapsed. Two days before, the patient’s left arm was swollen again, and he was referred to Bach Mai hospital.
On admission, the patient was conscious, Cushing’s face, body temperature of 39°C, regular pulse rate of 84 bpm, blood pressure of 110/70 mmHg, respiration rate of 22 bpm; diffuse swelling, painful and warm when touching on his left arm. MRI (Magnetic Resonance Imaging) and ultrasound of the left arm showed diffuse abscesses in muscle and subcutaneous tissue of the left arm and left forearm, the size of the largest abscess is 48 × 90 mm. Blood test revealed mild anemia (HGB 114 g/L), slightly elevated inflammatory marker (CRP 4.41 mmg/L), and other results in Table 1. Blood culture and pus culture were negative (7 days of follow-up). Other tests for HIV, rickettsia, tuberculosis, and autoimmune diseases (such as lupus, and rheumatoid arthritis) were negative. The patient was diagnosed multiple abscesses in the left arm, was drained of the abscesses, and treated with antibiotics (Ceftazidime 6 g/day, Moxifloxacin 400 mg/day, and Vancomycin 2 g/day). After 2 weeks of treatment, the patient’s left arm reduced swelling; therefore, he was transferred to the local hospital for further monitoring.
Blood test results in Bach Mai Hospital.

A week later, the patient had a fever and pain again, and was referred to the Center of Tropical diseases of Bach Mai Hospital. Complete blood count (CBC) revealed bicytopenia (HGB 87 g/L, PLT 51 G/L) (Table 1). The patient’s case was consulted by a hematologist and was decided to perform the bone marrow examination (including aspiration and biopsy). The bone marrow aspiration smear showed an increase in macrophages which contained many pathogens suspected to be Histoplasma with characteristics such as yeast form, round or oval shape, small purple nucleus accounting for one-third of the spore (Figures 1 and 2). Based on this result, the patient was treated with Ampholip 150 mg/day; meanwhile, cultures of pus and bone marrow fluid were repeated and followed up longer. The culture results were positive for Histoplasma capsulatum after 16 days. Additionally, a PCR test for Histoplasma diagnosis was performed and positive at 318 bp primer (Table 2). After 3 weeks of treatment, the patient had no fever and reduced swelling on his arm, CBC and other tests tended to normal range.

Histoplasma in bone marrow aspiration.
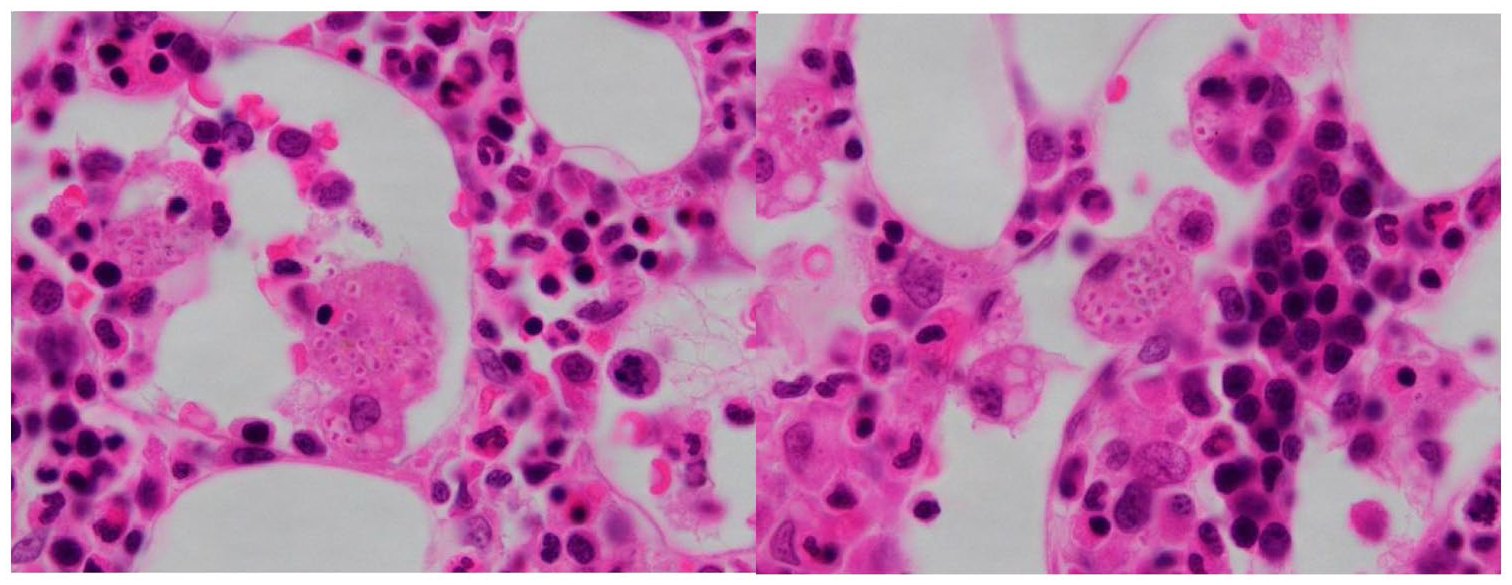
Histoplasma in bone marrow biopsy.
Histoplasma diagnostic PCR test.

Discussion
Worldwide, Histoplasmosis is most common in HIV/AIDS patients. 8 Other immunocompromised patients at risk for Histoplasmosis include transplant recipients, immunosuppressive treatment (such as steroids), and hematologic malignancies. 6 Symptoms of Histoplasmosis are variant, depending on patient characteristics, site of infection, and severity of disease, including fever, cough, fatigue, and weight loss.2,9
To laboratory diagnose of Histoplasmosis, there are several methods such as direct examination for mycology, histopathology, culture, and serology, depending on the laboratory capabilities. 5 The gold standard for the laboratory diagnosis of Histoplasmosis is still culture, however, growth of H. capsulatum is slow and usually takes 2 to 3 weeks or can last up to 8 weeks.5,6 Therefore, it is necessary to use other methods for faster diagnosis, such as serology or direct examination. Serology is useful for diagnosis but is not available in many laboratory facilities. Meanwhile, the direct examination is a simple method, allowing to provide imaging evidence of Histoplasma by analyzing the specimen under the microscope.
Histoplasmosis is caused by a dimorphic fungi Histoplasma capsulatum, presenting with a yeast form in body temperature and a hyaline mold form in the natural environment. 5 In the Wright-Giemsa staining, yeasts are round or ellipsoidal shapes, small (2-5 μm in diameter), have a purple nucleus occupied from one-third to one-half of the spore, light green cytoplasm, and surrounded by a clear halo. Most of these yeasts are intracellular (macrophage, histiocyte, neutrophil), and some may be outside macrophages.5,10 Types of specimens for this staining method depend on the clinical features of the patient, including bone marrow aspiration, puncture of lymph node, pus or exudates, cerebrospinal fluid, and peripheral blood. Thus, bone marrow analysis also plays an important role in diagnosing Histoplasma capsulatum.
In the study of Pamnani et al 2 on 4 cases of patients diagnosed with Histoplasmosis (2 HIV positive cases, 1 HIV negative case, and 1 unspecified case), all patients had fever and anemia, 3 of patients revealed thrombocytopenia, and bone marrow examination showed fungal cells in macrophages, very earlier in comparison to culture method, which sometimes takes up to 8 weeks.
The study of Qin et al 10 on 55 patients infected with P. marneifei (25 cases), H. capsulatum (10 cases), and other infectious pathogens (Mucor and Leishmania), all patients had fever and anemia, performed bone marrow tests showed fungal infection in macrophages and these results were quite early compared to culture test.
A research by Neubauer and Bodensteiner 11 showed that the sensitivity of bone marrow aspiration for Histoplasma diagnosis is quite high 67%-100%.
In this report, a patient with a history of prolonged use of Medrol could lead to an immunocompromised condition, was hospitalized for persistent fever and swelling of the left arm. In laboratory investigation, there was bicytopenia (anemia and thrombocytopenia), blood and pus cultures many times were negative, and bone marrow analysis revealed images of yeast suspected of Histoplasma. The patient was treated with antifungal medicine, a PCR test was performed with a positive primer for Histoplasma at 318 bp, and the repeated culture was positive with H. capsulatum after 16 days.
Conclusions
In general, bone marrow analysis plays an essential role in the diagnosis of some fungal infections, which can contribute to an early diagnosis, especially in cases of culture and serological tests are not available or cannot be performed. Patients hospitalized with fever and bicytopenia or pancytopenia should be performed early bone marrow test, which can support the earlier diagnosis to help patients have an opportune treatment.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Ph.D. Do Thi Vinh An: analyzing and detecting images suspecting Histoplasma in the bone marrow aspiration of the patient; contacting and advising Prof. Ph.D. MD. Cuong in the Center of Tropical diseases to treat the patient; contacting Ph.D. Ha to do diagnostic tests for the patient; was also the corresponding author during manuscript submission. Ph.D. MD. Nguyen Tuan Tung: consulting patient’s case and requesting bone marrow examination; collecting the data of the patient (personal information, clinical presentation, and test results). Ph.D. Bui Thi Viet Ha: selecting primer sequence and directly doing the diagnostic PCR test for the patient. MD. Vu Minh Tam: analyzing and detecting pathogens suspected to be Histoplasma in patient samples; contacting the Microbiology department of Bach Mai hospital to discuss this case, finding references; writing and editing manuscripts. Prof. Ph.D. MD. Do Duy Cuong: directly treating and monitoring the patient’s condition.