
Abstract
Background:
Gastric cancer is one of the lethal cancers and there is no effective treatment for these patients and still, 5-year survival rate is about 25% to 30%. Finding reliable biomarkers for early-stage diagnosis, targeted therapy, and survival prediction is a priority in this cancer.
Objectives:
In this study we were trying to know about the molecular classification of gastric cancers in a group of patients from the South of Iran.
Patients and Methods:
In a cross sectional study, 50 specimens of gastric cancer were selected that have enough tissue to be stained by immunohistochemistry (IHC). IHC was performed for Her-2, mismatch repair genes (MLH-1, MSH-2, MSH-6, and PMS-2), and PDL-1. Frequency of positive makers was compared with survival and outcome.
Results and Conclusion:
In our study, deficient MMR (dMMR) was detected in 4 patients (8.0%). PD-L1 expression in tumor cells (TC) was observed in 1 of 4 cases (25%) with PMS2 loss. However, PD-L1 in TCs and TILs (tumor infiltrating lymphocytes) was negative in 1 case with MLH1 loss and in 3 of 4 cases with PMS2 loss, which was not statistically significant. All of our 50 cases were positive for MSH2 and MSH6, 24% of which showed TCs with PDL-1 expression and 32% of them in TIL. HER2 was positive in 2 (2/50, 4.0%) cases, among which all of the cases were positive for PD-L1 expression in TCs and TILs, respectively. However, in HER2-negative group, 26.2% (11/42) and 28.6% (12/42) of tumors were positive for PD-L1 in TCs and TILs, respectively. The expression rate of PD-L1 in HER2 negative TCs was significantly higher than that in HER2 positive TCs (P = .033). Immunohistochemistry for Her-2 was equivocal in 6 cases (12.0%) none of which expressed PD-L1 in tumor cells. In our study minimum and maximum survival times from detection of gastric cancer were 1 and 87 months, respectively. The mean ± SD and median ± SD of overall survival time were 30.69 ± 4.88 and 18 ± 1.45 months, respectively. One and 3-year survival rates of 40% and 24%, respectively. PD-L1 expression was not associated with survival, but its expression was associated with intestinal type Lauren classification and negative HER-2. PD-L1 positivity in tumor cells or tumor infiltrating lymphocytes was not an independent prognostic factor in gastric cancer.
Introduction
Gastric adenocarcinoma is one of the common gastrointestinal cancers especially in the Asian countries such as Iran. Epidemiologic studies showed that the prevalence of gastric cancer in different provinces of Iran is between 0.2 and 100 per 100 000. 1 Although the incidence of gastric cancer has been decreased worldwide in recent decades, however it is the most common cancer in some provinces of Iran such as north and northwest provinces. 2 Unlike colon cancer, there has not been significant increase in survival of the patients with gastric cancer, and it is still the second leading cause of cancer related deaths. There is no exact treatment for these patients and still, the 5-year survival rate is about 25% to 30%, this is most probably because of lack of accurate knowledge about the molecular pathways in the pathogenesis of gastric cancer. Finding reliable biomarkers for early-stage diagnosis, and targeted therapy is helpful to increase survival rate. 3 It is will known that the accumulation of multiple genetic and epigenetic alterations can lead to dysregulation of oncogenes and tumor suppressors and is considered the driver during the tumorigenesis in gastric cancer. 4 The traditional morphology-based classification cannot convey the molecular heterogeneity of gastric cancer and cannot guide clinical practice in advanced disease for determining prognosis or predicting treatment responsiveness. Although the subclassification by molecular testing might increase the complexity of classification, identifying subtypes of gastric cancer based on molecular and genetic features is necessary to select targeted treatment to increase survival rate in the patients with gastric cancer. 5 Based on previous studies, multiple molecular classification has been introduced. However, there is a need for comprehensive molecular classification that correlates with histological features, clinical outcome, and prognosis of the gastric cancer. 6 Therefore this study is designed to obtain the possible value of combination of immunohistochemical markers, Her2, PD-L1, and MMR in gastric cancers and their relationship with histopathology and patient survival. By proper classification of the gastric cancers, targeted therapy could enhance the patient’s survival.
In this study, we tried to evaluate the molecular subtypes of gastric cancer in one of the largest referral centers in South of Iran. This is the first report from Iran.
Patients and Methods
In this retrospective study, we included records of 50 patients with gastric cancer by simple randomized sampling during 2013 to 2019 in the pathology department of affiliated Hospital of Shiraz University of Medical Sciences. Only cases included that had enough tissue for immunohistochemical staining as well as those with patients’ with consent to use their tissue for research. It’s worthy to mention that the tissues used in this study were anonymous to the researchers. Therefore, the inclusion criteria included (1) Enough tissue for immunohistochemistry, (2) Patients’ consent to use their tissue for research purposes.
Immunohistochemistry (IHC) was performed on tissue samples included from 50 gastric tumors. Immunohistochemistry was performed as routine procedure (manually). Antibodies were used as Table 1 shows for Her-2, PD1/PDL1, and microsatellites (MLH1, MSH2, MSH6, and PMS2). The stained tissue sections were reviewed and scored separately by 2 pathologists who were blinded to clinical parameters (BG and FA). PD-L1 expression was classified according to the intensity and percentage of positive tumor cells. Cases with intensity scores of 2+ and 3+ in at least 10% of tumor cells were defined as PD-L1-positive tumors.6,7 A tumor was taken as d-MMR (deficient-mismatch repair), if at least one of the markers (MLH1, MSH2, MSH6, and PMS2) showed a complete loss of nuclear reactivity Background non-tumoral glands and lymphocytes were considered as internal control. The criteria used in scoring HER-2 expression by IHC in gastric adenocarcinoma was based on previous reports. 8 The HERACLES criteria of HER2 positive were used with a 3+ HER2 score in more than 50% of the tumor cells by or with a 3+ HER2 score in 10% to 50% of the tumor cells, or with a 2+ HER2 score 2 in more than 50% of the tumor cells. 9
Brief description of antibody characteristics.

Statistical analysis was carried out using statistical package for social sciences (SPSS) (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Qualitative and quantitative variables were described using frequency (percent) and mean ± Standard Deviation (SD). Different variables were compared among the 2 groups using the Chi-square and fisher test for qualitative variables and the independent t-test for quantitative variables. Kaplan-Meier method was used to estimate the overall survival. P-value ⩽.05 was considered statistically significant.
Results
PD-L1 expression in gastric cancer and its correlation with clinico-pathological features
Tables 2 and 3 show the distribution of clinicopathologic findings in patients with gastric cancer, according to tumor cells (TC) and tumor infiltrating lymphocytes (TIL) and PD-L1 (negative and positive) expression. Patients with intestinal type Lauren classification, showed higher positive rate of PD-L1 expression (P = .035).
Correlation between PDL-1 and PD-1 expression and pathologic features of the 50 cases of gastric cancer.

Correlation between PD-L1and PD-1 expression and clinical features of 50 cases of gastric cancer.
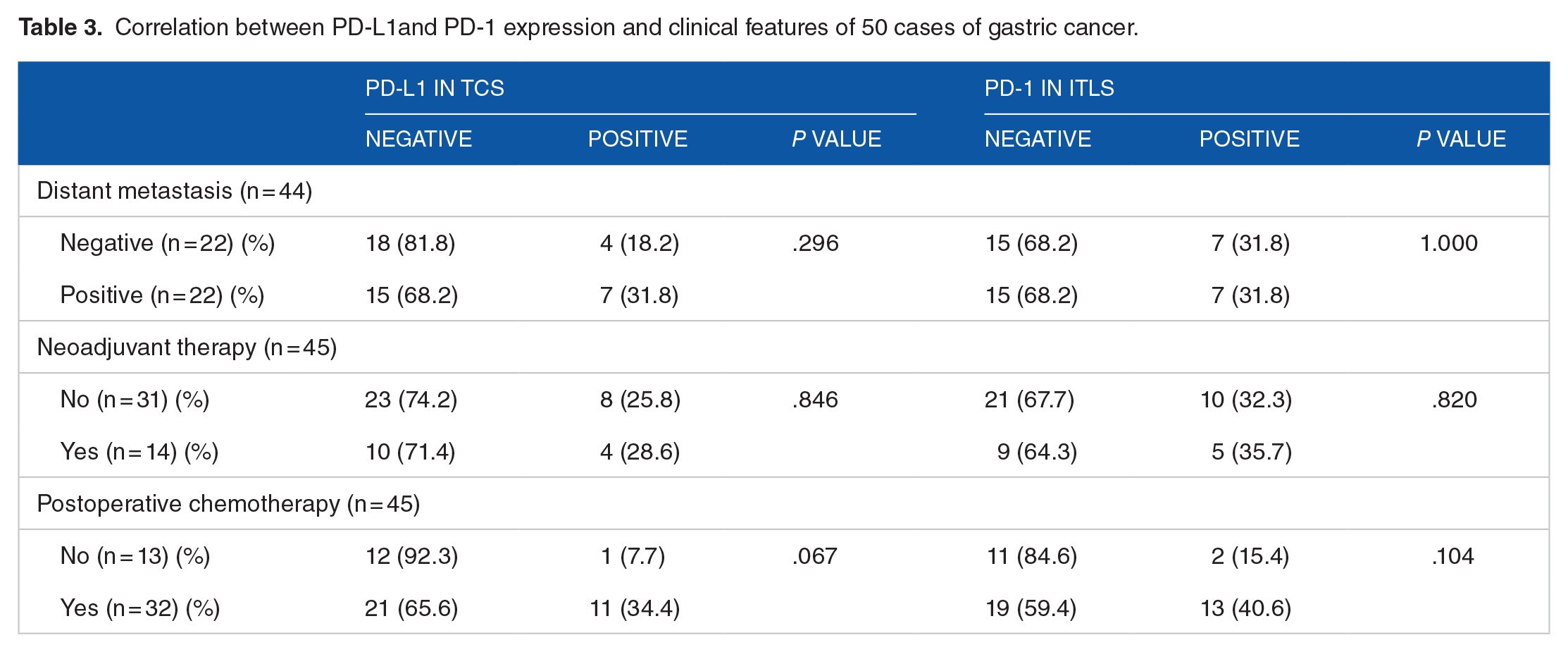
There was no statistical difference between the expression of PD-L1 (in TC and TILs) and age, gender, tumor size, tumor location, tumor differentiation, Tumor category (T1-4), lymph node metastasis, lymphovascular and perineural invasion. Clinical and therapeutic features such as distant metastasis, neoadjuvant therapy, and post operative chemotherapy showed no statistical correlation with PD-L1 expression in tumor cells and stromal lymphocytes.
PD-L1 expression in gastric cancers and MSI status
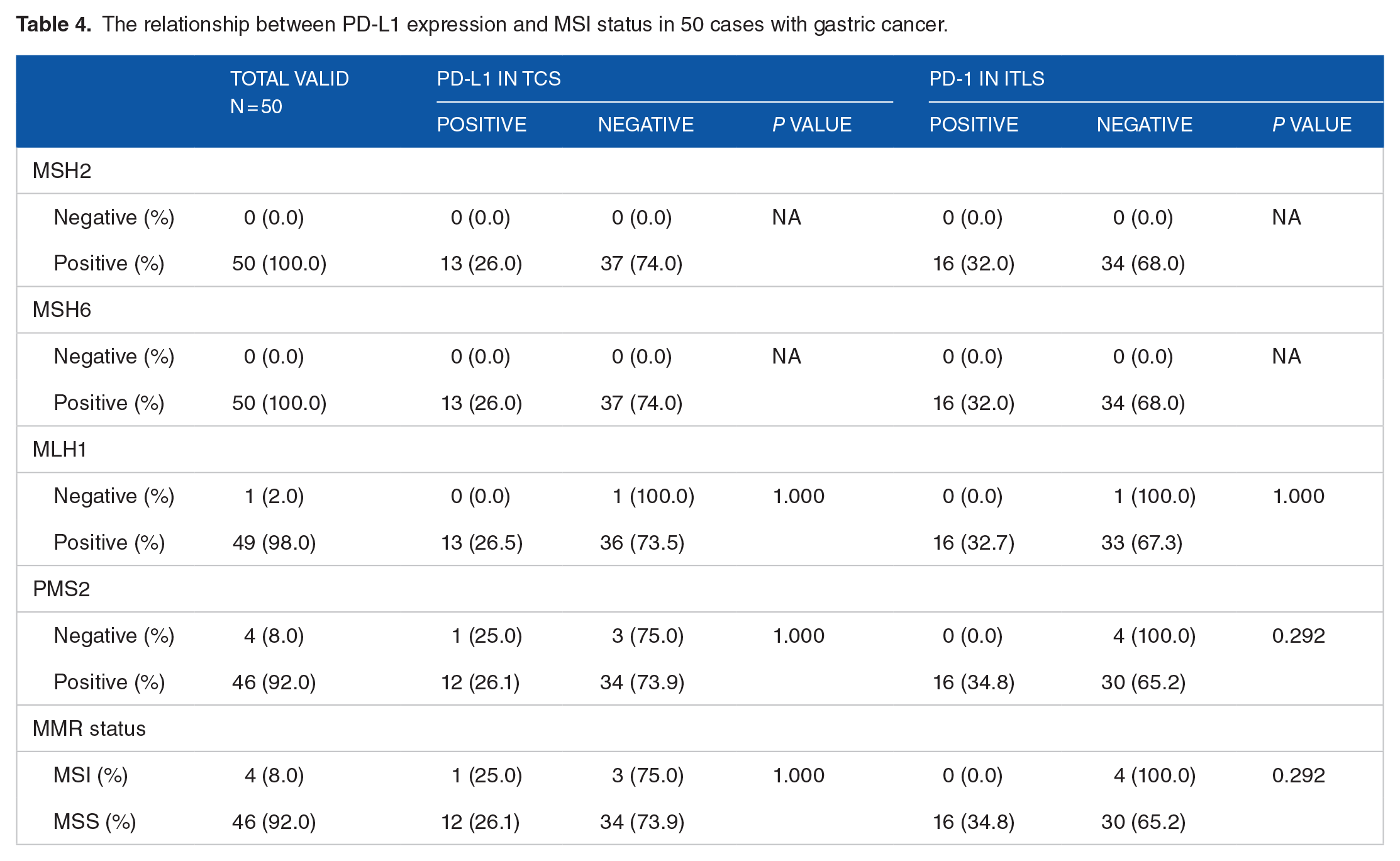
In our study, deficient MMR (dMMR) was detected in 4 patients (8.0%). As shown in Tables 4 and 5, 2% (1/50) and 8% (4/50) cases showed loss of MLH1 and PMS2 expression, respectively and none of them show the loss of expression of MSH2 and MSH6. PD-L1 expression in TCs was observed in 1 of 4 cases (25%) with PMS2 loss. However, PD-L1 in TCs and TIICs was negative in 1 case with MLH1 loss and in 3 of 4 cases with PMS2 loss, which was not statistically significant. All of our 50 cases were positive for MSH2 and MSH6, 24% of which showed tumor cells with PDL-1 expression and 32% of them in TIL.
The relationship between PD-L1 expression and MSI status in 50 cases with gastric cancer.
PD-L1 expression in gastric cancer and HER-2 status
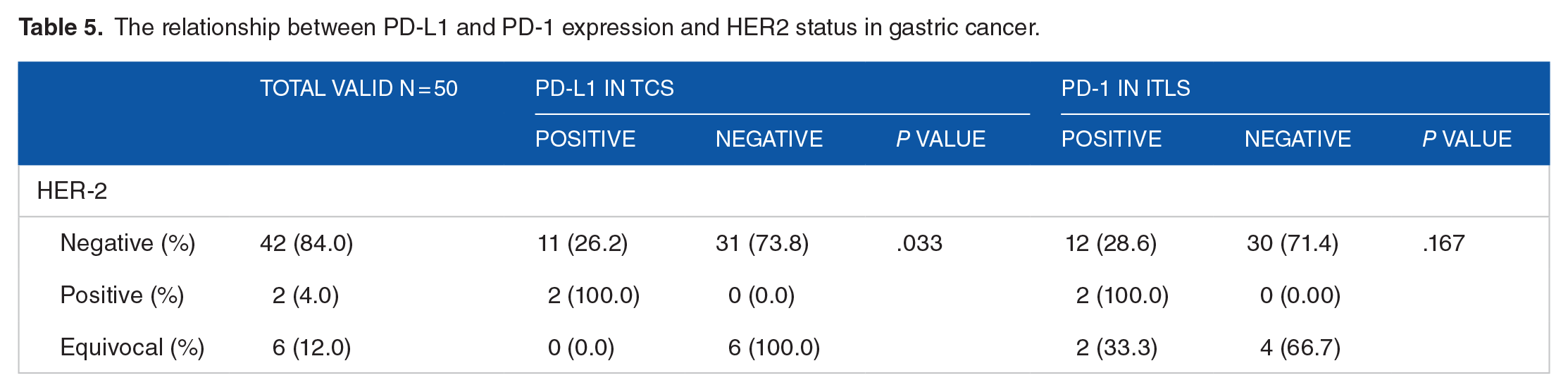
HER2 was positive in 2 (2/50, 4.0%) cases, among which all of the cases were positive for PD-L1 expression in tumor cells and stromal infiltrating tumor lymphocytes, respectively (Table 5). However, in HER2-negative group, 26.2% (11/42) and 28.6% (12/42) of tumors were positive for PD-L1 in TCs and TILs, respectively. The expression rate of PD-L1 in HER2 negative TCs was significantly higher than that in HER2 positive TCs (P = .033). Immunohistochemistry for Her-2 was equivocal in 6 cases (12.0%) none of which expressed PD-L1 in tumor cells.
The relationship between PD-L1 and PD-1 expression and HER2 status in gastric cancer.
Survival analysis
At the time of our study, 32 of 45 patients (71.1%) have passed away. Minimum and maximum survival times from detection of gastric cancer were 1 and 87 months, respectively. The mean ± SD and median ± SD of overall survival time were 30.69 ± 4.88 and 18 ± 1.45 months, respectively.
In negative PD-L1 group, 33.66 ± 6.04 months is the mean ± SD of survival time (median: 20 ± 2.54) and in positive PD-L1 group, mean of survival time is 19.39 ± 4.08 (median: 13 ± 2.59). Patients without PD-L1 expression have longer survival (P value <.05). Figures 1 and 2 shows survival plot according to PD-L1 expression.

Kaplan–Meier plot of survival according to PD-L1 expression in tumor cells.

Kaplan–Meier plot of survival according to HER-2 status in tumor cells.
Table 6 shows Means and medians survival time according to HER-2 expression (P value <.05).
Means and medians survival time for HER-2.

Survival of patients with negative HER-2 was higher than positive or equivocal HER-2 status (Figure 2).
Figure 3 shows longer survival of deficient MMR cases comparing to sufficient MMR cases with gastric cancer (38.75 ± 9.66 to 30.21 ± 5.24, P value <.05).

Kaplan–Meier plot of survival according to MMR genes in tumor cells.
Table 7 shows the summery of survival according to the expression of molecular markers.
Survival rate according to different markers.

Discussion
Gastric cancer is the leading cause of cancer related deaths worldwide. Despite of the significant progress in cancer treatment, gastric cancer is still a lethal cancer. It seems that molecular subtypes of gastric cancers show different cancer survival and therapeutic response. Studies from several groups over the past decade show multiple genomic alterations in gastric cancer, including gene mutations, somatic copy number alterations (sCNAs), structural variation and epigenetic changes. 3 The first effective molecular novelty designed by TOGA (treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer) trial demonstrated a significant improvement in overall survival with the addition of trastuzumab to chemotherapy when compared to chemotherapy alone in gastric cancers with HER-2 over expression. 3 A comprehensive study by “The Cancer Genome Atlas” (TCGA) consortium reported 4 molecular subtypes of GC: chromosomal instability (CIN), microsatellite instability-high (MSI), genomically stable, and Epstein-Barr virus (EBV) molecular subtypes. 5 However, the clinical significance of these subtypes has not been clearly clarified. The Asian Cancer Research Group (ACRG) reported 4 molecular subtypes of GC including microsatellite-stable (MSS)/TP53-, MSS/TP53+, MSI, and epithelial-to-mesenchymal transition (EMT) subtypes. 6
Our study was conducted to investigate the correlation between PD-L1 expression with MMR genes, HER-2 status, and clinico-pathological features in gastric cancer. There have been few studies analyzing combined 4 components of “tumoral PD-L1, MMR genes, and HER-2” study all together. Specifically, there has been no study from Iran that investigates the immunohistochemical expression of PD-L1 in gastric cancer.
The main and first line in treatment of gastric cancer is still chemotherapy resulting in a median overall survival (OS) of about 11 months and 5 year survival rate of about 25% to 30%.7,8
In this study, we studied 50 patients with gastric cancer for 6 years (2013-2019) from the South of Iran. According to this study, mean overall survival was 30.6 ± 4.8 months with median overall survival of about 18 months. Gill et al 10 reviewed 2043 patients with gastric adenocarcinoma and showed median survival of 13.1 months for Asians and 11.1 months for non-Asians (P = .0016). It seems that median overall survival is slightly higher for some Asian experience. Present study showed 1 and 3-year survival rates of 40% and 24%, respectively. This result was lower than Zhang et al.’s 11 study from China who has demonstrated the 1-year survival rate of 93.9% and 3-year survival rate of 77.3% among 132 surgically resected specimens of stage II and III gastric cancer. It seems that survival rate can be different in various geographic locations and ethnic populations.
PD-L1 is an important inhibitory molecule that interacts with PD-1 of T cells and blocks T cells proliferation and activity. 12 Expression of PD-L1 in tumor cells allows cancer cells to escape from host antitumor immunity. 13 There is significant variation in the reported expression of PD-L1 in gastric and gastroesophageal cancer. This variation might be due to several reasons, one of which can be the ethnical background of patients. There are discrepancies between correlation of PD-L1 expression in TC/TILs and histologic Lauren classification of gastric cancer. The present report demonstrated that PDL-1-positive tumor infiltrating lymphocytes were more commonly seen in intestinal type gastric cancer according to Lauren’s classification (P < .05). Similar findings were observed in a recent study by Choi et al 14 implied that PD-L1 expression in immune cells correlated with intestinal type of Lauren classification and may predict a better prognosis. However, PD-L1-positive tumor cells were more commonly detected in diffuse type. Pernot et al 15 suggested that diffuse type of advanced gastric cancer has lower rates of CD8+ TILs and circulating NK cells and Tregs than the intestinal type. Altogether, these findings advocated that Lauren intestinal type is a more favorable prognostic factor than diffuse type. Moreover, Saito et al 16 showed expression of PD-L1 in cancer cells as well as immune cells in Epstein–Barr virus-associated gastric cancer (EBVaGC) were significantly correlated with diffuse histology according to Lauren’s classification. This result is different from our finding that denied any relationship between Lauren classification and positive PD-L1 TCs and emphasized statistically significant correlation of intestinal type and positive PD-L1 TILs.
It has been reported that higher PD-L1 expression in tumor cells is correlated with both favorable and unfavorable outcomes in several malignancies.11,17-19 In the study by Wang et al, 20 survival analysis revealed that PD-L1 expression was not associated with prognosis and patients with deficient MMR and HER-2 negative status exhibited higher PD-L1 expression rates. Our findings showed higher PD-L1 expression in HER-2 negative gastric cancers (P = .033). This result was controversial and some of the previous studies were compatible with ours and some has revealed opposite findings.20-22 Therefore, Anti-PD-1/PD-L1 immunotherapy might become a target of treatment for HER-2 negative patients.
The frequency of HER-2 over expression in gastric and gastro-esophageal cancer ranges from 4.4% to 53.4% with a mean of 17.9%23-26 which is higher than 4.0% from our study. Thus, future large clinical trials should be performed to clarify the relationship between PD-L1 and HER-2 expression to know whether addition of immunotherapy to anti-HER-2 therapy is beneficial for those patients with HER-2 positive gastric tumors or not.
There are reports that showed high PD-L1 expression was significantly associated with dMMR.27,28 However, in contrast to mentioned studies, we could not find any relationship between PD-L1 expression and mismatch repair deficiency. Frequency of abnormal MMR proteins function in our study was 8% that is higher than 3.7% of Molaei et al 29 reported by evaluating 134 cases with gastric cancer in Iran.
Table 8 shows brief overview of the previous reports in comparison with ours.
A comparison between our results and other studies.

Conclusion
In conclusion, our study showed that PD-L1 expression is correlated with intestinal type Lauren classification and negative HER-2 status but not with deficient mismatch repair. PD-L1 positivity in tumor cells or tumor infiltrating lymphocytes is not an independent prognostic factor in gastric cancer.
Footnotes
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support for the research from the Research Dean of Shiraz University of Medical Sciences, Project number: 18377.
Author Contributions
Fatemeh Amirmoezi: Collecting the cases, preparing the IHC slides and reviewing the slides Bita GeramizadehL Main idea of the project, reviewing the slides, writing the paper.