
Abstract
Adult hepatoblastoma is a rare tumor whose etiology and mechanisms of development are still incompletely understood. Imaging and biological tests such as AFP and liver enzymes are non-specific. Histologically, there are 2 histological variants: pure epithelial with 5 types (pure fetal, embryonal, small cell undifferentiated, cholangioblastic, and macrotrabecular), a mixed epithelial and a mesenchymal variant with or without a teratoid contingent. The main differential diagnosis concerns hepatocellular carcinoma. The treatment of hepatoblastoma in adults is not yet standardized and surgery remains the mainstay of treatment. In this report we aim to describe the clinical, pathological, and immunohistochemical features of this rare entity in adult patients and discuss the elements allowing its distinction from hepatocellular carcinoma (HCC).
Introduction
Hepatoblastoma (HB) is the most frequent liver tumor in children which accounts for 79% of pediatric malignant liver tumors but only 2% of all pediatric malignancies. The majority of cases are diagnosed within the first 3 years of life. 1 However, Hepatoblastoma is an exceptional cause of primary malignant liver tumors in adults with a very poor prognosis and a high rate of mortality. 2 Because of its rarity in adult patients, treatment for adult hepatoblastoma is not yet standardized as in children and surgery remains the mainstay of the treatment 3
In this report, we present 2 cases in young adult patients who consulted for abdominal pain.
Case Report 1
We report the case of a 26-year-old female patient with no previous history, who was admitted to the hospital because of a mass in the right hypochondrium. Abdominal MRI revealed a multiloculated cystic formation in segment VI of the liver, without intense contrast after injection with an Alpha Foeta Protein level of 2275 IU/ml. Liver function test and lactate dehydrogenase were within normal limits and hepatitis (B and C) tests were negative.
The patient underwent an S5-S6 bi-segmentectomy associated with cholecystectomy and hepatic pedicle curage.
The macroscopic examination showed several confluent nodules forming a single mass measuring 8, 7 × 6 × 5 cm in size with a crisp texture. The surface of the liver was smooth without obvious disruption. The cut surface showed a yellow lobulated lesion with areas of necrosis and hemorrhage.
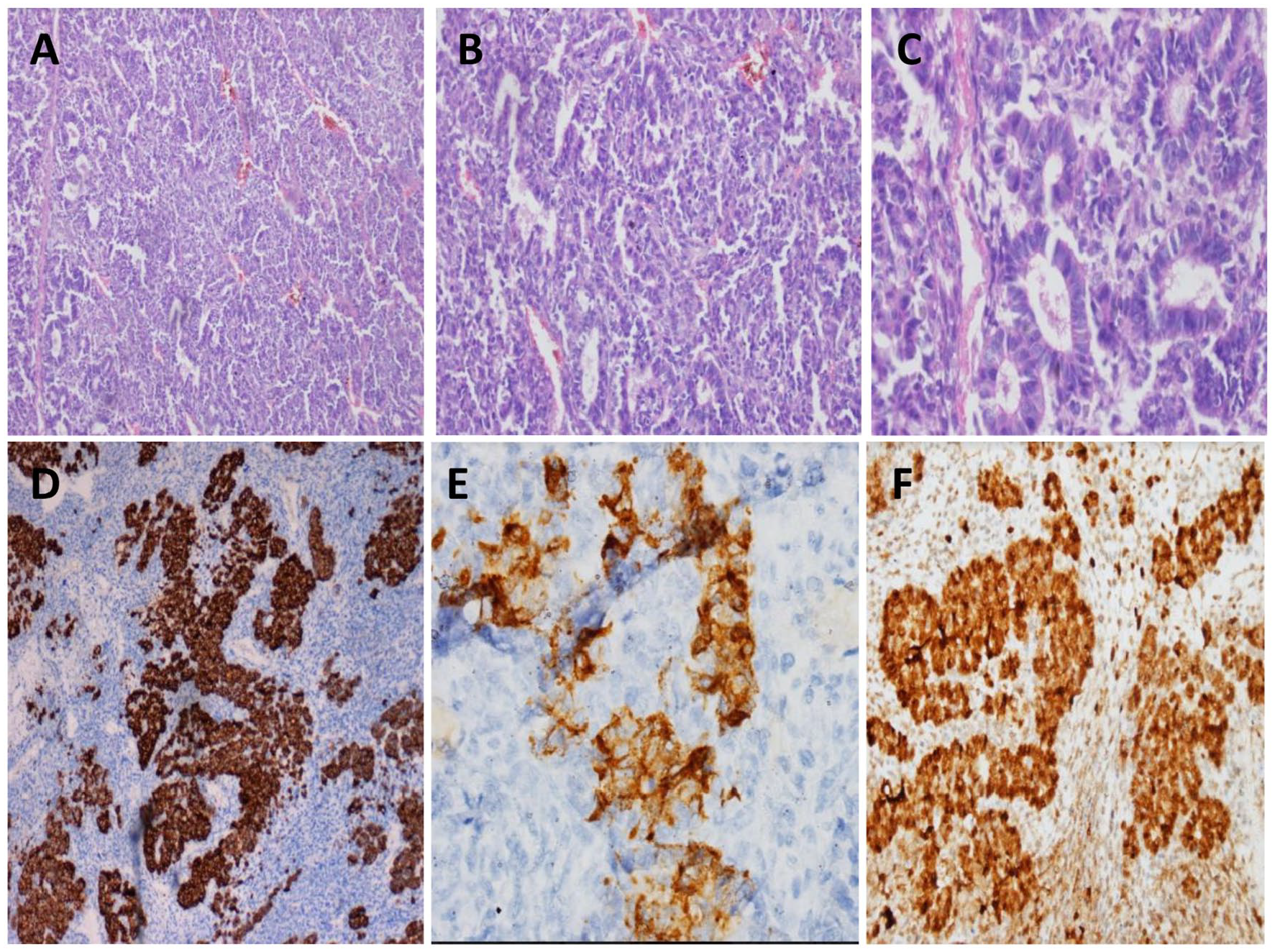
Microscopic examination showed a non-cirrhotic liver parenchyma which is the site of an epithelial proliferation with a double component .The first is formed of small and uniform cells arranged in thin trabeculae, the cytoplasm was either eosinophilic or clear with an appearance of light and dark pattern at low magnification. In the second pattern, the tumor cells were arranged in glandular, acinar or pseudorosettes structures. Mitotic activity was low in the epithelial component but high in the mesenchymal component. Tumor cells, resembling blastemal cells, showed a dark and scant cytoplasm with large nuclei. Immunostaining showed positive labeling of the cells with anti-hepatocyte and anti-glypican3 antibodies in both components. Tumor cells were negative for chromogranine and synaptophysin (Figure 1).

(A) Hepatoblastoma with fetal and embryonal pattern (HE ×40). (B) The fetal component is formed of small and uniform cells with clear or eosinophilic cytoplasm (HE ×400). (C) The embryonal component is composed of cells resembling blastemal cells with dark and scant cytoplasm and large nuclei (HE ×400). Tumor cells show : (D) Cytoplasmic and membranous b-catenin staining (×400). (E) Strong coarse granular glypican 3 staining (HE ×200) and (F) GS diffuse strong cytoplasmic staining( HE ×200).
The final diagnosis was mixed fetal and embryonic epithelial hepatoblastoma.
The patient was referred to the oncology department for chemotherapy.
Case Report 2
The second patient was an alcoholic 50-year-old male, who presented to the emergency department with a complaint of acute abdominal pain. Physical examination revealed severe abdominal distension. Abdominal computed tomography (CT) showed a large lobulated solid mass involving the entire liver with intra-abdominal fluid accumulation. A ruptured hepatic tumor with massive internal bleeding was suspected. At the time of diagnosis, routine blood investigations including liver function tests were all within normal ranges. Screening for viral markers was negative. The baseline serum alpha fetoprotein (AFP) was elevated (6386 ng/ml). They had urgently taken him to the operating room where an exploratory laparotomy was performed and good hemostasis was obtained after blood transfusion.
We received pre-operative fragmented liver biopsies. Histopathological examination revealed that the tumor is composed exclusively of immature hepatocytic elements and made up of mesenchymal and epithelial cells. The epithelial component is characterized by a fetal and embryonal pattern. The tumor cells were grouped in nests, islands, and broad trabeculae with a small round nucleus and finely granular eosinophilic cytoplasm. Some areas showed glandular configuration, acini and rosette formation, with brisk mitotic activity. The mesenchymal component comprised spindle oval cells with minimal cytoplasm, myxoid degeneration and necrosis. There was no evidence of extramedullary hematopoiesis or lymphovascular invasion.
Immunohistochemical stainings showed that the tumor cells were positive for synaptophysin and chromogranin A, but negative for panCk, Ck7, Ck20, and PLAP. Scattered cells showed positive staining of EMA.β-catenin staining exhibited a mixed nuclear and cytoplasmic pattern of the tumor cells (Figure 2).These pathology results were consistent with the diagnosis of a mixed hepatoblastoma. Following laparatomy, the patient was treated with adjuvant chemotherapy and surgical resection was planned.
(A) Mixed hepatoblastoma composed of mesenchymal and epithelial cells.(HE ×100). (B) The epithelial component is characterized by cells grouped in nests, islands, and broad trabeculae (HE ×200). (C) Some areas showed glandular and rosette formation (HE ×400) (D) Tumor cells are positive for synaptophysin (×40) (E), and chromogranin A (×400). (F), β-catenin staining exhibit a mixed nuclear and cytoplasmic pattern of the tumor cells (×200).
Discussion
In children, HB is the most frequent primary malignant liver neoplasm with a significant increase in incidence per year. It occurs typically in patients under 5 years (91% of liver malignancies ). Only 5% of HBs are in patients aged >4 years. The average age at diagnosis ranges from 12 to 21 months4,5
The etiology and mechanisms of hepatoblastoma are still unclear. However, several risk factors have been described such as prematurity, very low birth weight (<1500 g), maternal and paternal preconceptional and gestational tobacco smoking. 6
Reports of children hepatoblastoma cases revealed that this pathology can be associated with genetic syndromes specifically Beckwith-Wiedemann syndrome, hemihypertrophy, Prader-Willi, Simpson-Golabi-Behmel, Aicardi (X-linked mutation), trisomy 18 and Familial adenomatous polyposis. 7
In Adults, hepatoblastoma is an uncommon liver tumor. The first case of this tumor in a young man was reported in 1958. . Only 69 cases of this pathology have been recognized in the literature up to December 2018.
A review of 63 cases of hepatoblastoma in adults by Celotti et al published in 2016, revealed that the age of the patients reported ranged from 18 to 84, with a median age of 42 years. The ratio male: female was 1. Only in 49 articles sex was specified : 24 patients males and 25 females. 8
A subsequent study published in 2019 added 6 new cases reported in the literature from 2016 to December 2018.
Different investigations of genetic abnormalities in HB revealed different alterations such us alteration of the wnt/β-catenin signaling pathway including mutations in CTNNB1, AXIN1, APC and., p53. 9 The insulin growth factor 2 (IGF2) pathway is activated by genetic or epigenetic events such as allelic deletion of chromosome 11p15.5.10,11 Upregulation of cell-cycle pathway and loss of checkpoint contrôle (including PLK1-CDKN2A-CDKN1B), microsatellite instability and many other molecular abnormalities were also found. 9 Moreover, these tumors show few chromosomal abnormalities.
The most common are trisomies of chromosomes 2, 8, and 20, the gain of chromosome 22 and rearrangements or translocations affecting chromosomes 1q, 2, and 4q. 12
The revealing sign of hepatoblastoma is usually the right upper quadrant abdominal pain or the presence of abdominal mass .Other clinical symptoms included hemoperitoneum due to rupture of the tumor, massive gastrointestinal bleeding, 13 fever, vomiting, loss of energy, norexia, and loss of weight. HB can be well tolerated by patients and has few symptoms 2
In the literature, laboratory studies including blood count, liver function test, lactate dehydrogenase and, serological heptatitis revealed nonspecific results. 14 Alpha-fetoprotein (AFP) with hepatoblastoma is usually increased, however some patients can have normal or low AFP level like hepatocellular carcinoma. 15
Hepatoblastoma in adults are usually located in the right lobe and occur in non-cirrhotic liver chronic.
The radiological investigations, including abdominal ultrasonography, axial tomography and magnetic resonance imaging, may show single or multiple lesions. Tumors may appear as a large nodular mass surrounded by a fine fibrous capsule, pseudocapsule or with indistinct margins. Calcifications, hemorrhage and necrosis were noted in some cases. 3
Generally, imaging is not useful for the diagnosis of hepatoblastoma because there are no specific radiological signs of hepatoblastoma and different types of liver tumor, such as HCC, presented the same characteristics8 -13
However imaging is particularly useful to evaluate pulmonary metastasis and lymph node status. 6
Hepatocellular carcinoma is the main differential diagnosis. The differentiation between these 2 entities may be difficult because of the lack of particular clinical signs and radiological features. Histological study plays a key role in this distinction. The main histological criteria to distinguish HB from HCC are the presence of “light and dark” pattern, extramedullary hematopoiesis and mesenchymal elements. 3
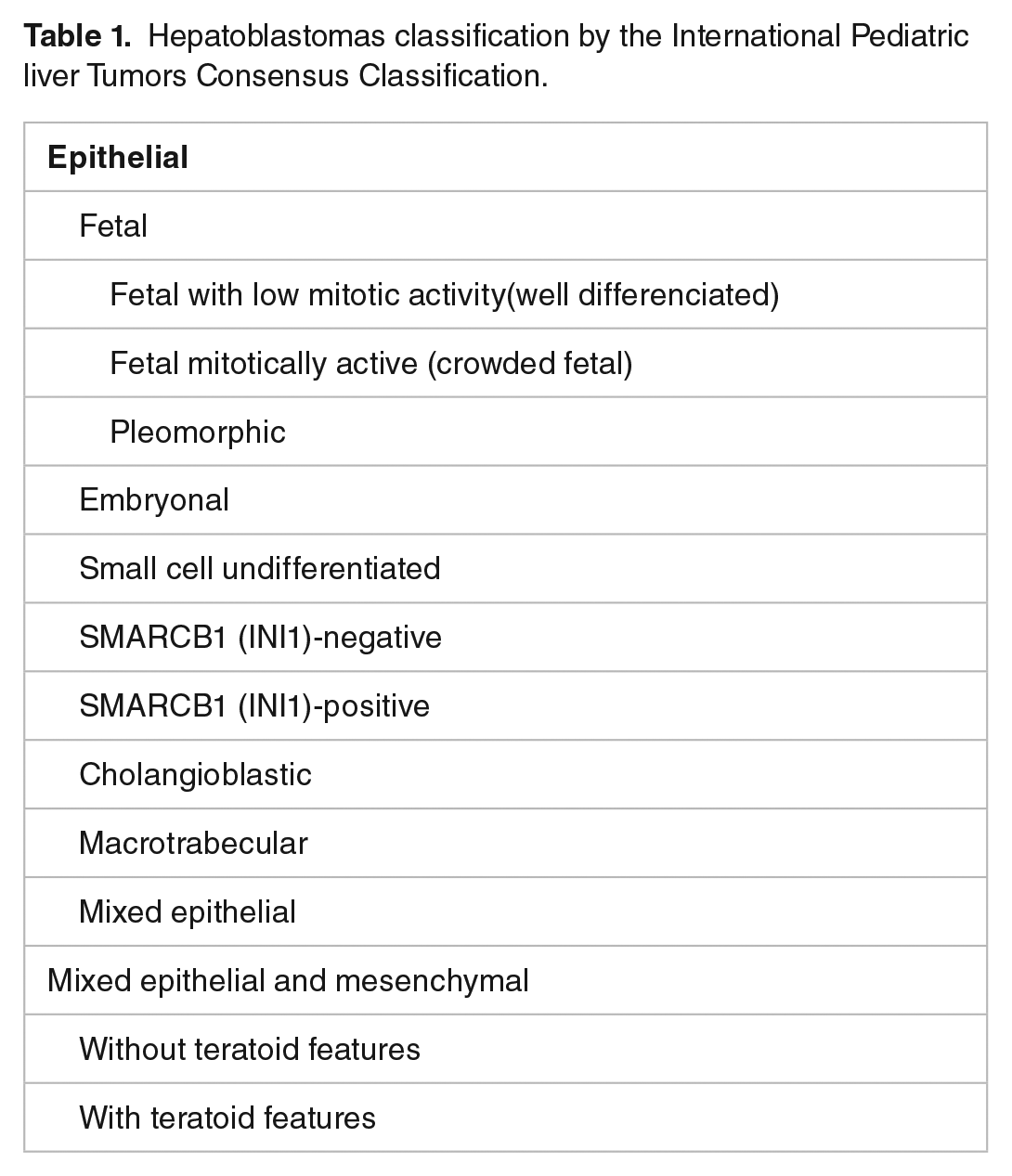
Hepatoblastomas are classified by the International Pediatric liver Tumors Consensus Classification as either epithelial or mixed epithelial and mesenchymal. (Table 1) It is based on the histological classification of HB originally proposed by Ishak and Glunz in 1967. 9
Hepatoblastomas classification by the International Pediatric liver Tumors Consensus Classification.
Epithelial hepatoblastoma
Histologically, the tumor consists of irregular lobules delineated by septa of varying thicknesses. These septa are composed of mature collagenous fibers, and contain usually venous vessels and lymphatics. 16
It can be subdivided into:
Immunohistochemically, tumor cells are strongly positive for glutamine synthetase (GS), and show finely granular staining with glypican 3 (GPC3).b-catenin (b-cat) is frequently membranous and even cytoplasmic, with rare nuclear staining. Hep-Par1 and AFP are also positive.
The “crowded” or mitotically active fetal HB has the fetal aspects described above. It is specifically defined by a mitotic index of more than 2 mitoses per 10 fields at high magnification. The pleiomorphic fetal is defined by nuclear pleiomorphism with anisokaryosis and multinucleated cells.1 -9
The Immunostains show strong positivity for GPC3 in a diffuse, coarse, cytoplasmic staining pattern and GS. Many positive nuclei for b-cat are seen. Hep-Par1 and AFP are positive.
Fetal and embryonal epithelial patterns are usually associated.1 -16
Immunohistochemistry, tumor cells show AFP and nuclear b-cat positivity. GS is variable. GPC3 is also variable, it may be absent or show strong, coarse, diffuse cytoplasmic staining. Ki67 is high.
Immunohistochemically, the SCUD pattern shows strong and diffuse nuclear b-catenin stain; it expresses also pancytokeratin, cytokeratin 19, and vimentin; in contrast it is negative for Hep Par 1, AFP, GS, and GPC3.
Tumor cells of cholangioblastic pattern show nuclear b-catenin stain, which is not seen in the reactive ductular population. These cells are also positive for CK7, CK19 but negative for GS and GPC3.
The Immunostains show strong nuclear b-cat expression. INI 1 is also positive as is the case with all hepatoblastoma components.1 -16
Mixed epithelial and mesenchymal hepatoblastoma
It is characterized by the association of mesenchymal and epithelial elements .The mesenchymal components may be composed of fibrous, osteoid and cartilage tissue. Mixed hepatoblastoma may present teratoid features composed of the endodermal (glandular, endocrinoid), neuroectodermal (glial elements, neuronal cells) or complex mesenchymal tissues (striated muscle).
It express a nuclear b-catenin stain. Mixed epiyhelial and mesenchymal hepatoblastoma with teratoid features show variable result depending on the components.1 –17
Due to the rarity of hepatoblastoma in adults, there is no standardized management of adult HB. Surgery is the mainstay of treatment. It aims for complete tumor resection. Although, some tumors are so big or extensive and cannot be completely removed3,15 Liver transplantation can be considered in these cases. 3 Surgery can be combined with chemotherapy as adopted in children, Cisplatin is the most commonly used chemotherapeutic agent. 15 Preoperative chemotherapy can be used to reduce the volume of unresectable tumors that are too big for conventional surgery.2,16
Conclusion
Adult hepatoblastoma is a rare entity with a poor prognosis, whose diagnosis is based on histology given the non-specific clinical, radiological and biological picture. The optimal treatment remains to be defined due to the limited data available.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
IE and EH analyzed and interpreted the patient data and wrote the manuscript. IE made the figures. IE performed the histological examination. BS and EB proposed the study, supervised IE and revised the manuscript. All authors read and approved the final manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Consent for Publication
Written consent has been obtained from the patient and the patient’s family for the publication of this case report.
Guarantor
Ihssan Elouarith