
Abstract
Skin and Adnexal tumours are a group of benign and malignant tumours whose basic diagnosis relies on histopathology. A single tumour may show more than 1 appendageal differentiation. Morphologic distinction between benign and its malignant counterpart is of utmost importance as it affects the treatment and prognosis of patient. We have described 3 cases who presented in our university hospital, in which final resection pathological diagnosis differed from initial core biopsy interpretation. The authors have made an attempt to provide a brief overview of diagnostic overlap existing between nodular hidradenocarcinoma and tumours of clear cell histology. Salient morphologic features differentiating cylindroma or trichilemmal carcinoma from squamous cell carcinoma have also been discussed. Final diagnosis is paramount for adjuvant management and prognostication of the patient in a clinical setting.
Introduction
Adnexal tumours are a group of benign and malignant neoplasms which exhibit largely similar histologic features. They arise from hair follicles, sebaceous gland, apocrine gland and eccrine gland.1,2 These tumour may express 1 or more lines of appendageal differentiation during neoplastic transformation as they arise from multipotent stem cells present within epidermis or its appendageal structures. 3 Carcinoma are rare with incidence around 0.05% reported in western literature.4,5 Precise categorisation of these benign tumours is purely academic and generally does not affect clinical outcome. However, some of these tumours can be a feature of a syndrome, for example, multiple trichilemmomas in Cowden syndrome, sebaceous adenomas in Muir–Torre syndrome. 6
As clinical presentation is very nonspecific, definitive diagnosis can be made on histopathology only and classification is according to predominant morphological component. Small biopsy and cytology may not prove to be accurate many a times for these lesions but at least it may differentiate between benign and its malignant counterpart and thus surgical resection can be determined. We herewith present a concise report of 3 cases with either prior cytology or biopsy diagnosis of adnexal neoplasm and how their diagnosis was modified on wide excision, the impact of discrepancy between biopsy and final excision diagnosis on patient’s management and prognosis.
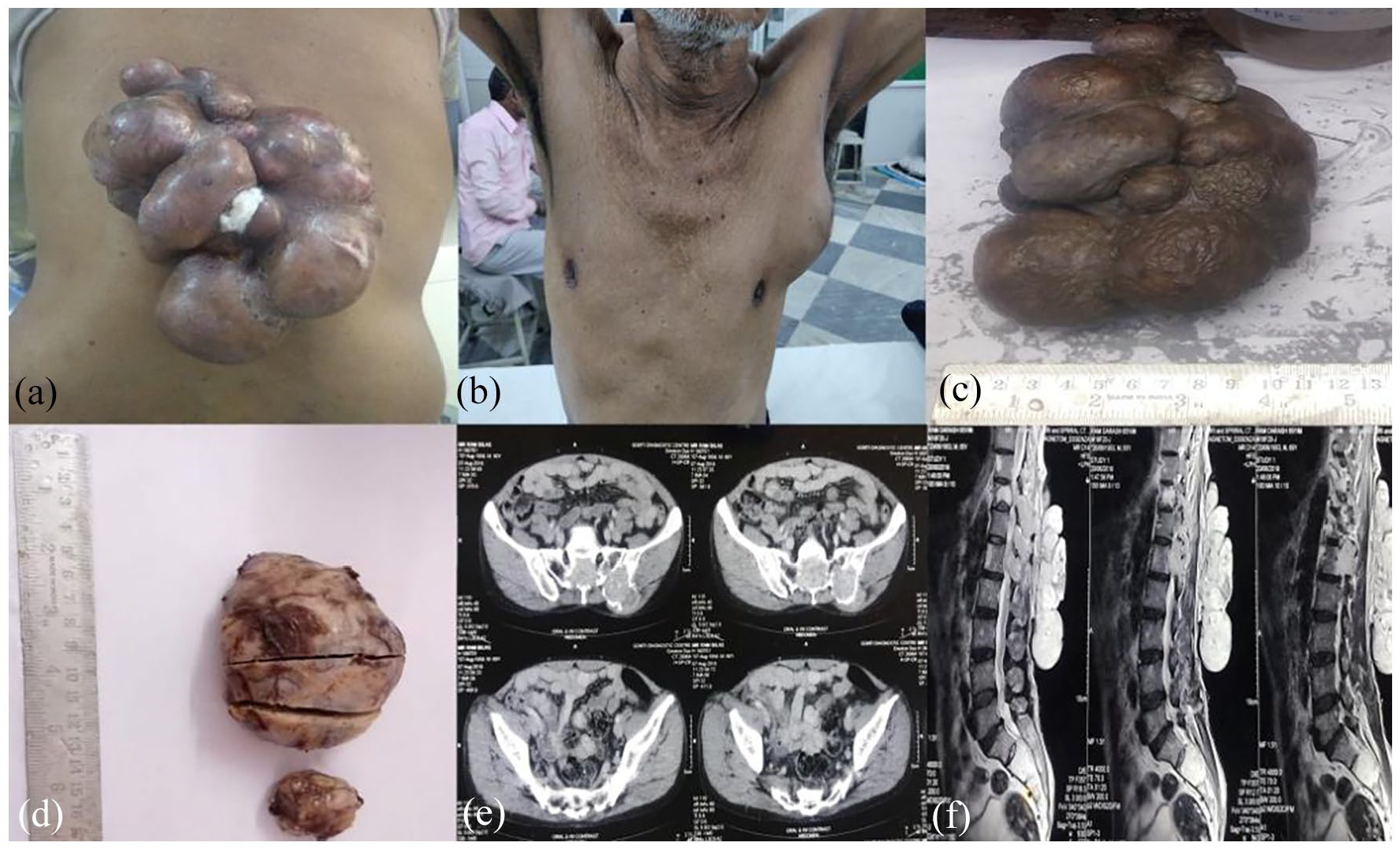
The clinical and gross images of back (a and c) and axillary (b and d) swelling show proliferative tumour. CECT and MRI images (e and f) showing bony infiltration of tumour.

Biopsy section show infiltrative tumour in (a) (H&E × 100). Cytology smear show papillaroid fragments in (b) (H&E × 200). Resection sections show intradermal tumour in (c) (H&E × 100), infiltration in (d and e) (H&E × 200) with clear cells and mucin filled spaces in (f) (H&E × 200).

Immunohistochemistery sections (×200) showing: Cytokeratin in (a) and S 100 positivity in (b). Negative staining for CEA in (c) and CD 10 in (d).

Gross picture of specimen (a). H&E section (×200) showing focal keratin pearl formation in (b). H&E sections (×100) showing positive margin (c) and perineural invasion (d). Immunohistochemistery sections (×200) showing positivity for p63 (e) and Cytokeratin (f). Negative staining is seen for CD 10 seen in (g) and BerEP4 in (h).

Scalp lesion of the patient (a). H&E section (×4) with pilar type keratinisation and area of clear cells (b). H&E section (×20) Areas of nucleomegaly, nucleolar prominence and mitosis (c). H&E section (×20) with area of pilar differentiation (d).
Discussion
Diagnosis of adnexal tumours is difficult as 1 lesion can mimic histologic features of 2 or more adenexal lesions. The diagnosis of malignancy may be evident but the recognition of adnexal origin and precise subclassification may be problematic. 7 There are a large number of defined entities but a debatable nomenclature or classification schemes from various authors seem to be conflicting till date. 8 A practical approach to the diagnosis of cutaneous adnexal tumours begins with – (a) derivation of the structure of origin (which may be difficult sometimes in view of multi-differentiation cells in the lesion), (b) evidence of malignancy and finally (c) determination of primary or secondary metastatic nature or a part of syndrome.
The correct diagnosis rendered taking above considerations has got utmost clinical and prognostic significance for a clinician and patient. Most skin adnexal tumours are benign, and therefore local complete surgical excision is curative. Morphological typing may be partially discounted still identification and differentiation of benign lesion from malignant lesion is of utmost clinical significance. A malignant counterpart of almost each of these tumours is rare, locally aggressive, and has a potential for nodal involvement and distant metastasis and thus has poor clinical outcome. The histological examination remains the gold standard in the diagnosis of skin adnexal tumours besides detailed clinical information with immuno-histochemical (IHC) studies aiding in confirmation of diagnosis. Most adnexal tumours are benign in nature. Malignant cutaneous adnexal tumour arises de novo or occurs in association with a benign component with propensity for local recurrence or distant metastases and thus overall poor outcomes. 9 Pinpointing the pathology is of paramount significance in determining the patient’s long-term survival and follow-up as 5-years overall survival for cutaneous adnexal tumours is between 70% and 80%. 10
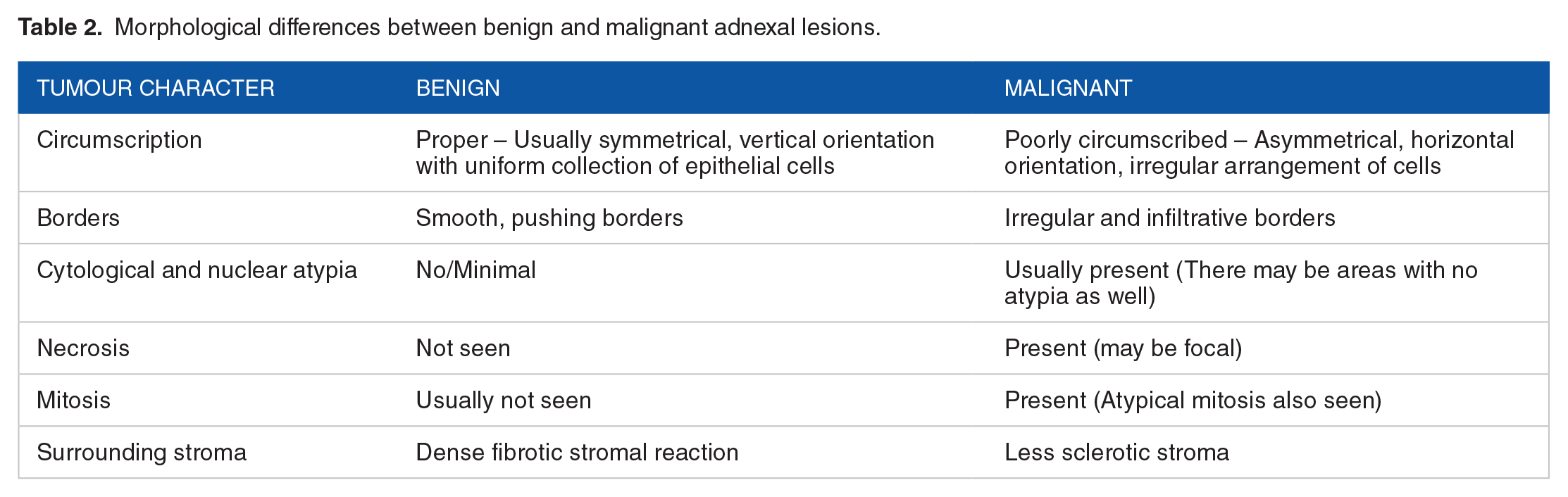
Assessment of cytological and architectural patterns is necessary in categorising cutaneous adnexal tumours. 11 Adnexal neoplasms can be categorised according to their association to overlying epidermis (Figure 6) or the prominent cell type (Table 1). The overlaps in histologic features pose an immense challenge for differentiating between benign and malignant lesions. For instance, numerous mitotic figures are often seen in benign tumours with follicular origin, such as pilomatricoma. Cytological atypia does not always entail malignancy and benign-appearing cutaneous adnexal tumours have been known to metastasise. The prominent morphological differentiating features between benign and malignant lesions are summarised in Table 2. All these histological features are relatively easily assessed in a complete excision; the challenges in the diagnosis are often related to a limited, superficial biopsy/cytology. A simplified immunohistochemical panel that may help in diagnosis of adnexal neoplasms is shown in Table 3.3,12,13 Clinical correlation is of paramount significance. A long-standing lesion that recently and suddenly increased in size may indicate a malignant transformation of an otherwise benign cutaneous adnexal tumour. Further the authors have discussed the major differentials of the pathologies of the above cases.

Relationship of adnexal tumour with epidermis.
Approach to adnexal neoplasm on basis of cell type.

Morphological differences between benign and malignant adnexal lesions.
Simplified and summarised – immunohistochemical approach to broad categories of adnexal neoplasms.

Abbreviations: AA, apocrine adenoma; AC, apocrine carcinoma; CS, chondroid syringoma; CYLIN, cylindroma; HAC, hidradenocarcinoma; PC, porocarcinoma; PEA, papillary eccrine adenoma; SP, syringocystadenoma papilleferum.
Hidradenocarcinoma (HAC) versus other tumours with clear cell histology
Hidradenocarcinoma (HAC), a malignant intradermal sweat gland tumour usually presents in fifth to seventh decade of life with no sexual and racial preferences. 14 The first case of hidradenocarcinoma was reported in 1954 by Keasbey and Hadley. 15 This tumour represents malignant equivalent of hidradenoma and amounts 6% of malignant eccrine tumour.4,5 Occasionally occurring in trunk, this tumour has a predilection for face and extremities.5,16 With pathogenesis still unknown, literature states that HAC has both eccrine and apocrine variants.16,17 Hall et al 18 has proposed that HAC arises only from ductal part of eccrine sweat glands only to contradict his own theory later. Clinically it presents as solitary asymptomatic, slow growing nodular skin lesion measuring approximately 1 to 5 cm.4,16 Metastasis is usually to regional lymph nodes, lung and bones5,19,20 On gross pathology, HACs are well-circumscribed nodules on the superficial skin. Morphologically, definitive histologic features that distinguish HAC from the benign counterpart or other related malignant tumours are lacking. Broad differentials may include adenoid cystic eccrine carcinomas, aggressive digital papillary adenocarcinomas, eccrine adenocarcinomas, and mucinous eccrine carcinomas. Primary eecrine tumours presenting similar features of benign adenexal tumours pose a great challenge to differ from HAC and metastatic visceral adenocarcinomas. 21 The morphological features supporting HAC are – no connection to overlying epidermis, nodular pattern, presence of 2 cell types and degenerating cells forming cyst like structures which were all seen in first case resection sections. However these features were not pronounced in biopsy as seen in Figure 1e though features of malignancy were seen. Immunohistochemical marker which may be of help from differentiating HAC from its eccrine counterparts is androgen receptor (AR) as seen in Table 3, rest others have overlapping results.
In summary, a lesion may be classified as malignant HAC if 3 or more of the following features are met viz. loss of circumscription, infiltrative growth pattern, deep extension, necrosis, perineural and lymphovascular invasion, nuclear pleomorphism and 4 or more mitoses per 10 high power fields. 22 Loss of circumscription, infiltrative growth pattern and necrosis were seen in our case with variable IHC expression – diffuse strong expression of CK, EMA and S-100 with no expression for CEA and CD10 (to rule out metastatic renal cell carcinoma). Genetically t(11; 19) translocation due to fusion of MECT1 and MAML2 gene and wild type TP53 mutation has been mentioned in anecdotal reports. 23
Cylindromas versus SCC
Benign tumour arising from eccrine gland is known as cylindroma. It has rare incidence of malignant transformation which may be clinically seen as recent increase in growth size, ulceration or reddish discoloration of tumour nodules. 24 Histomorphologically it is characterised by sheets of high grade undifferentiated tumour cells with abundant eosinophilic cytoplasm. Tumour necrosis and mitosis may also be seen. Morphologic features which are overlapping with SCC or its variants may be present in malignant cylindromas. 25 Though various published reports stress on the presence of benign adnexal tumour component to consider for malignant transformation; it may not be seen in a long-standing tumour. Immunohistochemically CEA may be useful in some scenarios as it is consistently seen in cylindromas but has variable to no expression in SCC (Table 3).
Increased risk of recurrence along with tumour metastasis and death is usually seen in cylindromas in cases where the following morphological features are evident. These include tumour location (ear, lip, anogenital, scars), size (>2 cm in diameter), depth of invasion (>4 mm or beyond subcutaneous fat), perineural invasion, poorly differentiated morphology, infiltrative or desmoplastic growth pattern and history of local recurrence. 26
Trichilemmoma (TA)/Trichilemmal carcinoma (TC) versus SCC with clear cell features
TA and its rare malignant counterparts are derived from the follicular outer sheath and have characteristic clear cytoplasm due to increased glycogen content and occasional presence of trichohylaine granules.8,27,28 It usually occurs on the sun-exposed areas of older individuals or may be a part of syndrome viz. Cowden’s syndrome. 29 The lesion is usually solitary and may present as an exophytic or polypoid nodule that may be hyperkeratotic with ulceration. TC was first described in 1976 as ‘a histologically invasive, cytologically atypical, clear cell neoplasm of adnexal keratinocytes which is in continuity with the epidermis and/or follicular epithelium’. 30 Histopathologically, TC demonstrates a lobular proliferation centred on pilosebaceous structures composed of clear cells with prominent nucleoli. Focal necrosis, haemorrhage or areas of squamous differentiation may also be present. The histological distinction between TC and SCC with clear features is challenging but also holds importance with the fact that chances of metastasis in TC are very low unlike SCC. Defined as the abrupt transition of nucleated squamous epithelial cells to enucleate keratinisation without the formation of a granular layer, it is a consistent feature of TC along with the presence (at least focally) of pagetoid interface, dermal invasion, trichohyalin granules and areas of peripheral nuclear palisading (Figure 5b and d). Moreover, in cases of SCC with clear cell features, an in-situ component is usually present which was not seen in our case. Clear cells of TC were stained positive with PAS as they contain glycogen but areas of trichohyalin granules are PAD positive. Both express CK5/6; however, there are reports that CD34, CK14 and CK17 are specific for TC and p63 and p40 are explicit for SCC (Table 3).
Conclusion
We present a simplified approach to the morphological diagnosis of adnexal neoplasms with summarised IHC. During a pathological evaluation of specimens for skin adnexal tumours, the pathologist should be provided with sufficient clinical data that may prove to be useful in achieving accurate diagnosis considering the fact that they show heterogeneous differentiation from the common folliculo-sebaceous apocrine unit. The gross examination should be done meticulously and status of the surgical resection margins should be recorded. The specimen should be thoroughly sampled. Sections from tumour and uninvolved areas are important to evaluate the growth pattern of the tumour. Small or superficial biopsy should be best avoided and complete specimen should be examined in entirety. Careful morphological observation with clinical co-relation still stands to be pivotal in diagnosis and classification of adnexal lesions.
Footnotes
Acknowledgements
We are thankful to King George’s Medical University for providing the infrastructure to perform our work. We are also thankful to our Immunohistochemistry and histopathology laboratory staff for their support.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization: Preeti Agarwal, Apoorva Agarwal.
Methodology: Preeti Agarwal, Apoorva Agarwal, Akshay Anand.
Software: Apoorva Agarwal, Preeti Agarwal.
Validation: Preeti Agarwal, Apoorva Agarwal, Akshay Anand, Manish Agarwal.
Formal analysis: Apoorva Agarwal, Preeti Agarwal.
Investigation: Apoorva Agarwal, Preeti Agarwal, Mala Sagar, Shalini Bhalla.
Resources: Madhu Mati Goel, Arun Abhinav Sonkar.
Data Curation: Apoorva Agarwal, Preeti Agarwal.
Writing - Original Draft: Apoorva Agarwal, Preeti Agarwal, Akshay Anand.
Writing - Review & Editing: Preeti Agarwal, Shalini Bhalla, Madhu Mati Goel.
Visualisation: Apoorva Agarwal, Preeti Agarwal.
Supervision: Madhu Mati Goel, Arun Abhinav Sonkar.
Project administration: Preeti Agarwal.