
Abstract
Introduction:
Adenosquamous carcinoma (ASC) is a rare subtype of the conventional adenocarcinoma of the bile duct. The clinico-pathological characteristics of this entity are poorly understood partly due to its rarity.
Case Summary:
A 67-year-old ASA II male presented with obstructive jaundice subsequently complicated by cholangitis. CT abdomen showed dilatation of the intra and extrahepatic biliary tree. Endoscopic retrograde cholangiopancreatography revealed a stricture with a mucosal growth at the ampulla of Vater. He had a pancreaticoduodenectomy and the distal common bile duct tumour identified in the specimen was on histology an adenosquamous carcinoma (ASC) of the extrahepatic bile duct.
Discussion:
ASCs are considered to have more aggressive tumour biology compared to adenocarcinomas. The presence of a squamous component at the invasive front relates to its poor prognosis. Surgery is the curative option, but with a high propensity for early recurrence and distant metastases. The scarcity of reports on the clinicopathological course of ASC have resulted in a lack of standardised care pathways.
Conclusion:
A better understanding of the clinicopathological characteristics, biological behaviour and disease progression of ASC will aid therapeutic options and prognostication.
Background
Adenosquamous carcinoma (ASC) first described in 1907, 1 has both glandular and squamous elements that are histologically malignant. It is a rare histological subtype of adenocarcinoma that occurs in glandular epithelium. The incidence of extrahepatic cholangiocarcinoma (ECC) varies from 0.5 to 2 cases per 100 000 person-years, with a higher incidence in Asia and North America.2,3 More than 90% of ECCs are adenocarcinomas and ASC with its greater malignant potential accounts for only around 2%.4-6
Preoperative diagnosis of the ASC is rare since yield from biopsies are poor and decisions on surgery are largely based on clinic-radiological features. Where a biopsy is available, it may represent only 1 of the 2 malignant components. 7
Only few cases of ASC have been reported to date1,6,8,9 and population-based studies are also limited.3,4,10,11 We report a case of ASC of the distal CBD and discuss the relevant literature. Informed written consent was obtained from the patient.
Case Presentation
A 67-year-old, ASA 2 male with diabetes mellitus, hypertension, ischaemic heart disease and dyslipidaemia was investigated for obstructive jaundice, subsequently complicated by a spontaneous cholangitis. In addition to deranged LFTs his haemoglobin was 6.6 g/dL. Abdominal CT showed dilated intra and extrahepatic bile ducts (CBD 1.8 cm) with a normal liver and no pancreatic lesions. The pancreatic duct was not dilated (Figure 1).

CT axial plane (A) and coronal plane (B) showing dilated gallbladder and extrahepatic biliary system indicated by arrow heads.
Endoscopic retrograde cholangio-pancreaticography (ERCP) revealed a bulging ampulla with a tight ampullary stricture and an 8 Fr × 10 cm plastic biliary stent was inserted. An ampullary biopsy obtained during the procedure showed histologically unremarkable duodenal mucosa.
Following optimisation of comorbidities and prehabilitation he underwent a classical pancreaticoduodenectomy. Histological assessment of the specimen and hepatic lymph nodes was done.
On macroscopic examination, the common bile duct (CBD) wall was thickened along its course from the transection margin to the ampulla of Vater. An ampullary mucosal bulge was observed protruding into the duodenal lumen. Cut sections through the pancreatic head revealed a 16 × 12 × 10 mm irregular, firm, white tumour just beneath the duodenal mucosa arising from the common bile duct close to the junction with the main pancreatic duct (Figure 2).
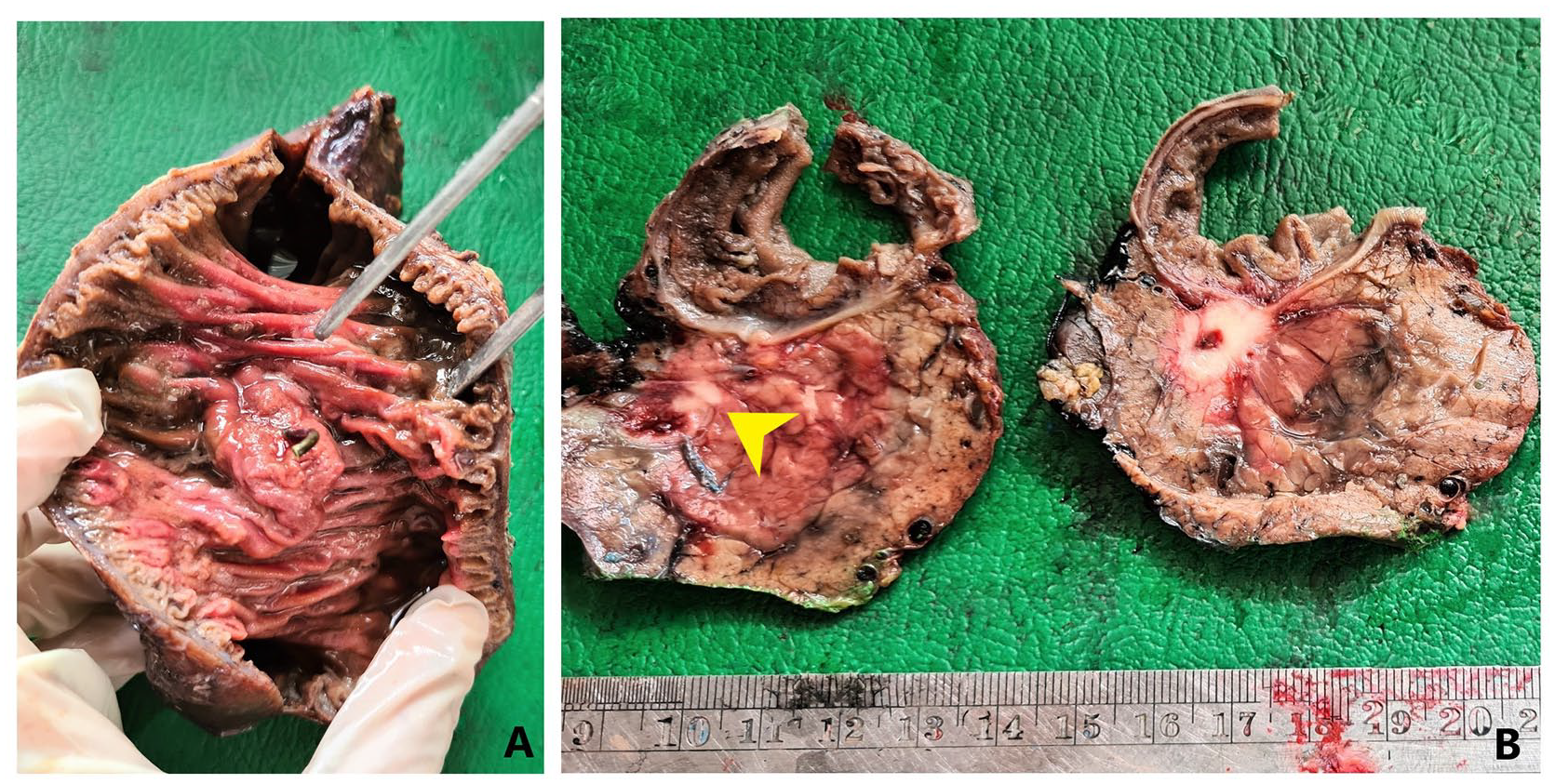
(A) Macroscopic view of the mucosal bulge at the ampulla of Vater and (B) cut sections through the pancreatic head reveal an irregular white tumour arising from common bile duct (arrowhead).
Microscopy revealed an adenosquamous carcinoma arising from the intrapancreatic CBD. The tumour exhibited a predominance of moderately differentiated irregular glands (75%) diversely merging with sheets and islands of atypical squamoid cells (25%). The tumour showed co-expression of CK7 and CK 5/6 (Figure 3). It extended through the ampullary duct to involve the duodenal mucosa at the major papilla. The CBD resection margin showed high-grade biliary intra-epithelial neoplasia. The tumour also exhibited pancreatic parenchymal invasion, lympho-vascular and perineural invasion, and regional lymph node metastases of squamous elements. The tumour stage was assigned as pT2 pN1 (stage group IIB).

Microscopic view of AC and SCC junction ((A) – H&E section ×100 magnification; (B) – H&E section ×200 magnification), (C) immunohistochemistry showing co-expression of CK7 in the AC component (×40 magnification), (D) immunohistochemistry showing co-expression of CK5/6 in the SCC component (×100 magnification).
Post-operatively the patient developed a grade B pancreatic fistula that resolved with percutaneous drainage and octreotide therapy. This was further complicated by an acute coronary event leading to left ventricular failure, bilateral bronchopneumonia and acute kidney injury all of which resolved with medical therapy. Unfortunately, he succumbed to a brainstem haemorrhage the 46th day after surgery.
Discussion
Adenosquamous carcinomas (ASC) are tumours composed of both glandular and squamous malignant elements. This needs to be distinguished from adenocarcinoma with areas of benign squamous metaplasia, which is largely caused by chronic inflammation, gallstones or choledochal cysts undergoing malignant transformation. 2 The pathogenesis of ASC remains uncertain. There are 4 prevailing hypotheses regarding its histogenesis (i) activation of pluripotent stem cells which have the capacity to induce the malignant transformation of both epithelial components; (ii) squamous metaplasia of the intestinal mucosa progressing to malignancy; (iii) adenocarcinoma transforming into squamous cell carcinoma; and (iv) collision/co-existence of both malignant tumours.1,12 The current consensus is that ASCs occur through metaplastic malignant squamous transformation of adenocarcinomas. 13 This is supported by the histopathological findings in the reported case which showed heterogeneous distribution and amalgamation of the malignant squamous and adenocarcinomatous elements. Neither squamous metaplasia in the adjacent non-neoplastic epithelium nor a transition from squamous metaplasia to squamous cell carcinoma was observed.
Although ASC-ECC shows a wide age distribution, 3 it typically affects patients in their 60s. There is an equal sex distribution 3 with a slight female preponderance.4,10 It has a higher incidence in Asia, particularly in Korea and Thailand, followed by North America.2,6
The proportion of each malignant epithelial component required for the diagnosis of ASC, differs according to the sites of origin. Although for ASC of pancreas, a minimum of 30% of either component is expected, no such criteria have been established for ASC of bile duct.2,9 The squamous component has been reported to range from 15% to 95% of the tumour mass. 4 Both the components in ASC are frequently moderately differentiated. Lymph node metastases may show an adenocarcinoma component, a squamous cell component or a mixture of the two components.4,7
ASC is regarded as a more aggressive tumour with a less favourable prognosis than its adenocarcinoma counterparts.3,4 The poor survival for patients with ASC may be due in part to it association with more aggressive pathological features including deeper invasion, frequent duodenal invasion, and higher disease stage. 4 A population-based study including cases identified from the Surveillance Epidemiology and End Results (SEER) data base between 1973 and 2013 reported the overall 1-, 2- and 5-year survival rates for patients with ASC ECC as 30.1%, 11.3% and 3.7% respectively with a median survival of 6 months. 5 A study of 36 Japanese patients reported slightly better survival rates, with overall 1-, 3- and 5-year survival rates of 57%, 26% and 16%, respectively, and a median survival of 13 months. 10
Hoshimoto et al pointed out that patients with ASC of the biliary tract exhibited a higher Ki-67 proliferation index in the SCC component compared to the AC component, 11 suggesting that this may be the reason for its aggressive nature. Other studies have reported significantly shorter doubling times of SCCs compared to ACs. 13
Hong et al reported that the survival of patients with ASC-ECC was less when the proportion of the SCC component was increased. 4 They also demonstrated that survival was significantly affected by the predominant tumour type at the advancing edge in ASC, with the presence of SCC being associated with a worse survival than the presence of an adenocarcinoma. 4 A predominance of the SCC component was observed at the advancing edge of the tumour and in lympho-vascular and perineural invasion in most instances, including the current case (Figure 4).

(A) SCC component of ASC is present at the invasive front with the tumour infiltrating the pancreatic parenchyma (H&E section ×100 magnification), (B) perineural invasion by the SCC component of the ASC (H&E section ×400 magnification).
A population-based study on the clinico-pathological characteristics identified that regional involvement was more frequent than both localised disease and distant metastases in ASC of the bile duct. 3 A Japanese study conducted by Okabayashi et al found that pancreatic parenchymal invasion and regional lymph node spread predicted a significant worsening of prognosis. 10
Table 1 summarises the findings of studies conducted on the survival of ASC of extra hepatic bile duct.
Summary of the studies performed in various countries on ASC of extrahepatic bile duct and its survival.

Surgery remains the treatment of choice for resectable disease in ASC, as for adenocarcinoma,6,7 with early-stage disease showing better survival. There are no standardised regimes of management for ASC-ECC due to small numbers of reported cases and sparse data.
Table 2 summarises the treatment and survival in reported cases of ASC of extra hepatic bile ducts.
Summary of the case reports from various countries on ASC of extrahepatic bile duct and its survival.

Younger patients with early stage disease are more likely to have surgery. Radiation has not been associated with improved survival supporting Guglielmi et al’s report that curative resection of intrahepatic cholangiocarcinoma is the only therapy that can achieve long-term survival. 15 ASC is notorious for early recurrence and metastases after surgery. 1 Thus, standardised adjuvant therapy with follow-up is warranted post-surgery.
Conclusion
Adenosquamous carcinoma is a rare histological variant of bile duct cancer and has a poorer patient survival compared to adenocarcinoma. Therefore, identification of a squamous cell component in EBD tumours has important implications for prognosis. Curative surgery remains the treatment of choice in resectable cases, though long-term survival is poor. Increasing the volume of data on this tumour subtype will contribute to better understanding its natural history and targeted therapeutic options.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SK prepared the initial draft of the manuscript. DS and SS were involved in the surgical care of the patient. SK and HW were involved in the pathological diagnosis. DS, SS and HW reviewed and critically revised the manuscript. All authors read and approved the final manuscript.
Ethics Approval and Consent to Participate
The Ethics Review Committee of the authors’ institute does not require ethical approval for the case reports.Written informed consent was obtained from the patient for publication of their clinical details and clinical images. A copy of the consent form is available for review by the Editor of the journal.