
Abstract
Prostate intraepithelial neoplasia is described as a precursor lesion to prostatic adenocarcinoma. High-grade prostate intraepithelial neoplasia (HGPIN) is classified as both grade 2 and 3 prostate intraepithelial neoplasia due to inconsistency between pathologists’ findings. In our study, we assessed the interobserver variability in the diagnosis of HGPIN among genitourinary and nongenitourinary pathologists. All cases with prostate adenocarcinoma diagnosis on needle core biopsy, radical prostatectomy, and transurethral resection of prostate (TURP) between the years 2005 and 2014 were included. In total, 191 prostate cancer cases were included: 109 needle core biopsies, 45 radical prostatectomies, and 37 TURP. All were independently reviewed by 2 urologic pathologists for the presence of HGPIN. High-grade prostate intraepithelial neoplasia was diagnosed in 65 cases (34%), among which the lesion was recognized by the reporting pathologists in 36 (55%) of the cases and was missed in 29 (45%) of the cases with a κ coefficient of 0.53. There was a moderate interobserver agreement in the diagnosis of HGPIN. Consultation with genitourinary pathologist can improve HGPIN diagnosis.
Keywords
Introduction
High-grade prostatic intraepithelial neoplasia (HGPIN) is considered the most accepted precursor lesion to prostatic adenocarcinoma (PCa).1-3 High-grade prostatic intraepithelial neoplasia consists of intraluminal proliferation of atypical cells with nuclear crowding and stratification. The nucleoli are usually seen at 20× magnification.1,2 However, recognizing HGPIN can sometimes be difficult, resulting in significant interobserver variation in its identification.4-8 Therefore, recognition of HGPIN may require a pathologist with genitourinary expertise. 8
The predictive accuracy of HGPIN for PCa has declined due to multiple factors, but the major factor is the use of extended biopsy techniques. This resulted in higher cancer detection rates in the initial biopsy. 1 That said, Lee et al 9 showed that finding HGPIN in cases with PCa is associated with higher Gleason Score, multiple tumors, and more perineural invasion, and reporting HGPIN is an explicit component of the College of American Pathologists (CAP) protocol even for patients with PCa. 10
There is considerable variation in the reported incidences of HGPIN in the literature. 11 This variance is most probably due to specimen type, tissue preparation, patient biopsy selection, and inconsistency in the recognition of HGPIN lesion among pathologists. 12 As part of the checklist for the CAP prostate protocol summary, 10 pathologists are reminded to look for and report HGPIN. That said, the interobserver variability in diagnosing HGPIN is generally good to excellent according to several studies.8,13-15
The aim of our study was to evaluate the interobserver variability in the diagnosis of HGPIN lesion between genitourinary and nongenitourinary pathologists in a tertiary hospital in Northern Jordan in a cohort of patients with PCa diagnosis.
Methods
Patients and tissue samples
We retrieved 191 prostate cancer cases from the archives of King Abdullah University Hospital obtained during the period 2005-2014. These cases included the following: 109 needle cores, 45 radical prostatectomies, and 37 transurethral resections of prostate. All cases were independently reviewed by 2 urologic pathologists (N.A.D and S.A.B.) for the presence of HGPIN, and diagnostic agreement was reached in controversial cases. Clinical data, including age and preoperative prostate-specific antigen (PSA) level, were obtained from patients’ medical records. This study was approved by the Institutional Review Board of Jordan University of Science and Technology.
Results
Patient characteristics
The clinical and preoperative PSAs are summarized in Table 1. The mean age of patients included in this cohort was 73.43 years (range, 41-99 years). High-grade prostate intraepithelial neoplasia was present in only 65 cases (34%); the mean age at the time of diagnosis was 72.14 years (range, 41-90 years). Of note, intraductal carcinoma was seen in 5 cases only in our cohort, 4 of which were not recognized by the reporting pathologist. The preoperative PSA was available in the 65 patients; the mean was 106.62 ng/mL and the median 13.68 ng/mL.
Clinicopathologic characteristics of all cases with HGPIN.
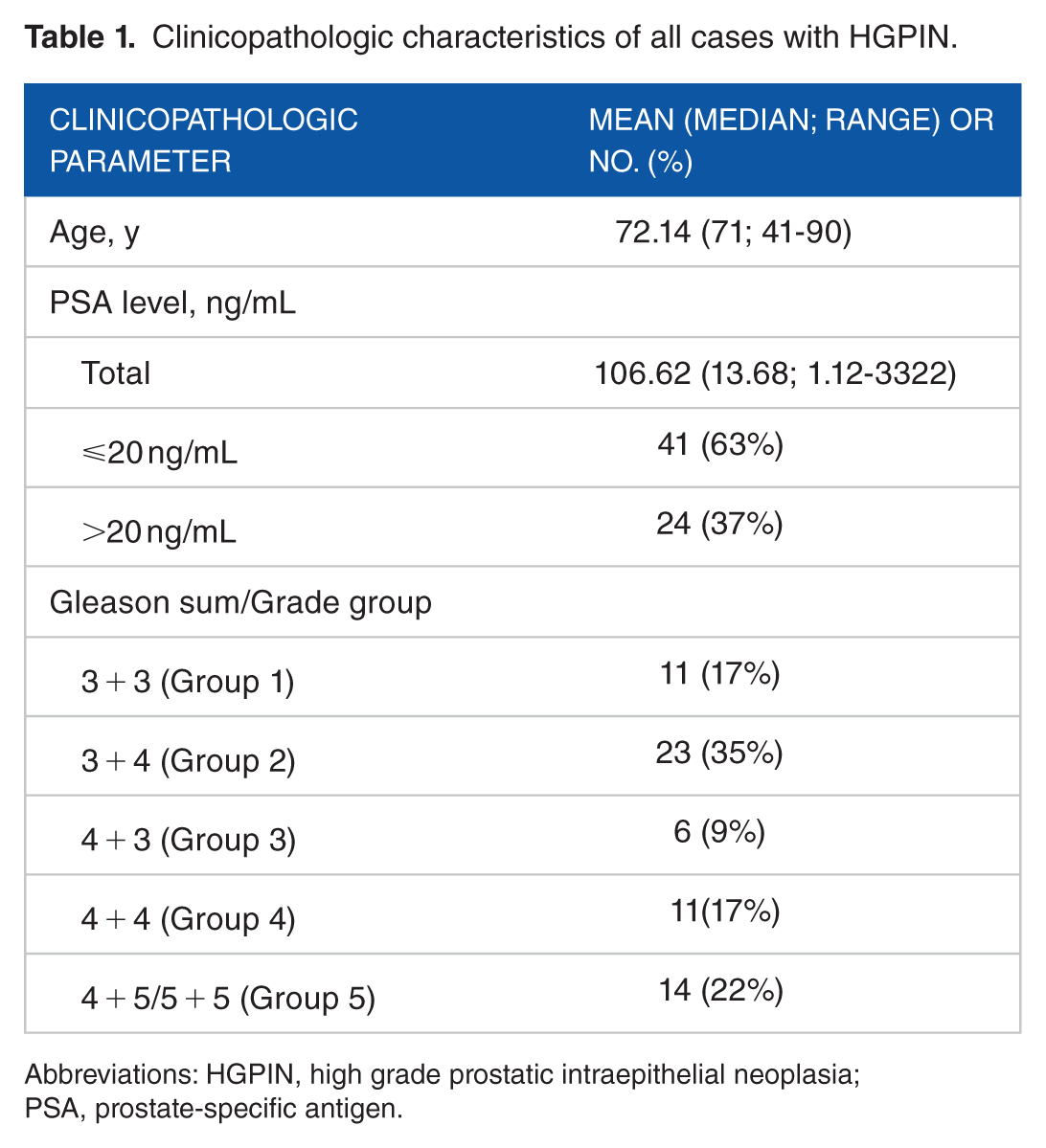
Abbreviations: HGPIN, high grade prostatic intraepithelial neoplasia; PSA, prostate-specific antigen.
Interobserver variability
Among the 65 cases of HGPIN, the lesion was recognized by the reporting pathologist in 36 (55%) and was missed in 29 (45%) cases. There was a moderate interobserver agreement with a κ statistic of 0.53.
Discussion
The 3-tier grading system for PIN dysplastic histopathology was originally established by McNeal and Bostwick. 3 Due to marked inconsistent agreement between pathologists as to whether a lesion represents grade 2 or 3, it was eventually decided that both grades share the same umbrella of HGPIN, resulting in a dichotomy of either low- or high-grade PIN that is more commonly used today.4,16
Histological characteristics of HGPIN are particularly protuberant in nature, consisting of neoplastic epithelial cells with nuclear enlargement, hyperchromasia, and prominent nucleoli.1,2 Moreover, HGPIN has the highest degree of basal cell disruption amid the other grades as reported by Bostwick and Brawer. 17
Normal prostatic tissue, metaplasia, benign proliferation, and malignant tumors may be confused with HGPIN. 4 Lesions that are fairly easy to discriminate from HGPIN are benign proliferations of basal cells and clear cell cribriform hyperplasia. 4 Malignant mimics of HGPIN include intraductal carcinoma, whether solid, cribriform, or comedo types 18 ; ductal (endometroid) adenocarcinoma; and transitional cell carcinoma of the ducts and acini.18-20
The exact predictive value of carcinoma incidence after initial HGPIN is of great disparity, fluctuating between 2% and 100%.8,21-25 Many studies have attempted to identify clinical, pathological, or molecular factors that can increase the predictive value of HGPIN and stratify patients at higher risk to develop subsequent PCa. Some of the published studies failed to find significant use of these factors in predicting PCa. 26 However, other studies have found that the presence of HGPIN, patient age, and serum PSA were significant predictors of cancer, particularly when taken together. 27 Moreover, multifocality of HGPIN and the number of cores involved were found to predict a higher risk of subsequent cancer on follow-up.28,29
Despite the importance of recognizing HGPIN, there is still insufficient uniformity in diagnosing and reporting it. The subjective diagnosis of HGPIN explains the occurrence of interobserver variability between genitourinary and nongenitourinary pathologists. As interobserver variability in low-grade PIN is high, pathologists do not routinely report this finding except for research purposes. 22 Interobserver variability generally poses a concern in the epidemiology and clinical diagnosis of prostate cancer.4,6,30 Tan et al 8 demonstrated that 75% of HGPIN lesions were initially missed by reporting pathologists when reviewing “benign” prostatic needle core biopsies. Moreover, Kronz et al 15 disclosed a 30-patient oversight of HGPIN out of 3251 prostate biopsy cases where HGPIN represented 34.5% of the missed lesions identified in the study.
Chan and Epstein 13 showed good agreement between primary and consulting outside specialists apropos discriminating benign specimens from HGPIN. Nevertheless, diagnostically significant disagreement with about one-third of all the initial diagnoses in their study was also reported. Most often, this disagreement resulted in changing an initial diagnosis of atypical foci suspicious for malignancy or HGPIN to cancer. Tan et al 8 suggested that hesitancy or general unfamiliarity in making such a diagnosis among local pathologists contributed to the inconsistency. Kronz et al 15 insinuated a cause of variability to be slide selection bias in addition to decreased accuracy upon examination due to reliance on second opinion.
Irrespective of the cause, diagnostic variability in the identification of HGPIN has important, sometimes quite unfortunate, implications for patients. In the study by Kronz et al, early distinction of HGPIN from adjacent atypical glands could have altered the clinical approach in 17 cases (0.5%) of the study. Not only do false-negative values contribute to interobserver variability, but false-positive results may also exist. Bostwick and Ma 30 showed an overdiagnosis of HGPIN in 60 (24%) of 247 cases by nonspecialists where expert consensus would indicate a benign condition. These results further attest to the difficulty of making such diagnosis among nonurologic pathologists, suggesting the likelihood of interobserver variability, and perhaps also technical quality factors, playing an additional role in the reported variation of HGPIN and PCa between populations and studies. 31
In our study, we determined the interobserver variability in diagnosing HGPIN between urologic and nonurologic pathologists in our department. In our cohort, all cases were reviewed independently by 2 urologic pathologists, and then the pathology reports were reviewed for the presence or absence of HGPIN. Among the 65 cases of HGPIN, the lesion was recognized by the reporting pathologist in 36 (55%) and was missed in 29 (45%) of the cases. There was a moderate interobserver agreement with a κ statistic of 0.53. These results fall within the range of the aforementioned studies on interobserver variability in the identification of HGPIN. Moreover, our results fall in step with the suggestion that consultation with a pathologist with genitourinary expertise could improve the accuracy with which HGPIN is diagnosed. 8
Our study has certain limitations, as we investigated the interobserver variability in HGPIN diagnosis in a cohort of patients with PCa diagnosis, at which point HGPIN is clinically irrelevant. Our aim in doing so was to see how frequent this lesion is underdiagnosed in our practice. That said, we recommend another study to determine how many isolated HGPIN diagnoses are missed in benign prostatic biopsies, which will have more clinical impact for the patients, insofar as recent studies suggest that the presence of ERG-positive isolated HGPIN in needle core biopsy can predict subsequent cancer diagnosis.32-34
In conclusion, this study highlights the interobserver variability in HGPIN diagnosis in a tertiary medical hospital in Northern Jordan. There was moderate interobserver agreement between genitourinary and nongenitourinary pathologists, with 45% of cases being missed by the reporting pathologists. Consultation with genitourinary expertise would improve the accuracy of HGPIN diagnosis. Further reporting studies on interobserver variability in the diagnosis of HGPIN are required, particularly to spread awareness and avoid unnecessary or undesirable clinical approaches in future confrontations.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the grant from the Deanship of Research, Jordan University of Science and Technology, Irbid, Jordan.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
N Aldaoud was involved in the design of the study, data collection, interpretation of the slides, and writing the manuscript. AH was involved in literature review and writing the manuscript. N Abdo was involved in statistical analysis. SAB was involved in interpretation of the slides. NM was involved in data collection. AG-B reviewed and edited the manuscript. All authors read and approved the manuscript.
Ethical Approval
This study was approved by the ethical committee of Jordan University of Science and Technology (Institutional Review Board [IRB]) in accordance with the 1964 Declaration of Helsinki and its later amendments. Formal written informed consent was not required with a waiver by the IRB.