
Abstract
Background:
Owing to limited diagnostic facilities and surveillance protocols, there is a paucity on the prevalence data of Clostridioides difficile infections (CDIs) in developing countries such as India.
Objective:
The aims of these studies are (1) to determine the prevalence of CDI in India, (2) to understand the risk factors of CDI, and (3) to determine the impact of different diagnostic methods on reported CDI rates.
Method:
A systematic literature search was conducted using PubMed and Google Scholar database to identify Indian studies reporting the prevalence of CDI. A total of 31 studies, published between 1990 and 2020 were included in the final analysis. A chi-square test was used to determine statistically significant association between prevalence rates, accuracy of different diagnosis methods, and antibiotic usage rates of CDI.
Results:
The prevalence of CDI was in the range of 3.4% to 18%, and the difference between regional prevalence of CDI was statistically significant (P < .001). The use of antibiotics, hospital stay, comorbidities, recent surgery, and the use of proton-pump inhibitors was considered as risk factors for the development of CDI. Compared to other regions, the rate of antibiotic usage was significantly higher in North India (P < .001). Among different diagnostic methods, C. difficile detection was significantly higher with enzyme-linked immunosorbent assay (18.02%) versus other multiple testing methods used (P < .001).
Conclusion:
There is a significant burden of CDI across the country. Further surveillance studies are required to monitor changes in prevalence of CDI, risk factors, and accuracy of diagnosis methods for a better understanding of the disease burden in India.
Keywords
Clostridioides difficile (C difficile) is a major cause of antibiotic-associated diarrhea (AAD) and is responsible for significant mortality and morbidity worldwide. 1 C. difficile has emerged as a predominant cause of hospital-acquired illness in the United States and developed countries. 2 C. difficile infections (CDIs) frequently occur in health care settings due to concomitant exposure to the organism and the use of antibiotics in patients with severe illnesses and concurrent conditions. The emergence of CDI in community settings in the United States is also evident from US study data. 3 Globally, C. difficile has emerged as a prominent enteric pathogen causing AAD in nosocomial and community populations. Despite being a prominent causative pathogen for AAD in the US and Europe, this enteric pathogen is highly neglected in India. 4
C. difficile is an infectious pathogen first identified in 1978 as a Gram-positive, spore-forming, anaerobic, bacillus. 5 This well-known human enteric pathogen is a frequent inhabitant in contaminated environments and the leading cause of infectious diarrhea in hospitalized patients.2,6 Antibiotic-associated diarrhea and pseudomembranous colitis (PMC) are the predominant clinical manifestations of CDI.5,7
C. difficile infections represent 15% to 25% of all cases of AAD. 8 The epidemiology of CDI has witnessed a remarkable increase since the turn of the 21st century. 7 However, developed countries like the United States has shown a declining trend of CDI burden and associated hospitalization from 2007 to 2018 due to the decrease in outbreaks associated with hypervirulent strains (eg, ribotype 027). 9 A similar trend was observed in data from the Public Health England Report that demonstrated a 76.2% decrease in CDI cases from 2007 to 2018. 10 On the contrary, the prevalence of CDI in developing countries, including India, is largely underestimated. 11
C. difficile-associated diarrhea is the hallmark symptom of clinical infections. Owing to several aspects such as poor awareness of the disease, insufficient laboratory capacity, and lack of proper surveillance systems, there is a paucity of data on CDI in developing countries. 11 Unlike resource-rich countries/continents, where substantial resources are available for the diagnosis and prevention of CDI, along with clinicians who frequently recommend testing of CDI even in patients with mild diarrhea, resource-limited countries may have diverted focus. 12 In Asia, infrequent testing of C. difficile detection is thwarted by low index of clinical suspicion and lack of rapidly accessible laboratory testing facilities, which in turn affect the exact prevalence data of CDI. 13 Widespread accessibility of antibiotics without prescription in most Asian countries and the frequent use of antibiotics as empirical therapy may result in reduced detection rate of C. difficile. 12
Inadequate capacity of microbiological laboratories could be another hindrance in attaining proper surveillance report on health care-associated infections including CDI in resource-limited countries like India. 12 In addition, the lack of routine tests for C. difficile in patients with diarrhea as well as the use of suboptimal testing methods further challenge optimal data collection. 11 Moreover, tedious and costly anaerobic techniques required for the detection of C. difficile may further contribute to the underestimated prevalence of CDI. 14
Due to the emergence of multidrug-resistant (MDR) C. difficile, it is essential to implement proper infection control policies as well as execute hospital epidemiology programs. 11 A better understanding of epidemiological patterns pertaining to CDI may help in devising better strategies for the prevention and control of CDI in a developing country like India.
Objective
This comprehensive systematic review was conducted to (1) determine the regional burden of CDI in India, (2) understand the risk factors of CDI in India, and (3) determine the impact of different diagnostic methods on reported CDI rates.
Method
This systematic literature review was conducted in accordance with the Preferred Recording Items for Systematic Reviews and Meta-Analysis (PRISMA). 15
Eligibility criteria for studies
All human studies, published from January 1, 1990 to May 30, 2020 in the English language that evaluated Indian patients of all age groups and reported the prevalence of CDI, risk factors of CDI, were eligible for inclusion. Only Indian studies were considered for the review.
Exclusion criteria for studies
Nonconsecutive case series, series with incomplete reporting of results, case reports, newsletters, editorials, and non-Indian data and publications before 1990 were excluded from the list. Review articles and other publications citing data from more than one study were excluded from the final review; however, those articles were used to identify individual studies that had not already been identified in the literature search.
Measurements
The primary outcome of this study was to determine the prevalence of CDI in India. The secondary outcome was to determine risk factors of CDI and the impact of different diagnostic methods on the reported CDI rates.
Search strategy
A systematic literature search was conducted using PubMed and Google Scholar database using search terms like “C. difficile AND India” OR “C. difficile AND Epidemiology AND India” OR “C. difficile AND Prevalence AND India” OR “C. difficile disease AND Risk factors AND India” OR “Risk factor AND C. difficile AND India” to identify relevant articles The search was performed after applying constant filters based on these additional search criteria: article types—clinical study, clinical trial, clinical trial, phase iii, clinical trial, phase iv, comparative study, controlled clinical trial, evaluation study, meta-analysis, multicenter study, observational study, pragmatic clinical trial, randomized controlled trial; language—English; publication date—January 1, 1990 to May 30, 2020; species—humans. A bibliographic search was also performed while assessing the full-text articles.
Data extraction
Data were collected from all the primary studies using a structured sheet in Microsoft Excel. Any discrepancies arising while entering the data were sorted out by discussion among all the contributors. The study characteristics extracted included authors’ details, year of publication, title of study, place of study, and type of study. Patient parameters included the number of study participants and their mean age. Two reviewers were involved in data extraction. Any disagreements among reviewers were resolved by discussion.
Statistical analysis
A chi-square test was used to determine whether there was any statistically significant association between the reported prevalence, impact of different diagnosis methods used on prevalence of CDI, and antibiotic usage rates before developing CDI. A P value <.05 was considered significant.
Literature selection
The primary literature search in PubMed and Google Scholar yielded 190 relevant articles. Eight more articles were added after a bibliographic search. After the removal of duplicate titles and abstracts, 77 full-text articles were screened for inclusion in the analysis. Following a thorough review of the full-text articles, a total of 46 studies were excluded, and the remaining 31 studies were included in the systematic review. Figure 1 represents the PRISMA flowchart of articles included in the analysis.

PRISMA flowchart of articles considered for inclusion in analysis.
Findings of the Analysis
Burden of CDI
A total of 31 articles reported data on the prevalence of CDI in different hospitals across India.16-46 Despite heterogeneity in the diagnostic approach for testing CDI between the studies, most of the studies confirmed CDI based on clinical diagnosis (“diarrhea”) and laboratory findings (“toxin positivity”). Heterogeneity exists in the study patient population in terms of age and comorbidities. Table 1 lists the studies conducted in different hospitals across India.
Burden of C. difficile in India.

Abbreviations: AAD, antibiotic-associated diarrhea; CCNA, cell culture cytotoxicity neutralization assay; CDI, Clostridioides difficile infections; CDT, C. difficile toxin; EIA, enzyme immunoassays; ELISA, enzyme-linked immunosorbent assay; HIV, human immunodeficiency virus; ICU, intensive care unit; NAAT, nucleic acid amplification test; PCR, polymerase chain reaction.
The studies included both pediatric and adult populations. Based on these studies, the prevalence of CDI in India was found to range between 3.4% and 18%. The studies predominantly highlighted cases of hospital-acquired CDI. In 3 studies, exclusively conducted among children aged 0 to 14 years, the prevalence of CDI was found to be in the range of 3.6% to 7.2%.21,45,46 The reported prevalence of CDI among 0- to 1-year-old infants was 25% 46 and 61.29% 45 of the total C. difficile toxin (CDT)-positive cases. Dutta et al 46 reported that 75% of CDT-positive children were 1 to 2 years old. Since none of the studies captured the data for age group <2 years old, it is not possible to report the colonization in this age group. Three studies involved only adult patients, and the prevalence of CDI was reported to be 3.4% in patients with ulcerative colitis and intestinal infection, 28 16% in patients with hospital-acquired diarrhea, 27 and 18.06% in HIV-seropositive subjects with diarrhea. 40 All patients with reported hospital-acquired diarrhea were under antibiotic therapy (CDT positive as well as CDT negative), 27 whereas the status of prior antibiotic therapy is poorly defined in the remaining studies in the adult population.28,40
Unadjusted statistical analysis was performed to investigate the association between prevalence of CDI and different geographical regions of the country. The difference in the regional burden of CDI was statistically significant (P < .001; unadjusted for age, sex, or diagnostic modalities).
Risk factors for CDI
A total of 22 studies reported the prior use of antibiotics in the population that developed CDI.17-20,22,24,25,27-31,34,40,42,43 Three studies have reported third-generation cephalosporin as a predominant risk factor for CDI development.26,34,42 Figure 2 highlights the studies where antibiotic usage was highest at the time of CDI diagnosis. Segar et al 22 reported a 4.7 times higher risk of developing CDI associated with the use of doxycycline among glutamate dehydrogenase (GDH)-positive patients versus GDH-negative patients.
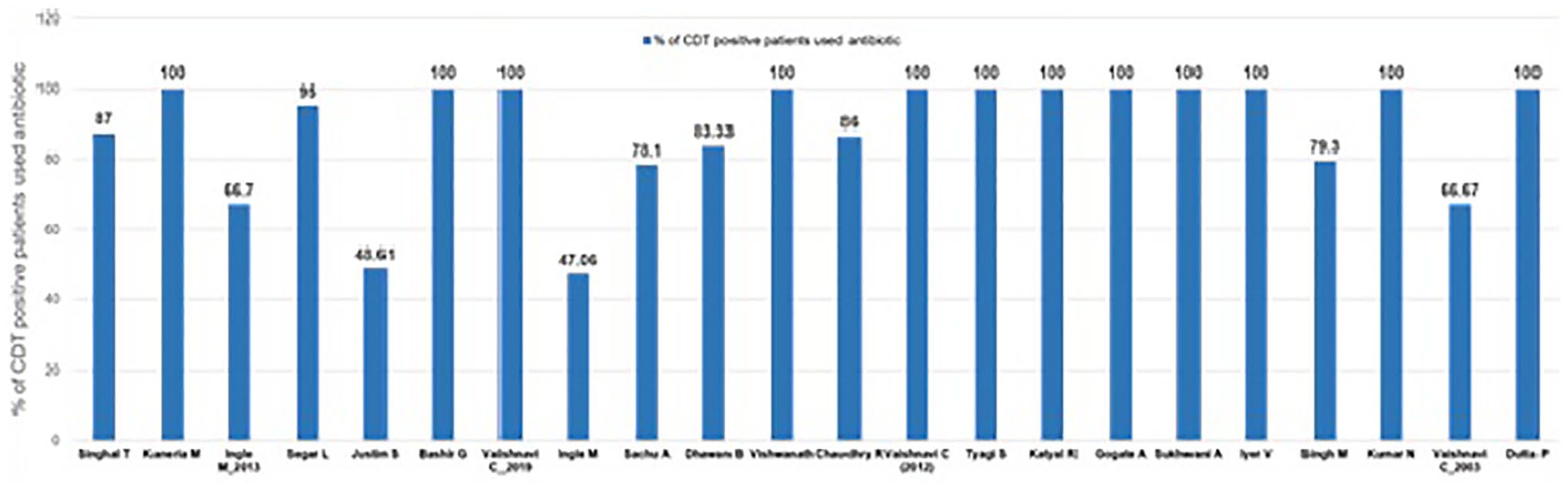
Prior antibiotic use in the CDI-positive subjects.
The majority of the studies have shown the occurrence of CDI in already hospitalized patients,16-19,21,24,26,27,29-31,33-37,39,42,46 indicating hospitalization as one of the key risk factors for developing CDI.
Advanced age is another key risk factor for the development of CDI.16,22,34,36 In the study conducted by Singhal et al, 16 39% of patients with CDI were more than 70 years old; Segar et al 22 showed that 50% of patients with CDI were between 51 and 60 years old. A majority of the studies reported a male preponderance for the development of CDI, except for one study by Justin and Antony in which females were more commonly affected by CDI than males.16,17,20,22,24,31,34,37,42 A majority of the studies reported comorbidities, especially different types of malignancies or carcinoma as a prominent risk factor for the development of CDI.24,25,29,31,33,34,42 Gastrointestinal conditions including gastrointestinal infections were reported in few studies as a potential risk factor for the development of CDI.20,29,32,44 Multiple studies have shown the use of proton-pump inhibitors (PPIs) as a potential risk factor for developing CDI.18,36,38 Apart from the above risk factors, intensive care unit (ICU) stay, use of chemotherapy, immunotherapy, and so on, were found to contribute to the development of CDI. A statistical analysis of 22 studies16-19,21,22,24-26,28-31,33-39,42,46 reported that the rate of antibiotic usage was significantly higher in North India than other regions (P < .001).
Diagnostic Methods Used in the Studies
Several diagnostic methods were used to diagnose CDI including culture tests, enzyme-linked immunosorbent assay (ELISA), positive latex agglutination test, enzyme-linked immunofluorescent assay, polymerase chain reaction (PCR), vero tissue culture, and so on. Table 2 highlights the different diagnostic methods used in the studies along with the reported prevalence of CDI in each of these studies.
Diagnostic methods used in the included studies and prevalence of CDI.

Abbreviations: CCNA, cell culture cytotoxicity neutralization assay; CDI, Clostridioides difficile infections; CDT, C. difficile toxin; EIAs, Enzyme immunoassays; ELISA, enzyme-linked immunosorbent assay; NAAT, nucleic acid amplification test; PCR, polymerase chain reaction.
The most frequently used diagnostic tests were anaerobic or toxigenic culture and ELISA (either as a single test modality or in studies that included multiple testing modalities). Among different diagnostic methods, the prevalence of CDI ranged between 3.4% to 21.6% and 4.9% to 18.06% when ELISA was used as single test18,28,33,36,41,42 and as a part of multiple testing modalities (ELISA in combination with other tests),16,21,23,24,26,29,30,34,39,41 respectively. The prevalence rate ranged between 5.9% and 16% when multiple tests were used excluding ELISA.20,25,27,31,35,41 Single test methods other than ELISA demonstrated a prevalence range between 3.6% and 25%.17,19,22,38,43-46
Discussion
Developing countries face immense challenges for optimized infection control due to limited surveillance data on CDI. 11 In India, C. difficile is a neglected, still emerging pathogen. 6 Owing to the emergence of MDR CDI, the prevention of infection through implementation of infection control and hospital epidemiology programs is an utmost need. This comprehensive literature review sheds light on this unmet need.
In this systematic literature review, the prevalence of CDI was found to be in the range of 3.4% to 18% across India. However, due to high heterogeneity related to the study design, patient population, testing strategies, and so on, it was challenging to draw a conclusive prevalence of CDI across different regions of India. It is noteworthy that the CDI rates were predominantly observed in hospitalized patients and patients who were on prior antibiotic therapy.
Several literature reviews and meta-analyses have delineated the prevalence of CDI across the globe including Asia. In a meta-analysis involving 51 studies and 37 663 patients from Asia, CDI was detected in 4343 patients. The pooled proportion of confirmed CDI among all patients with diarrhea was 14.8% with a higher prevalence in East Asia (19.5%) compared with South Asia (10.5%) or the Middle East (11.1%). 13 In a European surveillance study (conducted in multiple countries), C. difficile was identified in 4% to 39% of the collected stool samples. 47
The prevalence of CDIs in developing countries is comparatively low. A systematic review and meta-analysis conducted in developing countries including India showed a C. difficile prevalence of 15% in patients with diarrhea (including community and hospitalized patients), with no significant difference across regions. However, the same meta-analysis reported a significantly higher prevalence of CDI in hospitalized patients versus community patients (P = .02). 11 This outcome is in concordance with our analysis that demonstrates the majority of CDI cases in hospitalized patients.
The low prevalence of CDI in developing countries such as India can be attributed to poor awareness and inadequate testing. Proactive assessment of CDI in developed countries could be the underlying reason for the higher reported prevalence of CDI in developed countries. In comparison, developing countries suffer from suboptimal diagnostic facilities with limited capacity and capabilities. Thus, owing to several factors pertaining to diagnosis and management along with lack of awareness, it can be relatively hypothesized that the prevalence rate may remain underestimated in developing countries including India. 11
Uncontrolled and irrational use of antibiotics and poor hospital infection control policies have led to increased CDI occurrence in India. 4 In this systematic review, among several risk factors, antibiotic exposure, hospital stay, immunocompromised state, and, use of PPI were considered to be the risk factors for CDI. As compared to other regions, the rate of antibiotic usage was significantly higher in North India. This finding aligns with several systematic reviews and meta-analyses where exposure to antimicrobials was found to be one of the strongest risk factors for the development of hospital-acquired as well as community-acquired CDI.48-52 Antibiotic use may also result in recurrent CDI. 4 However, few studies have demonstrated the occurrence of CDI in children who were neither hospitalized nor on any broad-spectrum antibiotic treatment.53,54
Clinical history alone is inadequate for diagnosis of CDI and should be combined with other laboratory tests. The laboratory diagnosis of C. difficile is based on the isolation of the organism and the detection of its toxins and toxin-encoding genes. 55 Among several available laboratory test methods, cell culture cytotoxicity assay, toxigenic culture, real-time PCR, and enzyme immunoassays (EIAs) for GDH enzyme and toxins are frequently used for the diagnosis of CDI.56,57 Diverse testing modalities were used for the determination of the prevalence of CDI in the included studies. The most commonly performed diagnostic tests were ELISA (either as a single test or in multiple testing studies) and anaerobic or toxigenic culture. This is in concordance with a meta-analysis by Borren et al 13 where anaerobic/toxigenic culture and EIA were the most frequently used tests for the determination of CDI prevalence. In this literature review, the prevalence of CDI ranged between 3.4% and 21.6% and 4.9% and 18.06% when ELISA was used as single test and as a part of multiple testing modalities (ELISA in combination with other tests), respectively. Enzyme-linked immunosorbent assay is the most widely used laboratory test for detecting CDTs. However, there is a lack of standardization of screening methods used for CDI with a range of diagnostic tests being used to detect CDI in laboratories. 58 The Infectious Disease Society of America has recommended stool toxin test as part of a multistep algorithm (ie, GDH plus toxin; GDH plus toxin, arbitrated by nucleic acid amplification test [NAAT]; or NAAT plus toxin) rather than NAAT alone for patients at increased risk for clinically significant CDI. Owing to high heterogeneity in sensitivity and specificity level of several tests including ELISA (excluding cytotoxicity neutralization assay), the IDSA guideline places multiple testing modality over single ELISA test to ensure rapid detection, higher sensitivity along with cost-effective benefit. 59
The study limitation includes the potential for publication bias related to high variability among the studies selected. Owing to the immense heterogeneity of the articles, study design, as well as wide variation in diagnostic protocols, challenges were faced in analyzing the association of different parameters with CDI. In addition, in this comprehensive literature review, the study populations in the majority of the included studies were poorly defined, which complicated the review analysis. However, we tried to minimize the concerns through our precise adherence to the PRISMA model in selecting studies for inclusion. Further prospective studies are required to verify these results to facilitate preventive measures for mitigating CDI in the Indian subcontinent.
Conclusion
C. difficile is an emerging health care-associated infection in India and causes substantial morbidity and mortality in affected individuals. Hence, there is a need for all health care institutions to implement primary prevention measures for CDI (hand hygiene, environmental disinfection, and antibiotic stewardship), suitable surveillance/testing/treatment strategies for health care facility-onset diarrhea, and finally appropriate preventive measures (contact isolation and rigorous environmental disinfection) for infected patients.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This systematic literature review was funded by Pfizer Limited.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.G. and G.R. are employees of Pfizer India. S.W. was at Pfizer, India, during the time the study was conducted, but is now affiliated with Smith and Nephew, India. The authors declare that there is no conflict of interest.
Author Contributions
All authors have contributed equally toward the concept or design of the work; or acquisition, analysis, or interpretation of data; drafted the article or revised it critically for important intellectual content; approved the version to be published and have participated sufficiently in the work to take public responsibility for appropriate portions of the content.