
Abstract
Background:
Solitary fibrous tumor (SFT) is a fibroblastic tumor that has been originally reported as a pleural tumor but now has been defined as a tumor that can be seen everywhere in the human body. Histopathologically, many of the fibroblastic tumors can mimic SFT, and immunohistochemistry is necessary for differential diagnosis. Several markers have been used, and recently, STAT6 has been introduced as a diagnostic marker. No research study has been reported from Iran.
Objectives:
In this report, we are trying to introduce our experience about the clinicopathologic findings of 35 cases of SFT during the last 10 years from our center with an emphasis on the diagnostic role of STAT6 in this tumor.
Patients and methods:
During the last 10 years, we confirmed the diagnosis of 35 cases of SFT in the pathology archives of Shiraz University of Medical Sciences. These 35 cases were considered as cases. All the clinicopathologic findings were also extracted from the clinical charts of the patients. To evaluate the diagnostic role of STAT6, another 35 cases of spindle cell tumors were also extracted from the pathology archives as mimickers of SFT. STAT6 was stained in all of the 70 cases and controls.
Results and discussion:
Our experience showed that SFT is more common in middle-aged men with a wide age range, although it is very rare in children. It can be present in every location with a wide size range from less than 1 cm to more than 15 cm. The presence of abnormal staghorn vessels is one of the main diagnostic histopathologic characteristics. STAT6 showed a sensitivity and specificity of 91% and 86% in the diagnosis of SFT. Other markers such as CD99, CD34, and BCL2 have also been considered useful in the differential diagnosis of this tumor, although the diagnostic accuracy seems to be lower than STAT6. High mitosis, presence of necrosis, and atypia are important criteria for predicting malignant and aggressive behavior in SFT. Among 35 cases in our study, 17% showed malignant behavior as recurrent or metastatic tumors.
Conclusion:
Solitary fibrous tumor is a common soft tissue tumor that can be seen everywhere and needs careful histopathologic and immunohistochemical evaluation for the correct diagnosis and prediction of aggressive or benign behavior.
Introduction
Solitary fibrous tumor (SFT) is a spindle cell tumor which is mainly composed of fibroblastic component. The first description of SFT was in 1931 in pleura. At that time, it used to be called “hemangiopericytoma;” however, gradually it was revealed that SFT can be seen in every location of human body in addition to pleura such as deep soft tissue, subcutaneous area, retroperitoneum, abdominal cavity, and meninges. 1
This tumor has been reported mainly to occur in middle-aged adults (20-70 years of age), and it is equal in women and men. It usually presents as slow growing painless mass with large size (5-10 cm) and well-defined border. Magnetic resenonce imaging usually shows heterogenous signal intensity. 2 Grossly, SFTs are well-defined, firm, and homogeneous with or without capsule. Cut section shows homogenously white tissue. 3 Histologic sections show moderate cellularity with bland spindle to oval-shaped cells with no specific pattern. No significant atypia is seen. The intervening stroma is mostly collagenous, however, lipomatous (fatforming) differentiation may also occur. Many large branching and stag-horn thin-walled hemangiopericytic vessels are also present. This characteristic blood vessels with pericytes were what originally was defined by Stout in 1942. 4 In addition, some tumors show a predominent fat-containing component. 5 The number of mitotic figures is variable. Malignant transformation is defined as infrequent event in which a high mitotic count is noted, (>4/10 high power field [HPF]) with atypia and necrosis. 6 Rare histologic variants were aslo introduced such as mast cell rich, myxoid, 7 and giant cell rich variant. 8
Most SFTs behave indolently but sometimes they are aggressive and unpredictable, with bland cytomorphology. Contrary to sufficient local control, estimated relapse rates for malignant SFTs are about 30%.9,10
Histologic findings besides the immunohistochemical staining help to differentiate SFT and other benign spindle cell tumors such as schwannoma, fibromatosis, neurofibroma, and so on. 11
Markers such as CD99, CD34, and BCL2 are positive in SFTs and can be helpful, but recently a gene fusion NAB2-STAT6 is proposed as the molecular hallmark of SFT, encoding a chimeric protein that combines the early growth response (EGR)-binding domain of NAB2, a repressor of primary growth response (EGR) transcription factors that regulate dissociation and proliferation, with the transactivation domain of STAT6, a transcription factor that intercedes cytokine signaling.12,13 Molecular diagnostics of the fusion gene and immunohistochemical expression of nuclear STAT6 may be beneficial in diagnosing SFT, particularly in cases that are not clearly classified. 14 Subsequent studies have shown that STAT6 c-terminus nuclear immunoreactivity is a viable surrogate marker for the fusion gene and is both a sensitive and particular marker in the histopathologic diagnosis of SFTs. 14
In this report, we tried to investigate clinicopathologic characteristics of SFT in our center and evaluating the value of STAT6 as a marker for the diagnosis of SFT and differential diagnosis of SFT from its mimics.
Patients and Methods
In this cross-sectional study, we evaluated the positivity of STAT6 in 35 cases of SFT during 10 years (2009–2019) in the affiliated hospitals of Shiraz University of Medical Sciences. Another 35 cases with spindle cell morphology and diagnosis other than SFT were considered as negative controls (7 cases in each category: fibromatosis, schwannoma, neurofibroma, malignant peripheral nerve sheath tumor, dermatofibrosarcoma protuberance)
In this study, we extracted all 70 cases reported as SFT and other spindle cell tumors from the pathology archive of the affiliated hospitals of Shiraz University of Medical Sciences during 10 years. All the hematoxylin-eosin stains were extracted and reviewed by 2 pathologists (B.G. and F.S.) to confirm the diagnosis. The atypia was classified as mild, moderate, and severe according to hypercellularity, nuclear pleomorphism, and hyperchromasia. The severity of atypia was defined whether each item being mild, moderate, and severe (presence of highly atypical bizarre cells was defined as severe).
There were 35 cases of SFT in the study (23 males and 12 females) with a mean age of 50.77 ±19.65 [range: 1-99]. Other spindle cell tumors composed of 27 males and 8 female patients with the age range of 61.06 ± 16.97.
Clinical findings extracted from the clinical chart of the SFT patients including demography, treatment modalities, and outcome. The atypia was classified as mild, moderate, and severe according to hypercellularity, nuclear pleomorphism, and hyperchromasia. The severity of atypia was defined whether each item being mild, moderate, and severe (presence of highly atypical bizarre cells was defined as severe).
For all of the 35 patients, other immunohistochemical stainings were also done composed of Ki67, CD99, CD34, and BCl2. Then the best paraffin block was isolated and STAT6 performed by immunohistochemistry (IHC) for all of the 70 cases and controls.
We performed IHC on the corresponding formalin-fixed paraffin-embedded tissue block. The largest and well-fixed block of each patient was selected. Tissue slides (4 mm thick) were stained according to routine IHC procedure.
Section of tonsil served as STAT6-positive control in each immunohistochemical run. The IHC slides were evaluated by the pathologist. STAT6 was regarded as positive if nuclear staining is present.
Results
Thirty-five cases of SFT included into the statistical analysis. Twenty-two of SFTs were extrathoracic and 13 of them were intrathoracic.
Furthermore, tumor size was 8.16 ± 5.18 [range: 1-18] cm. Mild, moderate, and severe atypia were observed in 62.86% (22/35), 14.29% (5/35), and 5.71% (2/35), respectively. Also, 17.14% (6/35) of the patients did not show atypia. Necrosis was seen in 14.29% (5/35) of cases. Malignant SFT was diagnsoed if >4 mitoses/10 HPF were present, which was present in 28.57% (10/35) of our SFT cases (Figures 1–3). The mean number of mitosis in 10 HPFs was 3.47 ± 4.48 [ranged: 1-25]. It should be emphasized that mitosis should be considered as a sign of malignancy accompanied with infiltrative margins, pleomorphism, hypercellularity, and necrosis. 14

A solitary fibrous tumor of lung; (A) low power H&E view, (B) high power H&E view, (C) CD34, and (D) STAT6.

A solitary fibrous tumor of breast; (A) low power H&E view, (B) high power H&E view, (C) CD34, (D) BCL2, and (E) STAT6.

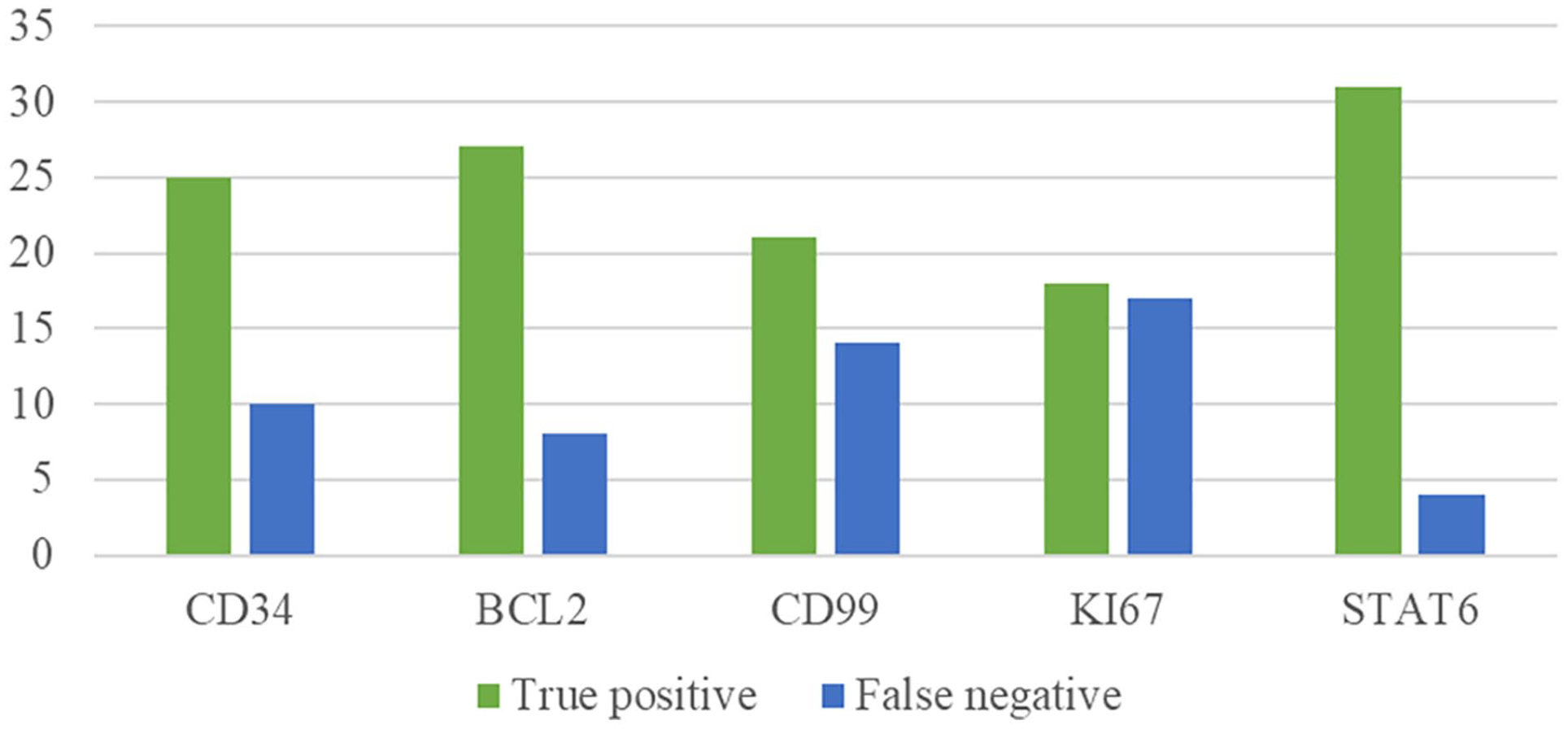
Comparing different IHC markers in diagnosing 35 definite SFT patients.
Also, all of cases, except one case, had underwent surgical resection. Four patients reported a recurrence of SFT; and 2 patients had metastasis and expired. Details of clinicopathologic findings of all 35 SFT patients are summerized in Table 1.
Clinicopathologic characteristics of the cases of SFT.
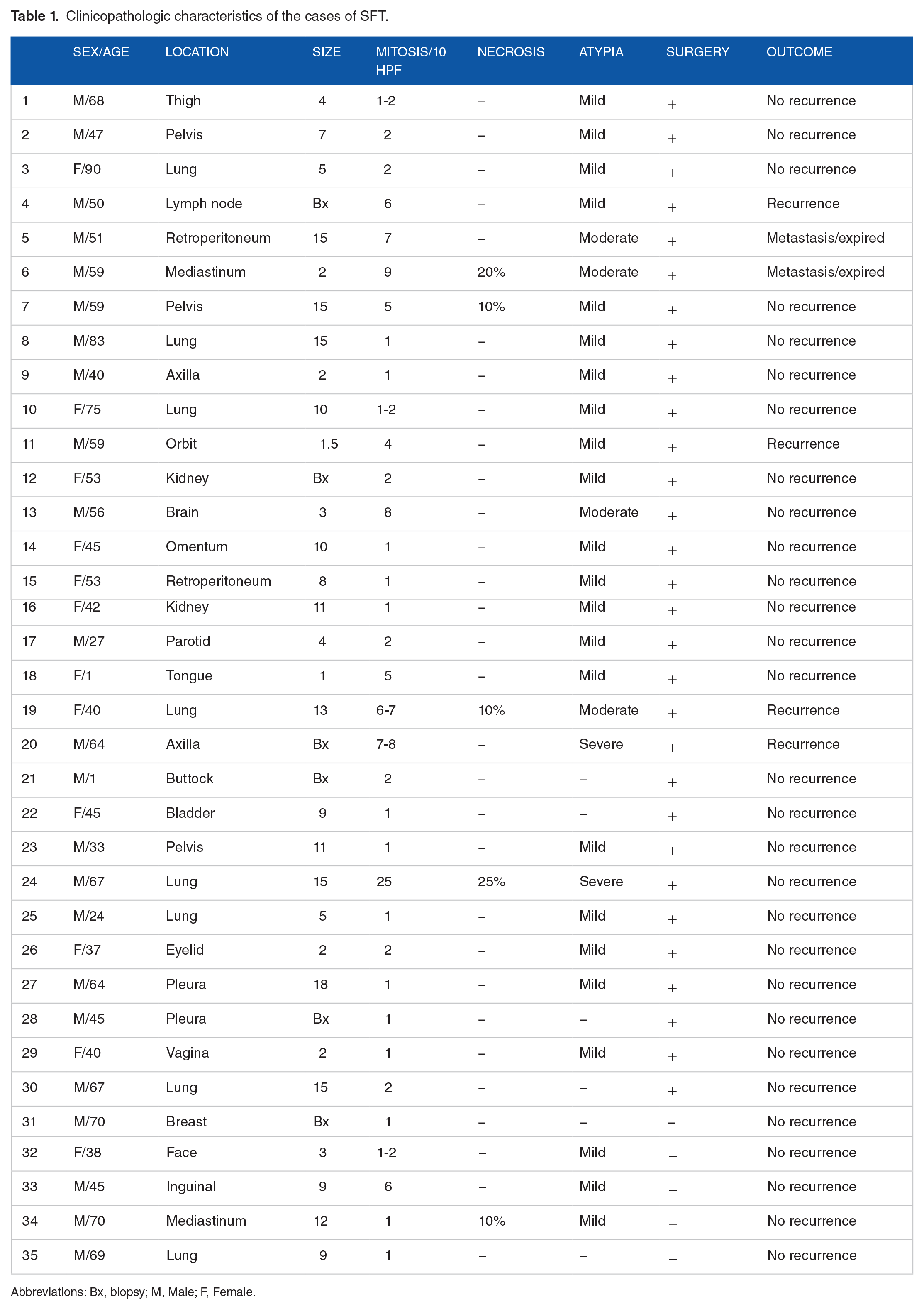
Abbreviations: Bx, biopsy; M, Male; F, Female.
Table 2 shows the value of different IHC markers in SFT, and Table 3 shows the comparison of the value of the diagnosis of SFT versus its mimickers by STAT6 and other markers. As Table 2 shows, more than 80% of the cases of SFT were positive for STAT-6, so this marker has the highest percentage of positivity in the SFT cases. The lowest percentage has been in CD99 which was positive in 60% of the cases. CD34 was the least specific marker which was positive in more than 70% of the non-SFT cases, which is shown in Table 3. Figure 4 shows the summery of diagnostic value of each marker in the diagnosis of SFT. As the figure shows, the best diagnostic value was in STAT-6. Only 3 cases with the diagnoses other than SFT were positive for STAT-6 (all 3 cases were fibromatosis). It is worthy to note that all of our cases showed intense nuclear staining.
Comparison of IHC markers with other clinicopathologic findings.
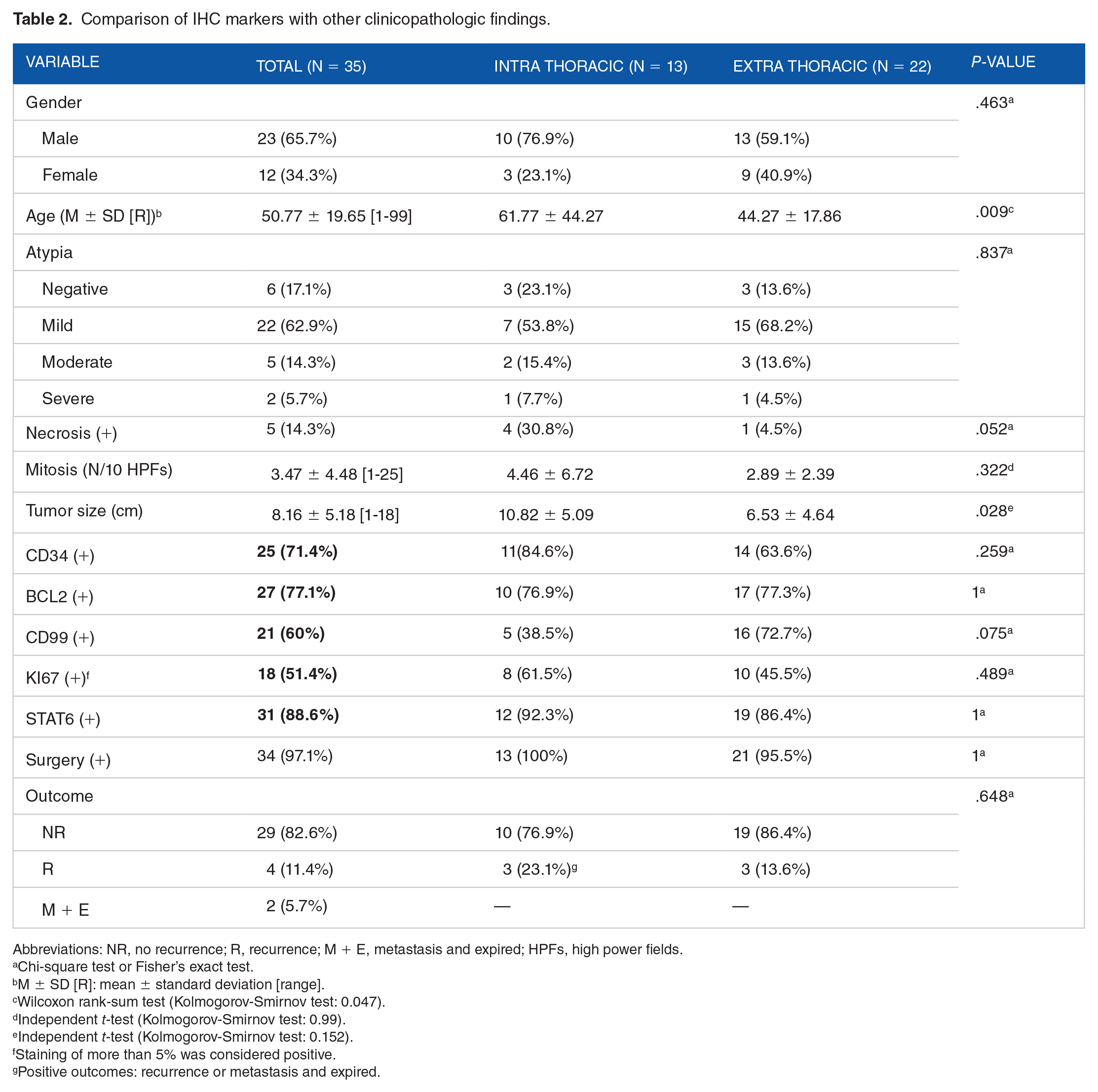
Abbreviations: NR, no recurrence; R, recurrence; M + E, metastasis and expired; HPFs, high power fields.
Chi-square test or Fisher’s exact test.
M ± SD [R]: mean ± standard deviation [range].
Wilcoxon rank-sum test (Kolmogorov-Smirnov test: 0.047).
Independent t-test (Kolmogorov-Smirnov test: 0.99).
Independent t-test (Kolmogorov-Smirnov test: 0.152).
Staining of more than 5% was considered positive.
Positive outcomes: recurrence or metastasis and expired.
Comparison of STAT6 positivity in SFT and non-SFT spindle cell mimickers.

High-power and Low-power view of malignant solitary fibrous tumor.
Discussion
Clinicopathologic findings of our study showed that SFT is more common in middle-aged men and can be seen in every location in human body. This tumor is very rare in children, and in our cross-sectional study, only 2 cases have been identified in pediatric population. The size range is variable from less than 1 cm to more than 15 cm. Histopathologically, SFT is a fibroblastic tumor with characteristic hemangiopericytic vessels which needs to be differentiated from other mimikers such as neural tumors and other fibrohistiocytic tumors. 3 In this study, we tried to investigate the value of STAT6 as an IHC marker versus other markers in the diagnosis of SFT. The main findings of our study showed that nuclear staining of STAT6 marker had the sensitivity and specificity of 88.6% and 91%, respectively. Diagnostic rate of other markers in the diagnosis of SFT were lower than STAT 6 (BCL2: 77.1%; CD34: 71.4%; CD99: 60%). This finding is compatible with previous reports. 15 NAB2-STAT6 has been proved to have pivotal role in SFT tumorigenesis, 16 and as a IHC marker, has an excellent diagnostic performance for the diagnosis of SFTs, as well as differentiating it from other mimicking pathologies.17-19 The reported sensitivity of STAT6 in the diagnosis of SFT has been from 87% to 100% in the previous reports.20-22
In our study, 17% of the cases with the final diagnosis of SFT showed recurrence and metastasis, composed of 4 recurrent tumors and 2 metastatic cases, which is higher than previous studies (10%). mitosis >4/10 HPFs, 2 showed necrosis, and 4 cases showed moderate-to-severe atypia. Also, in univariate analysis we showed that higher mitosis rate in 10 HPFs (P value < .0001) and more severe atypia (P value: .017) were correlated with worse outcome, that is, recurrence or meastasis. Other previous reports showed that up to one third of SFTs may show malignant features, atypia, and necrosis, which might be associated with malignant tumor behaviors.23-26 In the previous reports, 15% to 28.57% of cases showed malignant features. 23 Malignant SFTs should be differentiated from other sarcomas such as malignant peripheral nerve sheath tumors, synovial sarcoma, fibrosarcoma, and so on. 27
Conclusion
Solitary fibrous tumor is a tumor with wide-spread location preferences which can accurately be diagnosed by histology and IHC studies, especially the newly introduced STAT6. The overall prognosis is good, but atypia and mistosis are accurate predictor of malignant behavior.
Footnotes
Funding:
The author(s) received financial support for the research, authorship, and/or publication of this article: The project was financially supported by Research department of Shiraz University of Medical Sciences, project no:12607
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Bita Geramizadeh: Idea of research, looking at slides, analysis of data, and writing the paper.
Fatemeh Safavi: Looking at slides and analysis of data and help to write the paper.