
Abstract
Lacrimal gland chondroid syringoma is a very rare tumor with classic clinico-radiological symptoms that should be familiar to clinicians for appropriate patients’ management as the tumor has potential for recurrence and malignant transformation. We report herein a case of chondroid syringoma in a 35-year-old patient presenting with progressive painless proptosis for 2 years. He underwent complete surgical removal of the tumor, with subsequent clinical improvement of his symptoms.
Introduction
Lacrimal gland tumors are uncommon, they represent around 12% of orbital tumors according to some reported series. 1 Histologically the most frequent lacrimal gland lesions are inflammatory, lymphoproliferative and epithelial respectively.2-4 Pleomorphic adenoma is the main epithelial tumor of the lacrimal gland.3-5 Pleomorphic adenoma is a well known benign tumor commonly found in salivary glands, however it can be found elsewhere with different names: mixed benign tumor or chondroid syringoma especially in sweat glands.6-8 Lacrimal gland chondroid syringoma (LGCS) is a very rare tumor with some characteristic clinico-radiological features that could be used for appropriate patient’s management as this neoplasm has potential for recurrence and malignant transformation.1,9,10
We report herein additional case of LGCS in a 35-year-old patient who presented with progressive proptosis.
Case Presentation
A 35-year-old male patient presented to hospital for progressive and painless right proptosis for 2 years. At clinical examination, the patient had good general condition, with right proptosis without eye movement limitation or visual disturbances. His visual acuity was 10/10. A cranio-cerebral computed tomography-scan (CT-scan) has been performed. It showed a well circumscribed retro-ocular tumor at the supero-lateral part of the orbit with no calcifications or bone destruction (Figure 1a and b). The tumor was isodense with no contrast enhancement. The patient underwent surgical resection of the tumor.
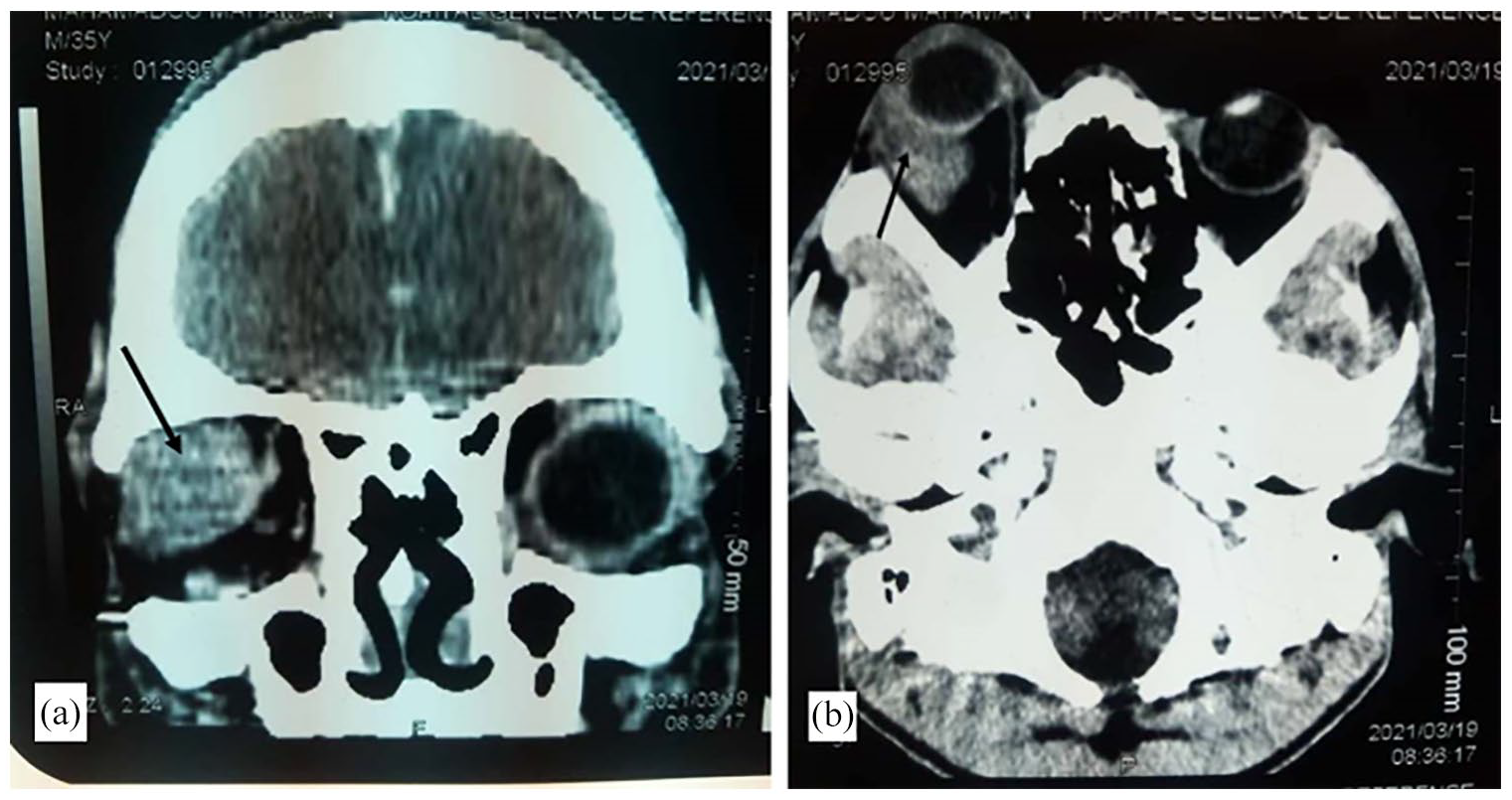
Cranio-cerebral computed tomography-scan (CT-scan), chondroid syringoma. Note a well circumscribed retro-ocular tumor at the supero-lateral part of the right orbit with no calcifications or bone destruction (arrows) ((a): coronal view, (b): antero-posterior view).
The resected nodular specimen measured 3.5 × 3.5 cm with a firm and whitish cut surface (Figure 2). The histopathological analysis showed a well circumscribed tumor with abundant fibrous and chondroid stroma (Figure 3, black arrow) associated with nests of polygonal cells and intercommunicating ductal structures lined with 2 or more rows of polygonal cells. Tubular lumens contain amorphous eosinophilic substance (Figure 3, blue circle), and keratinous cyts are occasionally seen (Figure 4, black arrow). There were no cellular atypia or mitotic figures (Figures 3 and 4). These histopathological features were consistent with lacrimal gland chondroid syringoma (LGCS).

Gross picture of specimen, chondroid syringoma. A nodular and white-tinged tumor with smooth contours.
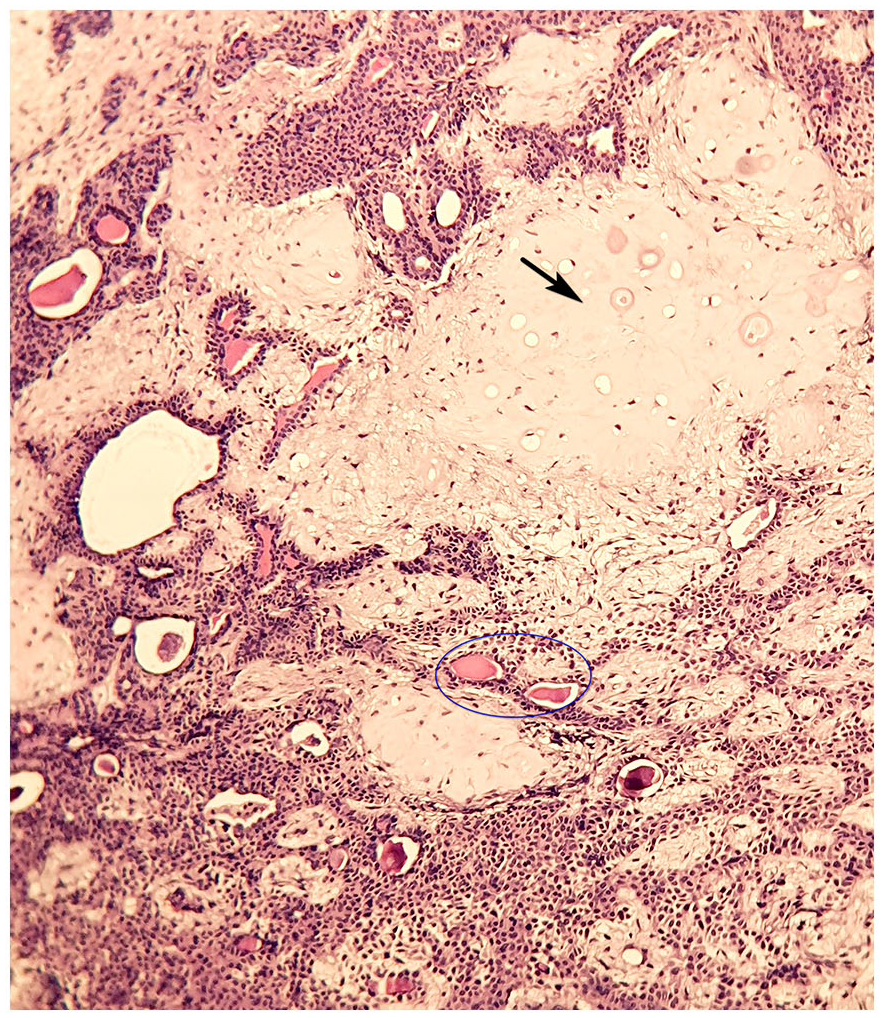
Tumor section, chondroid syringoma. Abundant fibrous and chondroid stroma (black arrow) associated with sheets and tubules of epithelial and myoepithelial bland cells. Tubular lumens contain amorphous eosinophilic substance (blue circle) (hematoxylin and eosin stain, ×100).

Tumor section, chondroid syringoma. Higher magnification shows there are no cellular atypia and mitotic figures. Keratin whorls are focally seen (black arrow) (hematoxylin and eosin stain, ×200).
The patient recovered well after surgery with correction of his proptosis and was discharged from the hospital.
Discussion
Lacrimal gland chondroid syringoma (LGCS) is a very rare tumor with quite characteristic clinical and radiological features that should be familiar to clinicians for adequate patients’ management.9,10
The tumor is usually found in adult-patients with a mean age around 38 to 47 years, and there is no gender or side predilection.1,5,9 LGCS develops mainly in the orbital lobe of the gland, and patients present with progressive painless proptosis with sometimes axial deviation.5,9,11-13 These symptoms have typically long duration, beyond 10 months.5,9 The present case had these classic clinical features with long duration of about 2 years. The painless symptoms obviously explain why patients seek clinical attention belatedly.
The radiological features of LGCS consist of a well-defined lesion in the lacrimal gland fossa, with no destruction of the surrounding tissues.9,12,14 Calcifications or bone erosions could rarely be associated. 9
These stereotypic clinico-radiological features led Rose and Wright 9 to propose a score for preoperative diagnosis of LGCS. 10 This score is mainly based on the presence or absence of some clinical and radiological signs (on high resolution CT-scan): duration of acute symptoms (less or more than 10 months), persistent pain, sensory loss, well-defined mass, tumor calcifications, bone invasion (Table 1). Patients with long clinical symptoms duration, without pain, with a well circumscribed mass without calcifications and bone destruction, have a strong preoperative suspicion of LGCS. The recommended management of these patients is surgical complete tumor removal without prior biopsy. Malignant preoperative diagnosis is suspected in patients with short symptoms duration, painful, larger and ill-defined masses with calcifications and bone destruction. Incisional preoperative biopsy should be performed in such cases. 9
Algorithm for the management of lacrimal gland masses according to Rose and Wright. 9

Total score: −8 to +2: probably carcinoma (for incisional biopsy); −6 to +2: probably malignant mixed tumor (for incisional or excisional biopsy); +3 to +8: probably pleomorphic adenoma (for excision without prior biopsy).
Incomplete resection and subsequent recurrences are predictive of malignant transformation.15-17 Preoperative biopsy is believed to cause tumor cells displacement into surrounding tissues with recurrence risk. 9 Hence the recommendation to remove the biopsy track with the tumor in patients with prior biopsies.
Although the score and recommendations of Rose and wright have a valuable clinical application, they are not always verified. In fact, many preoperative misdiagnoses of LGCS have been reported.1,18 Cases of LGCS may have misleading clinical and radiological presentations (pain, short clinical symptoms, calcifications, bone destructions). Also, some orbital lesions may mimick clinico-radiological features of LGCS, leading to unnecessary or suboptimal surgery. 18 On the other hand, the effect of preoperative biopsies on the tumor prognosis (especially recurrences) is controversial. 19 Our patient presented with classic clinical and radiological signs, and the surgical resection of the tumor was performed without prior biopsy.
Histopathological analysis is the only reliable way to achieve a correct diagnosis of LGCS. The histological diagnosis is straightforward although the site is very uncommon. It shows typically a variable admixed amount of epithelial, myoepithelial and stromal tissues.1,9 The epithelial cells are arranged in sheets and tubules associated with epithelial cells. Squamous cell metaplasia or cystic changes are not uncommon. The stromal elements show fibrous, chondroid or osseous differentiation. Cells are bland without atypia or significant mitoses. The tumor is well circumscribed by a fibrous capsule. However, focal tumor extensions into the capsule may be observed, justifying the surgical resection of the tumor with a small rim of healthy surrounding tissue. 9 Our patient has well-circumscribed LGCS with focal squamous metaplasia with fibrous and chrondroid stroma.
The outcome of LGCS is good after complete surgical resection.1,5,9 Recurrences and malignant transformation are very rare. Sivamani et al 20 have reported a case of an 84-year-old man who presented with a recurrent chondroid syringoma on the glabella that had been excised 4 years previously.
The malignant transformation of LGCS leads to carcinoma ex pleomorphic adenoma or malignant mixed tumors.15,17 A rapidly growing painful mass with orbital destruction is suggestive of malignancy. 9 The histological variants of carcinoma ex pleomorphic adenoma are mainly adenoid cystic carcinoma, mucoepidermoid carcinoma, myoepithelial carcinoma, or squamous cell carcinoma. Carcinoma ex pleomorphic adenoma shows atypia, mitoses and invasion of surrounding tissues. 10 A residual component of LGCS is often seen within the malignant tumor. 15 There are no specific molecular markers for malignant mixed tumor, although they overexpress some cellular proliferation factors like Ki-67 or c-myc along with some genetic alterations that are also found in the benign counterparts (pleomorphic adenomas).7,16
Conclusion
Lacrimal gland could rarely be a site of a common histological tumor (chondroid syringoma). This benign tumor presents usually with stereotypic clinico-radiological symptoms that should be familiar to clinicians for better patients’ management as the tumor has potential for recurrence and malignant transformation.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
BE initiated the study and wrote the manuscript, KOKA and AS performed the surgical management of the patient. All authors revised and edited the manuscript. All authors approved the final version of the manuscript.