
Abstract
Background:
Unlike some neighboring countries like Nigeria, few studies on actual causes, impact and the prevention of road traffic collisions have been carried out in Ghana. There is the need for further research and this study sought to link injuries that caused the death of drivers involved in vehicular collisions to the latent possible contributing diseases and medical conditions in these drivers and how these conditions predispose them to the collisions.
Methods:
This is a retrospective study that used the forensic autopsy records of driver fatalities and various injuries and medical conditions of drivers involved in road traffic collisions. Information on all drivers was retrieved from archives at the Komfo Anokye Teaching Hospital’ Pathology Unit. Demographics and cause of death were used in selecting the cases, including all driver-related road traffic collisions from 2009 to 2014.
Results:
A total of 1842 road traffic collisions were recorded with 127 of them being driver related. There were 31 cases (24.4%) in 2014; the highest cases recorded for this study, with the least recorded in 2009 with only 12 cases (9.4%). There were 121 (95.3%) male drivers and 6 female drivers (4.7%). Most of the male drivers were between the ages of 30 and 39 with 39 cases, while that of females was between 40 and 49 years with 6 cases. There was no significant statistical correlation between age and sex (P = .124). No statistical correlation also existed between sex and year (P = .331). Pathologies of all body systems were established. Cardiovascular diseases were the most prevalent systemic medical condition seen in the drivers with 44.1%.
Conclusion:
The study established that the drivers had various latent medical conditions and all these could lead to possible incapacitation, affecting driver judgment, leading to collisions on the road. The National Road Safety Commission (NRSC) should request medical screening before issuing driver licenses.
Keywords
Introduction
Road traffic collision is a global challenge with diverse causes and effects. It poses financial challenges to families and countries at large. 1 An estimate of $518 billion is spent annually on fatalities associated with road traffic collisions, of which about $65 billion to $100 billion is spent on middle-income countries worldwide. 2 Annually, an estimated mortality rate of 1.4 million people is recorded, while up to 50 million are injured. The World Health Organization (WHO) has projected an increase in incidence by the year 2020, although various interventions have been made to reduce its occurrence. 2 Developing countries account for 80% of the global mortality rate. Road traffic collisions and associated fatalities seem almost unavoidable in middle-income countries, especially those in Africa. A lot of studies have shown an annual increase in this disaster over the decade. Bekibele et al, 3 reported a yearly increment in road traffic collisions in Nigeria with the highest susceptibility among motorists. Studies in Zimbabwe have also confirmed this asseveration. 4
In Ghana, 2249 mortalities were recorded in 2012 while 14,169 injuries were recorded. Ghanaian men are also known to be highly involved in road collisions than females. 5 The active working force within the age range of 30 to 44 years are more susceptible to road traffic collisions, while those above 65 years are less likely to be involved in road traffic collisions. It is also known that most people at risk of road traffic collisions in Ghana are mostly pedestrians, followed by passengers, motorists, and drivers. 6
Many studies have attributed road traffic collisions to vehicular/mechanical faults, alcohol overdose by drivers, bad road systems, and human/driver errors. Few studies, however, have linked medical conditions of drivers as a possible contributory factor to these road traffic collisions.2,3,7 Medical conditions of drivers are very important, as acute onset will result in incapacitation of drivers. Diseases that are likely to cause drivers to lose control include epilepsy, ischemic heart disease, vision impairment, and hypertension.3,7 In people with epilepsy, not only can a seizure itself cause incapacitation hence a collision but also anticonvulsants often have side effects that include drowsiness. People with epilepsy are more likely to be involved in a traffic accident than people without the condition. 8 Some studies, however, have debunked this assertion. 9 In developed countries like India for example, drivers with epileptic or some cardiovascular diseases are sometimes prohibited from driving. This, however, is not the case in most developing countries.
Road traffic fatalities can be mild or severe, reliant upon the impact. The type of crash as well as the nature of the injuries sustained by the victims has an influence on the chances of survival. Studies have shown a 10:1 injury to mortality ratio globally.10,11 Head, abdominal, pelvic, extremities, spine, and thoracic injuries are among the numerous injuries suffered by drivers.12 -14
Not much has been published on the incidence of road traffic collisions in this country unlike Nigeria and Ethiopia in Africa.15,16 This study is an autopsy-based report on the injuries sustained by drivers and assesses the various medical conditions in vehicular drivers who are involved in road traffic collisions, and how these conditions could lead to possible incapacitation of drivers that led to the collisions. These medical factors were only identified via postmortem examination.
Methodology and Materials
The study was approved by the Committee on Human Research Publications and Ethics (CHRPE) of the School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology and the Komfo Anokye Teaching Hospital, Kumasi with approval no.: CHRPE/AP/349/19.
The Komfo Anokye Teaching Hospital (KATH), located in Kumasi in the Ashanti region of Ghana is the study site. The Hospital has a 1200-bed capacity and is the major referral center that serves the Ashanti region and extends to the northern part of the country. The region borders with the Eastern, Central, Western and Bono and Ahafo regions and as such the hospital is accessible to all the surrounding cities and towns.
This study is a retrospective review of various injuries and postmortem medical conditions of drivers involved in road traffic collisions. Data and all other information on the drivers involved in road traffic collisions were retrieved from the forensic autopsy archives at the Pathology Unit, KATH, Kumasi, Ghana. The Pathology Unit under the Diagnostics Directorate has a storage capacity of 500 cadavers for autopsy and preservation. The Unit receives cases from the Teaching Hospital as well as from other satellite hospitals and clinics within the Kumasi Metropolis, neighboring town and district hospitals, and in some cases, from other regions. It has 3 consultants and 5 specialists with several residents. Autopsies are performed by a specialist, who is assisted by a resident and are usually supervised by at least 1 consultant pathologist. The Unit also serves as a Teaching/Resource center for Medical students from the University as well as resident doctors.
Age, sex, and immediate cause of death were the parameters used in selecting the eligible cases. All driver-related road traffic collisions were extracted from 2009 to 2014. Those with missing or incomplete information were excluded from the study. Only drivers of motor vehicles in motion on roads/highways were considered. Drivers who died on the spot or were hospitalized for less than a month before dying from the injuries sustained were included in the study. Drivers found dead in stationary or parked vehicles were excluded.
The underlying preexisting diseases that could lead to possible incapacitation found in the drivers at autopsy were extracted from comprehensive autopsy report archives. The pathological conditions were grouped into multisystem, cardiovascular, respiratory, gastrointestinal, neurological, genitourinary, musculoskeletal, hepatobiliary, serous, and endocrine systems.
Injuries sustained were broadly grouped as; Thoracic injury, Head injury, Abdominal injury, Neck injury, Pelvic injury, Shock, and Polytrauma. Injuries of the head were further classified as Mild Head injury and Severe Head injury (include Basal skull fracture, Subdural, and Subarachnoid hemorrhages) as well as Crushed head injury. Neck injuries were also grouped as mild and severe neck injuries. Mild/Severe is in respect of degree of injury to the neck. Mild neck injury looked at contusions, abrasions, etc. (these injuries did not cause any marked deformity of the neck) compared to severe, which lead to major deformity to the vertebrae and/or spine. Cervical spine injuries with cord, and neck fracture are classified as severe.
Thoracic injuries were further classified into mild, severe as well as crushed chest injuries and vascular tube ruptures. The thoracic injuries were categorized as such with superficial injuries or thoracic fractures without displacement classified as mild and those with penetrating injuries with vital organs (lungs, heart) affection as severe. Those with complete chest collapse were taken as crushed. Liver and spleen rupture and intra-abdominal bleed were the abdominal injuries found. The data was entered into MS Excel 2016 and analyzed with Statistical Package for Social Sciences (SPSS version 21) for the descriptive statistics and correlations. Cross-tabulations with Chi-square tests were performed for age and sex as well as between systemic pathologies and site of injuries.
Results
From 2009 to 2014, 7544 death cases were recorded and 1842 road traffic collisions deaths were recorded by the unit, with 145 of them being driver deaths. Out of the 145 cases, 127 were eligible and thus selected for the study.
There were 31 cases (24.40%) in 2014; the highest proportion recorded for this study. The least was observed in 2009 with only 12 cases (9.40%). The highest incidence of 39 cases was observed between the ages of 30 to 39 years, while 60 to 69 years recorded the least of only 5 cases (3.90%). The minimum and maximum ages were 20 and 60 years respectively, having a mean age of 39.17 ± 11.68. The highest age proportion (14 cases) was between 30 and 39 years in 2014, followed by 10 cases in 2011 between the ages of 20 and 29 years (Table 1).
Year, sex and age distribution of medical factors contributing to death.

n, total.
There were 121 (95.30%) male drivers and 6 female drivers (4.70%). Most of the male drivers were between the ages of 30 and 39 while that of females was between 40 and 49 years. The latter recorded 6 cases while the former recorded 39 cases in all. Bivariate Chi-square analysis proved that there was no significant correlation between age and sex (P = .124). The annual distribution of highest number of cases of 31 cases in 2014 and 2 cases in 2010 and 2012 for male and female, respectively.
Pathologies of all systems are found except lymphoreticular. Cardiovascular diseases were the most prevalent systemic diseases followed by the respiratory system. The least incidence was recorded for both genitourinary systems and visceral organ anomalies. There were 56 cases (44.08%) of cardiovascular diseases, 20 respiratory diseases (15.75%), 18 (14.18%) of endocrine, and 1 (0.79%) genitourinary disease. The remaining systemic diseases were visceral organ anomalies, with 1 (0.79%); gastrointestinal with 2 (1.57%); hepatobiliary, 8 (6.31%); musculoskeletal, 4 (3.15); neurological system, 9 (7.08) and multi-organ diseases with 2 cases, representing 1.57% (Table 2).
Distribution of autopsy findings of preexisting medical conditions in drivers.
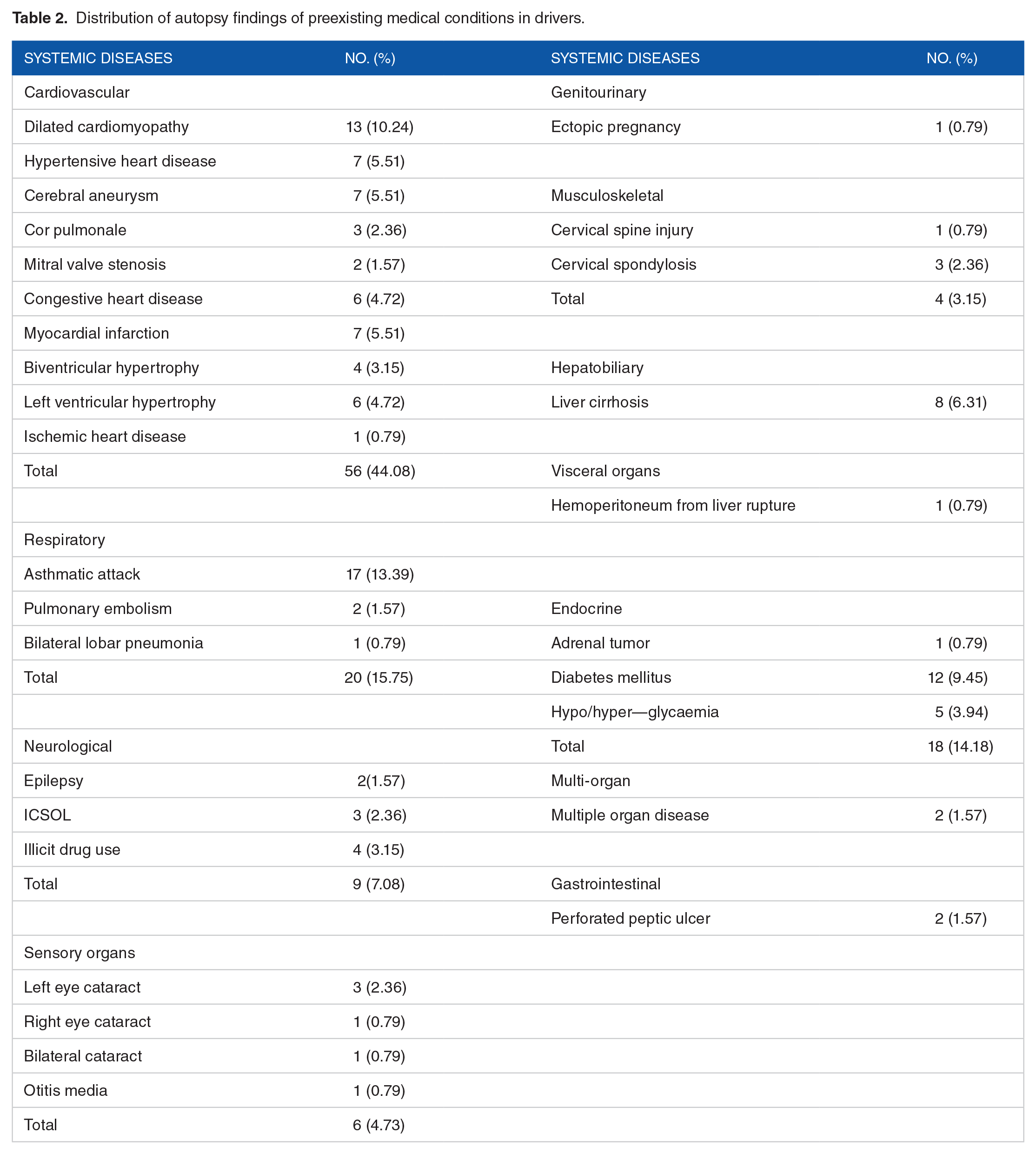
Hemoperitoneum and otitis media were the serous cavity pathologies recorded, each having 1 incidence each. Hemoperitoneum was recorded in 2011, the same for otitis media. Both were found in male drivers. There were 10 different cardiovascular diseases recorded in this study. The peak incidence was dilated cardiomyopathy (13 cases, 10.24%). The least were ischemic heart disease with 1 reported case, representing 0.79% (Table 2).
Respiratory diseases recorded in this study were asthmatic attack (17 cases, 13.39%), pulmonary embolism (2 cases, 1.57%), and bilateral lobar pneumonia (1 case, 0.79%). The gastrointestinal findings were perforated peptic ulcer (2 cases, 1.57%). Neurologic system recorded 9 cases with 2 (1.57%) epilepsy cases, illicit drug use 4(3.15%) and ICSOL 3(2.36%). Conditions of the sensory system had 6 cases of which 3 (2.36%) were reported as left eye cataract. Right eye cataract, bilateral cataract, and otitis media recorded a single case (0.79%) each. There was a case of ectopic pregnancy recorded as a genitourinary condition. Hepatobiliary findings depicted only liver cirrhosis on 8 occasions (6.31%). Endocrine pathologies constituted only 1 (0.79%) adrenal tumor cases, 12 diabetes mellitus (9.45%), and 5 hypoglycemia cases (3.94%) while multisystem pathologies included multiple organ diseases with 2 cases (1.57%).
With 74 (58.2%) of cases, head injury was by far the commonest trauma, followed by multiple organ injuries (polytrauma) with 25 cases (19.7%). With only 1 case representing 0.8% of all trauma cases, pelvic injury had the lowest occurrence. This is depicted in Table 3 below.
The distribution of injuries sustained by drivers.
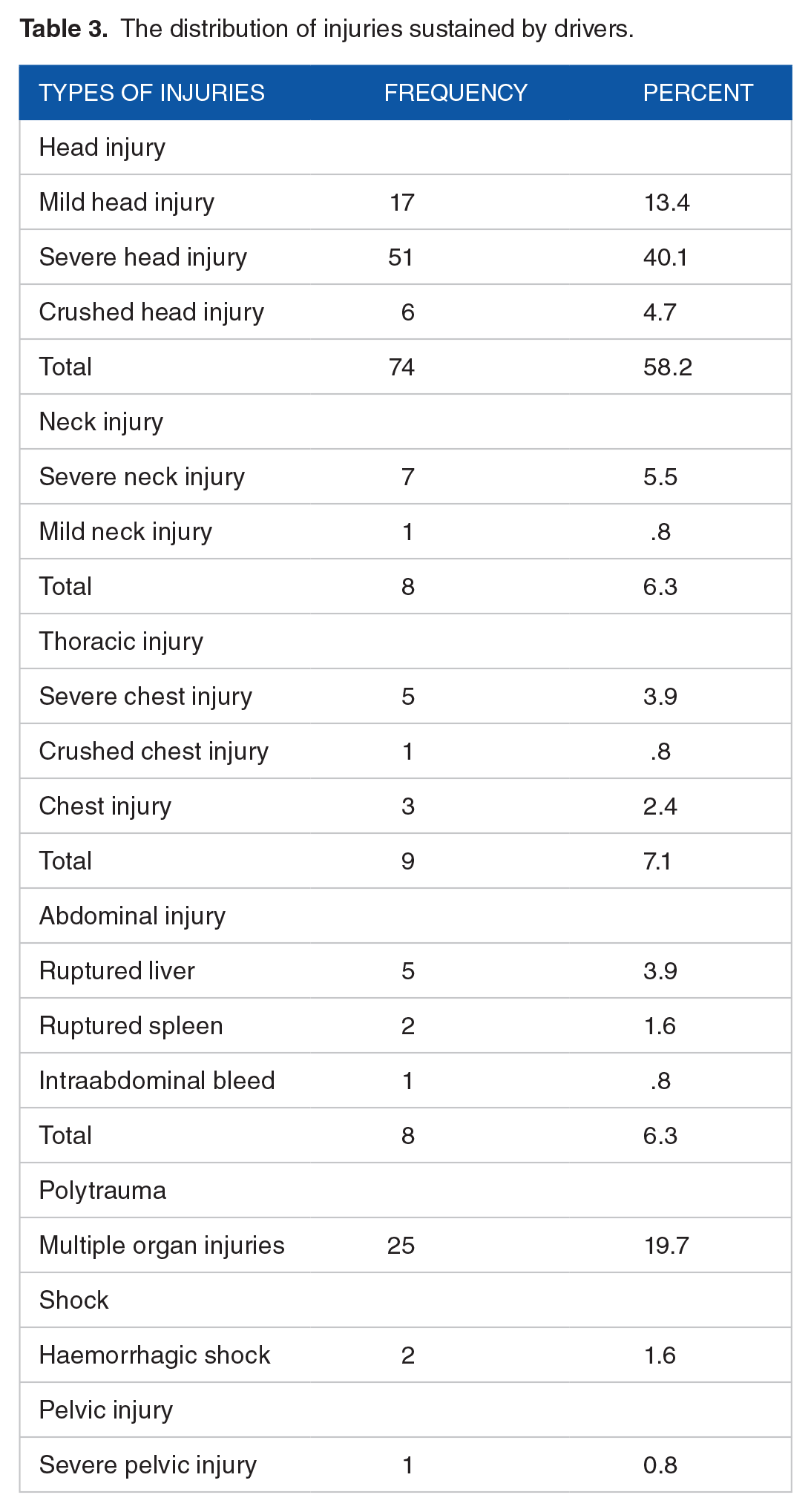
Severe head injury had the highest proportion with 40.1% (51 cases), comprising Basal skull fracture with 1 case (0.8%), 4 cases of both subdural and subarachnoid bleeding, accounting for 3.1% each. Mild head injury made up 13.4% of cases. Six (6) of the cases were crushed head injury, representing 4.7%.
The highest proportion of neck injuries was Severe (cervical spine injury with cord affection) with 5.5% whilst mild neck injury accounted for 0.8% (Table 3).
There were 9 thoracic-related injuries and 5 (3.9%) of that was severe chest injury, 3 (2.4%) were mild chest injuries, and crushed chest injury accounted for 1 (0.8%) of cases. Polytrauma accounted for 19.7% of cases and abdominal injuries had 8 cases comprising 5 liver ruptures representing 3.9%, 2 spleen ruptures (1.6%), and 1 intra-abdominal bleed (0.8%). The Table 3 below depicts these results.
Assessing the annual distribution on the various types of road traffic fatalities, there was no significant correlation (P = .08). Head injury had the highest annual incidence with 25 cases in 2014, then 2011 with 17 cases. Thoracic and neck injuries were recorded in males only.
Head injury was the most injury associated with all systemic medical conditions except endocrine. There were 74 drivers with head injuries, of which 33 had underlying cardiovascular diseases, 11 had respiratory disorders, 3 for gastrointestinal and musculoskeletal, 6 for neurological disorders, 5 for hepatobiliary, and 2 for serous cavity abnormality. One head injury was reported for multisystemic pathology and genitourinary diseases (Table 4). Severe head injuries were dominant and mostly associated with dilated cardiomyopathy. Polytrauma was associated with 11 cardiovascular, 6 respiratory, 3 hepatobiliary, 2 musculoskeletal, and 1 each for neurological, endocrine, and multisystem pathologies.
Systemic pathologies and site of injury distribution.

Chi Square value = 0.995—statistically insignificant.
Cardiovascular diseases had the highest incidence (56 cases) among the various injuries recorded. This was followed by respiratory (20 cases) and endocrine systems (18 cases). Musculoskeletal and neurologic diseases had 4 and 7 cases, respectively. Seven out of the eight neck injuries were cervical spine injuries with cord involvement, of which 4 of them were associated with drivers with cardiovascular disease. Severe chest injuries were identified among 5 drivers, 3 had underlying cardiovascular diseases, and 1 each with respiratory and musculoskeletal anomalies. Ruptured liver was the predominant abdominal injury incident among the 5 drivers. Four of these drivers also had cardiovascular disease while the remaining was musculoskeletal linked. Most drivers with polytrauma and head injuries were found to be involved with asthmatic attack among respiratory diseases. Two drivers with head injuries were reported to consume alcohol in excess, while only 1 with thoracic injury had alcohol overdose. Left cataract was found in 3 drivers who sustained head injury. The level of associations were generally not significant (P = .995).
Discussion
Driver-related road traffic collisions and associated fatalities accounted for 7.8% of all road traffic mortalities recorded within the study period. This shows a high incidence compared to 0.63% that of Moafian et al 17 in Iran. This also differs slightly from the 10% reported by Jha et al 13 and the 6.5% reported by Seid et al. 18 The 95.3% mortality recorded for males agrees with what Moafian et al 17 reported.
An estimated 65% rise in fatalities on the road in this part of the world seems possible as findings from the study revealed increased incidence over the years with only a little lows in years 2012 and 2013 with more than 100% increase in driver-related road traffic collisions and associated mortality from 2009 compared to that of 2014. 17
There was a high proportion of male driver mortality compared to females with 13:1 male to female ratio. Contrary to the findings of Bener, 10 which had a peak age-range incidence of 10 to 25 years, most drivers in this study were between 30 and 39 years with mean age 39.17 ± 11.68. This was marginally trailed by the age group 40 to 49 years. Siaw et al 6 recorded a peak age range of 35 to 44 years. They explained that most of the active working forces that could afford to drive were within this age range, hence are more probable to be engaged in road traffic collisions. The lowest age group proportion was recorded by the 60 to 69 years, making up 3.9% of all injuries and is consistent with that reported by Jha et al, 13 and attributes the less mobility by drivers of 60 plus years as the reason for the low prevalence. Most of the collisions and associated fatalities incidence occurred in 2014 with 24.4% cases. This confirms the projected increase in road traffic accidents in Ghana by Coleman. 2 Atubi 16 also reported on a possible rise in incidence of road traffic collisions among drivers. All these studies made such assumptions based on the rising population sizes and the projected increase in the number of automobiles on our roads.
A lot of efforts have been made through research to identify the major cause(s) of road traffic collisions. Driver-related cause of road traffic collisions in Ghana according to Coleman 2 was mostly attributed to illiteracy, drug or alcohol overdose, overloading, over speeding, unqualified drivers and design of road signs. Little is known on pre-existing medical conditions of drivers who died via injuries sustained in road traffic collisions. Norman 7 in his WHO report, asserted the possibility of medical factors inherent in drivers as a cause of road traffic collisions. Medical factors are classified into cardiovascular, respiratory, gastrointestinal, abdominal, neurological system, and hepatobiliary system pathologies. Other factors include multiple organ diseases and shock.
Cardiovascular diseases accounted for the majority of all medical conditions detected among the drivers (44.1%). This is in agreement with the WHO’s report on Ghana in 2015 with cardiovascular diseases being the majority contributor to mortality in Ghana, of all non-communicable diseases (14.5%) compared to the 13.4% for malaria,19,20 with most of the drivers with cardiovascular conditions in this study having dilated cardiomyopathy (10.3%) among other cardiovascular disorders. Norman 7 asseverated a greater likelihood of drivers suffering from ischemic heart disease or myocardial infarction (leading to collisions) than dilated cardiomyopathy or any other cardiovascular diseases. He further affirmed conditions such as hypertension as a contributory factor to road traffic collisions. Drivers with any of these cardiovascular diseases are predisposed to sudden unconsciousness or “black out,” resulting in loss of control and eventually leading to collisions. Most drivers were aware of these pathologies but conceal or failed to seek medical attention. 7
Respiratory diseases accounted for 15.7% deaths among drivers. Majority of these diseases were asthmatic attacks. Drivers with respiratory diseases like asthmatic attacks, pneumonia and pulmonary embolism like recorded in the current study were at risk of experiencing breathing difficulties. Asthmatic attack onset can be triggered by allergies such as smoke, pungent smell, and dust, which is common on many roads in Ghana. These put drivers in these conditions at a higher risk of losing control, eventually leading to collisions. Air pollutants such as fumes from vehicles and factories, ozone, and dust can trigger and exacerbate these conditions and therefore impair breathing. 21 Charlton et al 22 discussed some respiratory disorders that can also lead to road traffic collisions; these include emphysema and chronic bronchitis.
Perforated peptic ulcer was the only gastrointestinal pathology recorded while that of genitourinary origin is ectopic pregnancy. No study has documented the effect of perforated peptic ulcer and ectopic pregnancy as a major medical condition contributing to road traffic collisions and accompanying fatalities.
Majority of drivers with neurological pathologies were due to illicit drug use. A lot of studies on road traffic collisions have vividly proven substance overdose as a cause of these collisions, most especially alcohol. Bekibele et al, 3 reported 50.5% alcohol use by drivers . He further asseverated that central nervous stimulants such as kolanut and cigarette are some substances abused by drivers. Norman’s report proposed hypnotics, sedatives, and tranquilizers are possibly abused drugs by most drivers. Although much is not known of epilepsy being a cause of road traffic collisions, Norman 7 made an assertion that epileptic drivers are susceptible to seizures or “black out” which will lead to complete loss of control, with the current study reporting a driver with epilepsy. Intracranial space occupying lesion (ICSOL) can induce severe headache among drivers with such condition. This can result in loss of control or visual impairment due to its neurological and usually sudden effects. 22
All drivers involved in this study sustained post-crash injuries. However, some pre-existing muscoskeletal pathologies encountered were cervical spine injuries and cervical spondylosis. These conditions are triggered by some neurological disorders that can result in the onset of severe headache or back pain. In some cases, this can lead to vomiting and visual loss, and to a larger extent, seizures. Arthritis, limb amputation, and hip fracture are some musculoskeletal conditions that can predispose drivers to road traffic collisions. 22
Liver cirrhosis was the only hepatobiliary pathology encountered in this study, accounting for 6.3% of all cases. Drivers with liver cirrhosis at its peak onset will become tired and weak. This is followed by confusion and possibly unconsciousness leading to collisions. 23 This is a possibility in a country where most drivers embark on journeys on empty stomachs to avoid natural inconveniences such as stomach upsets on the way due to the lack of rest stops on our roads.
Adrenal tumor was found in 1 driver. Little is being known of this as a contributory factor to road traffic collisions. However, adrenal tumor is a serious medical condition that can lead to hypertension, heart palpitations, severe headache, diabetes, abdominal pains, and nervousness. Peak onset of any of these diseases will lead to a total loss of control. 24 Norman 7 reported diabetes mellitus and hypoglycemia as major conditions that make drivers more probable to road traffic collisions, as the sudden onset of complications of the 2 can lead to total collapse resulting from cardiac-related pathologies. Some studies have confirmed diabetic drivers are at higher risk. 25 Other medical factors identified in this study were ectopic pregnancy and multiple organ damage. Studies are yet to prove the effect of ectopic pregnancy as an immediate cause of road traffic collisions. 26
Sensory organ diseases are very vital, especially among drivers. Left, right, and bilateral eye cataract is a major anomaly that needs to be checked among drivers. Eye cataract is a contributory factor to visual impairment; hence drivers with this condition are more likely to have visual difficulty, especially at night that leads to poor judgment by such drivers. Many studies have proven visual acuity/impairment as a cause of collisions on the road.27,28
The nature of fatality depends on the type of collision.14,18 Head injuries accounted for the majority of fatalities recorded with 58.27%. This is consistent with the findings of Kual et al 14 and Seid et al. 18 Majority of the head injuries were severe (33.1%) compared to mild (13.4%). Again from the study, 6 (4.7%) drivers had crushed head injuries and 1 driver (0.8%) suffered basal skull fracture. This trend is in stark contrast with the incidences of severe, moderate, and mild head injuries reported by Seid et al. 18 Subdural and subarachnoid hemorrhage was recorded in 4 drivers each (3.1%). Higher incidences of subdural and subarachnoid bleed among drivers has been reported in many studies.14,18 The high incidence of head injuries demands the enforcement of the use of seatbelts by vehicle users, especially those at the wheel.
Neck and head injuries recorded by the study were 64.6% and sharply contrasts the 19.86% reported by Kual et al. 14 The high percentage recorded from this study is attributed to the indiscipline demonstrated by many drivers, who despite the bad nature of our roads and other factors like the proliferation of unstandardized and unapproved road rumps, do not adhere to the wearing of seat belts and do so mostly to impress road taskforce.
Thoracic injuries are widespread in most road traffic collision studies. They made up 7.09% of injuries recorded in the study with severe chest injury, mild chest injury and crushed chest injuries making up 3.9%, 2.4%, and 0.8%, respectively. Similar outcomes have been described in several other studies.14,18 This can be attributed to the same reason as cited in the previous paragraph with a general lack of adherence to the wearing of seatbelts.
Eight drivers (6.3%) suffered various abdominal injuries. This finding is similar to that by Seid et al 18 in Ethiopia and considerably lower than what Kual et al 14 reported. The abdominal injuries recorded include liver and spleen rupture, with 3.1% and 1.6% respectively. Kual et al 14 recorded 19.81% and 11.34% liver and spleen rupture respectively, a finding that slightly contrasts our study.
In most findings from other research, pelvic injuries are rare, and makes up 0.79% of all injuries reported from this study. Two drivers (1.57%) registered haemorrhagic shock, while 25 (19.69%) of them suffered polytrauma. This is consistent with what Kual et al 14 reported but considerably lower compared to the 93.5% polytrauma reported by Eke et al. 29
Correlations between medical conditions and road traffic collisions remain a paradox. Although some studies have proven it to be a cause of road traffic collisions, others have exempted it from the commonly known causes of road traffic collisions and accompanying fatalities. Mishra et al 30 proved the affiliation of medical conditions such as diabetes and epilepsy to road traffic collisions. However, the majority of studies on the causes of road traffic collisions have excluded medical factors. 31
In this study, the predominant association between the medical condition and the type of injuries sustained by drivers was cardiovascular pathology and head injury. Only a few studies have so far attempted to correlate medical factors with the type of injury they can lead to. Likewise, the findings of this study showed no statistical significance between the medical factors and type of injury (P > .05). Further studies on the subject may reveal significant associations between the 2 factors with higher sample sizes. Based on the findings from the current study, it can only be asserted that medical factors may have a role to play in drivers involved in road traffic collisions.
Conclusion
Medical conditions may not directly influence the type of injuries sustained by drivers involved in road traffic collisions. However, acute or chronic diseases put vehicle drivers at a greater risk as it onset can lead to unconsciousness and impaired judgment, hence incapacitation that results in road traffic collisions. Drivers with inherent medical conditions are predisposed to losing control at any time, thereby putting them at risk of getting involved in road traffic collisions. Just as much emphasis is being placed on the mechanical factors of vehicles and intake of alcohol or drugs by most drivers as major contributory factors to road collisions and accompanying fatalities worldwide, the health of drivers must also be of global concern. Increasing mortality among drivers in Ghana is evident. Head injury and polytrauma accounted for most of these deaths. Most of the injuries were preventable by the adherence to the use of seatbelts and serves as a warning to the National Road Safety Commission to enforce strict adherence to road laws. Although it could not be ascertained that the medical conditions had a direct effect on the collisions recorded in the study, the demand for the medical state of drivers seeking licenses cannot be overlooked. Could the medical condition of drivers be a contributory factor to the rampant road traffic collisions and its associated mortality in this country? This requires further in-depth research with larger sample sizes that may reveal significant associations.
Footnotes
Acknowledgements
The authors appreciate the contributions of Mr. Dick of the Pathology Unit of Komfo Anokye Teaching Hospital for making data on road traffic accidents available. The authors also wish to thank the Ghana Police for making information on these accidents victims available for the study.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.