
Abstract
Introduction:
Neurofibromatosis type 1 (NF1) is one of the most common autosomal dominant genetic disorders. Some clinical manifestations are present at birth, while some develop during childhood, and others can occur at any age. Given the early age at which patients develop clinical features, diagnosis is often made during childhood. The most prevalent features of NF1 are café au lait spots, dermal and plexiform neurofibromas, and learning disability. A variety of skeletal problems may be seen in NF1, including scoliosis, short stature, and pseudoarthrosis. Reduced skeletal bone mass has been documented to be a common phenomenon in children and adults with NF1. Decreased serum 25-hydroxyvitamin D (vitamin D) levels have been noted in adults and children with NF1 and have been reported to be inversely correlated with the number of dermal neurofibromas in adults. However, the actual correlation of vitamin D level to bone density and dermal neurofibroma number in children with NF1 remains unclear.
Objectives:
The primary objective of this study was to evaluate vitamin D levels among children and adolescents with NF1. The secondary objective was to describe the levels of vitamin D among children and adolescents with NF1, to verify in which age group there is a higher frequency of vitamin D alterations, and to explore vitamin D level correlations between age, gender, sun exposure, number of neurofibromas, and number of plexiform neurofibromas.
Methods:
This was an observational, cross-sectional, hospital-based study. We obtained a convenience sample of individuals with confirmed diagnosis of NF1 from patients attending the Medical Genetics Service of the IPPMG-UFRJ and Santa Casa de Misericórdia of Rio de Janeiro over a 24-month period. We evaluated vitamin D levels in blood samples of patients with NF1 by a chemiluminescent immunoassay method, and we correlated the results with gender, age, number of neurofibromas, number of plexiform neurofibromas, and satisfactory sun exposure.
Results:
Of the 55 patients, 28 (50.9%) were female and 27 (49.1%) were male. Patient ages ranged from a minimum of 1.2 to a maximum of 19.6 years (mean age 10.95 years) and the median was 11.11 years. Median and mean body mass index (BMI; z score) were -0.09 (minimum value -1.63 and maximum of 4.62) and 0.16, respectively. The mean value of vitamin D was 30.82 ng/mL (±12.31) and the median was 29 ng/mL (minimum value of 10.40 ng/mL and maximum of 79.19 ng/mL).
Conclusions:
The levels of vitamin D did not differ according to gender, age group, or the presence or number of cutaneous neurofibromas. Among patients with adequate sun exposure, there was a higher incidence of sufficient serum vitamin D levels. Patients with cutaneous neurofibromas in the 0 to 11 age group had a greater tendency to vitamin D sufficiency in relation to patients aged 11 to 19 years.
Introduction
The term neurofibromatosis refers to a heterogeneous group of hereditary syndromes that lead to tumors of the central and peripheral nervous systems. By far the most common form is the neurofibromatosis type 1 (NF1, 96%), followed by neurofibromatosis type 2 (NF2, 3%) and a less known form, schwannomatosis. 1
NF1 or von Recklinghausen disease is one of the most common genetic diseases in the world population, being an autosomal dominant disease with considerable variation in severity and clinical presentation among affected individuals, and characterized by the involvement of several systems, organs and tissues of completely different embryonic origins.2-5 Patients may present stigmatizing signs of the disease such as cutaneous neurofibromas, plexiform neurofibromas and bone alterations, which may lead to embarrassment and interpersonal relationship problems.6,7
Skeletal impairment is frequent in patients with NF1. We can categorize skeletal phenotypes of NF1 as generalized or focal manifestations. Generalized skeletal manifestations (osteopenia, osteoporosis and short stature) are common, but usually mild, while focal abnormalities (tibial dysplasia, short angle scoliosis, and sphenoid wing dysplasia) are less common but cause significant morbidity. The relationship of generalized skeletal manifestations to the occurrence or progression of focal skeletal abnormalities is unknown, and the general understanding of bone growth, remodeling, and repair in NF1 is critical for therapeutic development. 8
Some studies have reported a significant decrease in vitamin D levels (25 [OH] D) in adults with NF1,9-11 in addition to decreased bone mineral density.12-14 Studies identified an inverse relationship between the number of cutaneous neurofibromas and serum vitamin D levels in adults with NF1; it is possible that patients with multiple cutaneous neurofibromas are more likely to cover the skin and therefore sun exposure is inadequate.9-15 Another explanation is that vitamin D and neurofibromin could interact at the level of cell proliferation and reducing the pro-apoptotic and antiproliferative effects of vitamin D in patients with NF1 could promote the tendency to form tumors. 9 Case-control scientific studies conducted mainly with adults showed a higher prevalence of hypovitaminosis D in patients with NF1, decreased serum 25-hydroxyvitamin D (vitamin D) levels were reported to be inversely correlated with the number of dermal neurofibromas in adults. 9
To date, there are only a few studies conducted specifically on children, and none of them in the southern hemisphere. Cases of vitamin D deficiency and vitamin D insufficiency may also be associated with bone disease and should be corrected. 16 Based on the above, this work aims to study the levels of vitamin D in children and adolescents with NF1 in Rio de Janeiro.
Objectives
The objectives were to describe the levels of vitamin D among children and adolescents with NF1, to verify in which age group there is a higher frequency of vitamin D alterations, and to explore vitamin D level correlations between age, gender, sun exposure, number of neurofibromas, and number of plexiform neurofibromas.
Method
This was an observational, cross-sectional, hospital-based study. The present study is part of the research line “Clinical and Epidemiological Study of Genetic Diseases in Childhood and Adolescence” within the Post Graduate Program in Internal Medicine of the Federal University of Rio de Janeiro Medical School (UFRJ).
A convenience sample of patients with confirmed diagnosis of NF1 was obtained among those who attended follow-up visits to the Medical Genetic Service of the IPPMG-UFRJ and the Santa Casa de Misericórdia of Rio de Janeiro in the period of 24 months. Inclusion criteria identified patients with a confirmed clinical diagnosis of NF1 according to the criteria established at the National Institutes of Health conference in 1987, in the pediatric age group (0-19 years old). Sun exposure was defined as sun exposure of upper and lower limbs for 15 to 20 minutes, at least three times per week between 10:00 A.M. and 3:00 P.M. 16
A data form was used to register the information collected. History taking and physical examination were performed after obtaining written informed consent from parent (or legal guardian) or from the patients if ⩾ 18 years of age. The presence or absence of cutaneous neurofibromas and plexiform neurofibromas was based on clinical observation. Then a date was set for blood withdrawal for vitamin D dosing.
All blood samples were collected and analyzed at the same laboratory (Lâmina Laboratory) in Rio de Janeiro. Vitamin D levels were evaluated using the chemiluminescence immunoassay method. Vitamin D deficiency was considered when 25OHD was below 20 ng/mL (50 nmol/L) and vitamin D insufficiency when blood levels were between 21 and 29 ng/mL 25OHD levels greater than 30 ng/mL are ideal for bone health. 16
The vitamin values used in this study were in accordance with the guidelines of the Brazilian Dermatology Society, which considered vitamin D deficiency if the levels were below 20 ng/mL (50 nmol/L), insufficiency if the levels were between 21 and 29 ng/mL and sufficiency if they were above 30 ng/mL. Since 2018, the guideline changed to the following: vitamin D deficiency if the levels were below 10 ng/mL, insufficiency if the levels were between 10 and 20 ng/mL and sufficiency if they were above 20 ng/mL.
The data were stored in an Excel worksheet and analyzed using the GraphPad Prism 7 program. Analysis included frequency distribution, central tendency (mean, median), and dispersion (standard deviation, maximum, and minimum limits). For comparisons, at the exploratory level, the non-parametric test (χ2) was used.
This study was approved in 2015 as part of the NF 1 research line in the UFRJ, for the post graduate program in Medicine. Therefore, the data collected were analyzed using the values of vitamin D at our disposal at the time, which were still current until 2018.
Results
The total number of patients enrolled in the IPPMG Medical Genetics Services and the Santa Casa da Misericórdia Hospital in Rio de Janeiro during the study period was 110. The number of patients eligible for the study was 85, however, 9 patients declined to participate; we were unable to contact 7 patients/caregivers and another 7 did not return with the result of the requested laboratory test. Fifty-five patients were included in the study (Table 1).
Data collected from the 55 patients enrolled in the study.

Of the 55 patients, 28 (50.9%) were female and 27 (49.1%) were male. Patient ages ranged from a minimum of 1.2 to a maximum of 19.6 years (mean age 10.95 years) and the median was 11.11 years. Median and mean body mass index (BMI) (z score) were -0.09 (minimum value -1.63 and maximum of 4.62) and 0.16, respectively. Of the total of 55 patients, 46 (83.6%) were in the eutrophic range, 7 (12.7%) were in the overweight range, 1 (1.85%) were in the obesity range, and 1 (1.85%) were in the severe obesity range. No patients were in the range of thinness or extreme thinness. None of the patients had orthopedic (minor or major) abnormalities. A positive family history of NF1 occurred in 21.8% (12/55), with maternal NF1 diagnosis among 75% (9/12) and paternal diagnosis in the remaining 25% (3/12) cases.
Cutaneous neurofibromas were present in 34.5% (19/55) of the patients. Eighteen patients (32.7%) had plexiform neurofibromas. In our sample, 13 patients (68.4%) presented cutaneous neurofibromas on the trunk.
We obtained the results of the of vitamin 25 (OH) D serum levels of 55 patients (88.7%). Mean serum vitamin D level was 30.82 ng/mL (±12.31) and the median was 29 ng/mL (minimum value of 10.40 ng/mL and maximum of 79.19 ng/mL). Of the 55 patients with vitamin D levels measured, 9 (16.4%) were vitamin D deficient, 20 (36.3%) were insufficient, and 26 (47.3%) were sufficient. Sun exposure was inadequate in 54.8% of the patients (34/62).
Serum vitamin D sufficiency (sufficient, insufficient, or deficient) was compared with adequate or non-adequate sun exposure for each patient. The distribution of patients presenting sufficient vitamin D levels and adequate sun exposure was found to be statistically significant (χ2 = 13.62; P = .0001) (Figure 1).
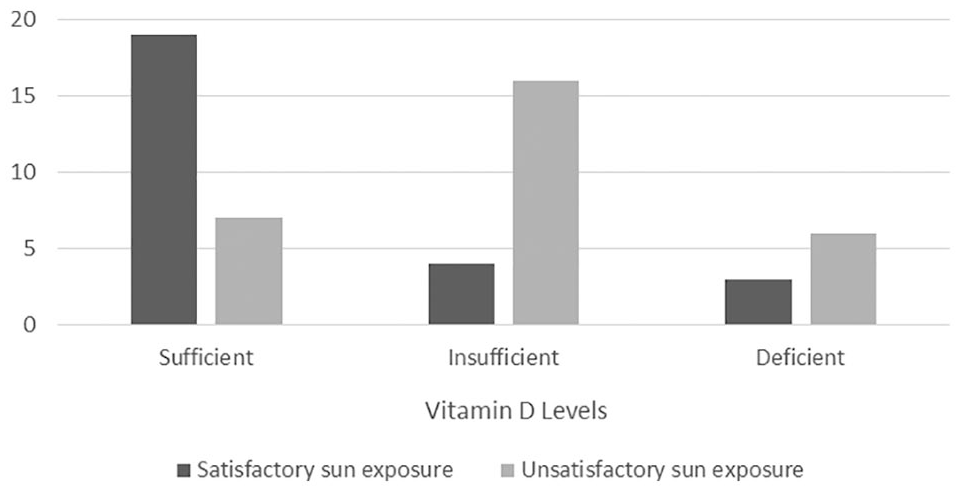
Distribution of patients by vitamin D sufficiency and sun exposure.
We did not observe a correlation between patient age and serum vitamin D sufficiency (χ2 = 3.418; P = .181) in the total patient population. However, among the patients with cutaneous neurofibromas, there was a significant correlation between age < 11 years and vitamin D sufficiency in comparison to the age range of 11 to 19 years (χ2 = 6.967; P = .030) (Figure 2).

Distribution of vitamin D levels compared to the ages of patients with cutaneous neurofibromas.
Of the 19 patients with cutaneous neurofibromas, 11 (57.9%) had sufficient vitamin D levels, 5 (26.3%) had insufficient levels, and 3 (15.8%) presented deficient levels, and no correlation between presence of cutaneous neurofibromas and vitamin D levels was observed (χ2 = 2.30; P = .317) (Table 2).
Vitamin D sufficiency by age.

Abbreviation: CNF, cutaneous neurofibroma.
The vitamin D levels of the patients with cutaneous neurofibromas were compared to gender and no statistical significance was found between the groups (χ2 = 2.12; P = .346) (Table 3).
Vitamin D sufficiency by gender.

Abbreviation: CNF, cutaneous neurofibroma.
Discussion
In this study, we evaluated vitamin D levels in a pediatric NF1 population. Vitamin D has been extensively studied and its insufficiency or deficiency has been acknowledged in some conditions17,18-21 it is much more frequent in countries of the northern hemisphere and in the elderly, due to the lack of sun exposure and the low dietary intake of vitamin D precursors. 22
Low levels of vitamin D have previously been reported in adults11,23-26 and in children10,25,27-29 with NF1. Studies in the northern hemisphere (three in Germany, two in the United States and one in Italy) of patients with NF1 showed lower levels of vitamin D in these patients as compared to the general population.10,11,23,25,27 In our population, adequate sun exposure would be expected due to the climatic characteristics of Rio de Janeiro. We found 26 patients with satisfactory sun exposure and 29 with unsatisfactory sun exposure, among those who had their vitamin D levels dosed. Significant differences were found in the distribution of vitamin D deficiency/insufficiency/deficiency categories when correlated with adequate sun exposure.
In our sample, more than half of the patients presented cutaneous neurofibromas on the trunk, an area usually covered with clothing and that would not be related to inadequate sun exposure for aesthetic reasons. Lammert et al 9 suggested that low serum levels of vitamin D could be related to less sun exposure in patients with more cutaneous neurofibromas, for aesthetic reasons of the disease.
Our results are in agreement with studies that did not identify vitamin D deficiency in pediatric patients with NF1.25,28 We did not find statistical significance related to the occurrence of low levels of vitamin D and the presence of cutaneous neurofibromas, as reported by Stevenson et al 27 However, in our study, patients with cutaneous neurofibromas in the age range of 0 to 10 years presented a greater tendency toward vitamin D sufficiency as compared to the older age range (11-19 years). We did not find any data in the literature with which to compare this result, and should be considered a new finding from this study.
The location of cutaneous neurofibromas was not explored in the scientific literature assessing vitamin D levels among the NF1 population. The number of cutaneous neurofibromas found can range from a few to thousands 5 depending on the patient, and 14% of children less than 10 years of age have cutaneous neurofibromas, compared to 44% between the ages of 10 and 19 years, 85% of patients between 20 and 29 years of age, and 94% of adults over 30. 30 In our study, cutaneous neurofibromas were present in 33.8% of the patients. Of the 19 patients presenting cutaneous neurofibromas, 9 (47.4%) were younger than 10 years of age, and 10 (52.6%) were between 10 and 19 years old, frequencies higher than those reported in the literature. However, the tendency of increased numbers of cutaneous neurofibromas with increasing age is in agreement with that reported elsewhere. This corroborates the progression of the disease characteristics.
In our study, plexiform neurofibromas were present in 35.4% of the sample, a percentage compatible with that described in the literature. The different frequencies may be related to sample type and size. Plexiform neurofibromas are considered congenital and occur in 25% to 50% of children with NF1. 31 Huson et al, 32 showed that 26.7% of the individuals presented plexiform neurofibromas at physical examination. More recently Hernández-Martín and Duat-Rodríguez, 33 found in their samples a prevalence of 10% of plexiform neurofibromas in their patients.
In our study, the location was trunk (30.5%), head and neck (25%), limbs (30.5%) and genital region (14%) not corroborating with that found in the literature. The most frequent location of plexiform neurofibromas is the trunk (43%), followed by head and neck (42%) and extremities (15%). It is common to find the involvement of the following cranial nerves: V (trigeminal), IX (glossopharyngeal), and X (vagus). These benign congenital tumors often develop in association with major nerve tracts, where they may involve multiple fascicles and branches of the nerves. 34
Children with NF1 are generally thin. 35 A Brazilian study where physical parameters of children and adolescents with NF1 were plotted on the growth charts identified 3.7% of underweight patients and 17.1% of short stature in the pediatric age group with NF1. 36 Our work differed from those above, since most of our sample presented eutrophy (89% with z-score ⩾ -2 and z-score < +1).
The sources of vitamin D include dietary intake, and also, importantly, sun exposure. 22 In our study, sun exposure was unsatisfactory in most study participants (29/55). The importance of Vitamin D in association with neurofibromin function may exert tumor suppression functions, reduce the pro-apoptotic and antiproliferative effects of vitamin D in patients with NF1 as well as promote the tendency to form tumors. 9 Therefore, it is suggested that studies with a larger number of patients and a longer period of follow-up be established, stipulating the possible correlation of inhibition of the appearance of new neurofibromas.
To date, there are still gaps in relation to vitamin D and NF1, but most of the findings in the pediatric age group indicate a decrease in the serum levels of this vitamin.10,25,27-29
Conclusion
In the evaluation of serum vitamin D levels in 55 pediatric NF1 patients evaluated, sufficiency was found in 47.3%, insufficiency in 36.3% and deficiency in 16.4%. The level of vitamin D did not vary according to gender, age group, or the presence or number of cutaneous neurofibromas. Among patients with adequate sun exposure, there was a higher incidence of sufficient serum vitamin D levels. Patients with cutaneous neurofibromas in the 0 to 11 age group had a greater tendency to vitamin D sufficiency in relation to patients aged 11 to 19 years. We suggest a larger scale study to confirm these findings.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Alessandra Santos – writing (original draft), investigation, data curation, project administration, methodology.
Mauro Geller – conceptualization, project administration, resources, supervision, validation, writing (review and editing).
Spyros Mezitis – validation, visualization, writing (review and editing).
Allan E. Rubenstein – validation, visualization, writing (review and editing).
Lisa Oliveira – formal analysis, software, validation, visualization.
Daniel J. M. Medeiros Lima – formal analysis, software, validation, visualization.
Mendel Schumacher Neto – validation, visualization.
Rafael Nigri – validation, visualization.
Karin Gonçalves Soares Cunha – validation, visualization.
Sanyu Takirambudde – validation, visualization.
Márcia Gonçalves Ribeiro – project administration, resources, supervision, validation, writing (review and editing).