
Abstract
Background:
Intrahepatic cholangiocarcinoma is a highly malignant tumor with a very short 5-year survival. Multistep carcinogenesis has been suggested as the main pathway for the development of this tumor. Main suggested precursors have been (1) biliary intraepithelial neoplasia (BilIN) and (2) intraductal papillary neoplasm of bile duct (IPNB). The former is flat and does not produce grossly and radiologically detectable mass lesion, but the latter produces grossly identifiable lesion.
Objectives:
The development of bile duct dysplasia (BilIN) in chronic biliary diseases has been investigated and proved, but the incidence of BilIN in non-biliary causes of cirrhosis such as hepatitis B and non-alcoholic steatohepatitis has very rarely been investigated. In this study, we have tried to find out the prevalence of BilIN in non-biliary cirrhosis.
Patients and Methods:
During the study period (2017-2018) in 100 explanted livers with the diagnosis of non-biliary cirrhosis, thorough sampling (at least 20 sections) was performed, and pathologic sections were studied for the presence of BilIN.
Results:
In the 100 studied livers with different diagnoses of non-biliary causes of cirrhosis, 31% of cases showed BilIN-1 and 2% of cases showed BiliIN-2. No case of BilIN-3 has been identified.
Discussion and Conclusions:
Non-biliary causes of cirrhosis should be considered as precursors of cholangiocarcinoma (BilIN); however, the incidence of this occurrence is low.
Introduction
The most common malignant tumor of the biliary tract in the liver is intrahepatic cholangiocarcinoma (ICCA), which has a very poor prognosis and a 5-year survival of less than 20%. Early diagnosis of this tumor and its precursors is very important for surgical resection when it is amenable to be resected. 1
Recent studies have shown the role of multistep carcinogenesis in the pathogenesis of ICCA leading to a general concept of hyperplasia-metaplasia-dysplasia-carcinoma sequence.2,3
In these steps, several precursors have been identified, most common and well documented of which are 2 premalignant biliary changes, that is, intraductal papillary neoplasm of the bile duct (IPNB) and biliary intraepithelial neoplasia (BilIN) (flat or low-papillary biliary dysplasia). The former produces mass lesion and the latter is a flat and microscopic lesion. 1
Biliary intraepithelial neoplasia is a preneoplastic epithelial lesion with cytologic atypia, which is categorized based on the degree of cytologic atypia such as BilIN-1, BilIN-2, and BilIN-3. 1
As it has been mentioned, BilIN is a microscopic lesion with no grossly identifiable mass lesion, so radiologic findings are not helpful in diagnosis of these lesions. The gold standard for the diagnosis of BilIN is pathologic examination. 1 The BilINs do not produce mass lesion, so detection of them requires complete random sectioning and thorough sampling of the suspected specimen such as explanted liver. 4
There are not so many studies regarding the frequency of BilIN, which majority of them have investigated these lesions in biliary diseases. In our previous experience with the explanted livers of the patients with biliary-type cirrhosis secondary to primary sclerosing cholangitis (PSC) as the most important precursor of ICCA, the frequency of BilIN was very low.5,6 In this study, we tried to evaluate the frequency of BilIN in explanted livers of non-biliary cirrhotic livers.
Patients and Methods
During 2 years (2017-2018), in the affiliated hospitals of Shiraz University of Medical Sciences, 100 explanted cirrhotic livers with various non-biliary underlying causes were evaluated for the presence or absence of BilIN in intrahepatic biliary tract. For each specimen, the patient’s clinical chart was evaluated, and clinical findings, including sex, age, and cause of liver cirrhosis, were recorded and correlated with the pathologic diagnosis. The study population were 68 men and 32 women, mean age of 44.7 ± 17 (range, 6-69 years) with different primary causes. Tables 1 and 2 show the underlying causes of these 100 cases of cirrhosis.
Underlying causes of cirrhosis in 100 non-biliary cases of cirrhosis examined for the presence of BilIN.

Abbreviation: BilIN. biliary intraepithelial neoplasia.
Prevalence of BilIN in explanted livers with non-biliary cirrhosis according to the underlying cause of cirrhosis.
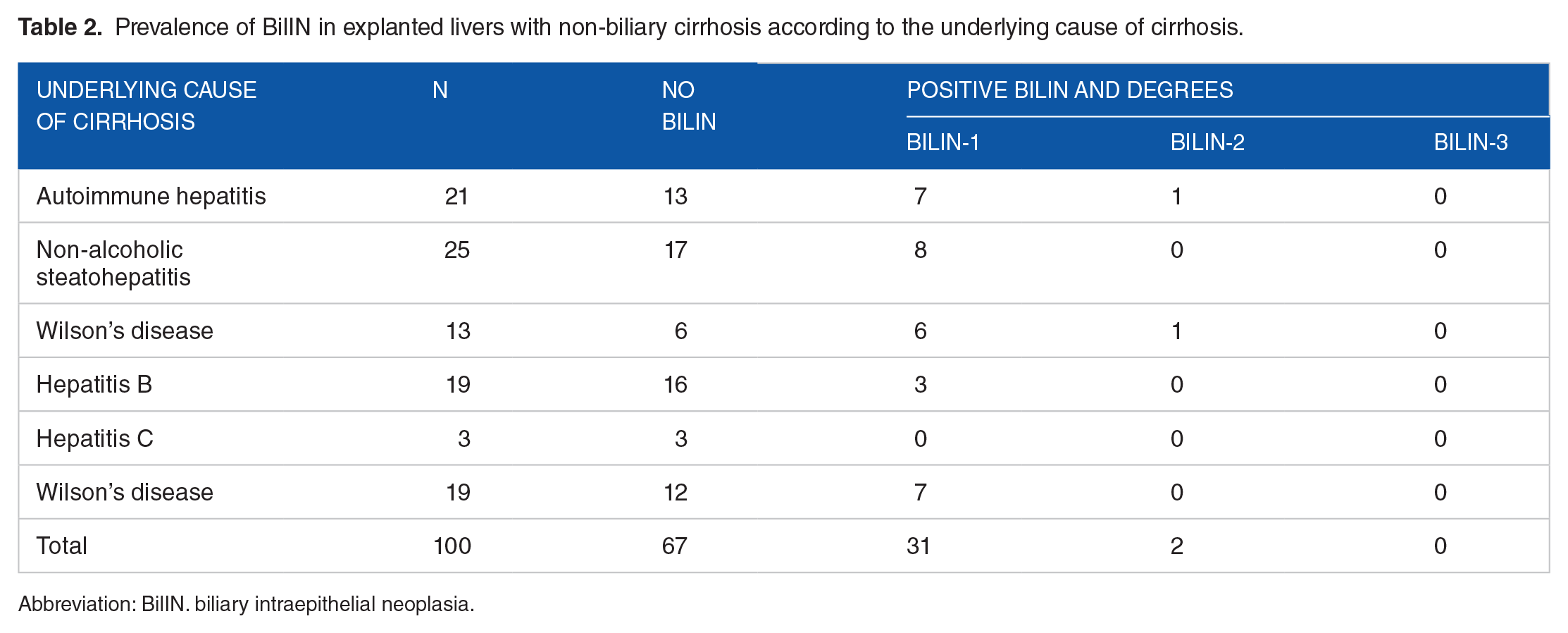
Abbreviation: BilIN. biliary intraepithelial neoplasia.
For the diagnosis of BilIN, thorough sampling was done from the large hilar and septal intrahepatic bile ducts. The sections were randomly taken because no grossly abnormal finding was seen. In each case, at least 20 sections were taken and were evaluated under the microscope by an expert hepatopathologist (B.G.).
Diagnosis and grading of BilIN have been performed according to the documented criteria. 3 Briefly, in BilIN-1, ducts have mucinous metaplasia and there is only minimal nuclear atypia, enlargement, and crowding. BilIN-2 contains ducts with obvious nuclear stratification and low-grade dysplasia, but atypia is less than high-grade dysplasia. In BilIN-3, ducts show intense cytologic atypia and loss of nuclear polarity that reaches the luminal surface. 7
Results
Among the 100 studied livers with non-biliary cirrhosis, 31 cases showed BilIN-1 and 2 cases showed BilIN-2, but no BilIN-3 was seen in any case. Therefore, the overall prevalence of BilIN-1 and BilIN-2 in our study population was 31% and 2%, respectively. None of the cases with the diagnosis of BilIN showed any histologic evidence of inflammation or bile duct epithelial damage.
In 21 cases of BilIN, there has been multiple BilIN in the same case, that is, 80% of the cases with the diagnosis of BilIN had multiple lesions; however, both cases with the diagnosis of BilIN 2 had a single lesion.
Among 31 cases with BilIN-1 (Figures 1 and 2), 7 cases show that the primary cause of liver cirrhosis was autoimmune hepatitis, 8 cases of non-alcoholic steatohepatitis (NASH), 6 Wilson’s disease, 3 hepatitis B, and 7 cases were cryptogenic cirrhosis. All of the BilINs have been in the perihilar and segmental bile ducts, that is, in the bile ducts with the diameter more than 400 µm.

Section from septal bile duct with BilIN-1 (upper figure: H&E, ×250, lower figure: H&E, ×400). BilIN indicates biliary intraepithelial neoplasia; H&E, hematoxylin and eosin.

Sections from septal bile duct show BilIN-2 (H&E, ×250). BilIN indicates biliary intraepithelial neoplasia; H&E, hematoxylin and eosin.
One of 2 cases that contained BilIN-2 was a 34-year-old woman, case of liver cirrhosis with the underlying cause of autoimmune hepatitis, and the other one was a 35-year-old man, case of liver cirrhosis due to Wilson’s disease.
Discussion
Cholangiocarcinoma (CCA) is a malignant tumor originating from epithelial cells of bile ducts. Cholangiocarcinoma is either intrahepatic or extrahepatic. The incidence of ICCA is increasing, and its 5-year survival of ICCA is still very low. 8 Earlier diagnosis of precursor lesions of CCA can be beneficial for improving the prognosis of this highly malignant tumor. 9
There are several well-documented risk factors for ICCA such as PSC, parasitic diseases, and chemical agents. Other non-biliary chronic liver diseases and cirrhosis have long been identified as a significant risk factor in the development of hepatocellular carcinoma, but recently a similar pathogenesis has also been suggested for ICCA and its precursors. 9
Biliary intraepithelial neoplasia has been proven to be non-invasive precursor lesions of ICCA. Biliary intraepithelial neoplasia and its significance to biliary carcinogenesis have extensively been investigated in chronic biliary diseases, such as PSC, hepatolithiasis, or liver fluke infestations, because these are main known risk factors for the development of CCA, but much less investigation has been made about other major predisposing factors of ICCA, such as non-biliary cirrhosis secondary to chronic viral hepatitis, and NASH. As has been mentioned before, recent studies suggested that liver cirrhosis associated with the non-biliary diseases such as chronic hepatitis C virus (HCV), particularly in conjunction with alcohol, may be related to biliary dysplasia of large bile ducts. 7
In the current study, we tried to investigate the frequency of BilIN in other non-biliary cases of cirrhosis such as NASH and hepatitis B–related cirrhosis. We performed this research by thorough sectioning of the biliary tracts of the explanted livers with the diagnosis of non-biliary cirrhosis after transplant. The overall frequency of high-grade BilIN (BilIN-2 and 3) in non-biliary cases of cirrhosis was very low, and no case of BilIN-3 and only 2 cases of BilIN-2 have been identified. This frequency has very rarely been investigated in the previous literature, and to the best of our knowledge, less than 5 studies have been reported. In the study conducted by Wu et al in the United States, on a population consisting of several groups with chronic non-biliary diseases including liver explants with alcoholic cirrhosis (n = 94), hepatitis C–related cirrhosis (n = 44), and non-cirrhotic liver diseases (n = 80) (livers removed for metabolic disorders and massive hepatic necrosis), prevalence of BilIN (each grade 1, 2, and 3) was investigated. In the cases of alcoholic cirrhosis, this prevalence was 35%, 57%, and 4%; in the cases of HCV cirrhosis, this prevalence was 55%, 20%, and 7%, and in non-cirrhotic cases, this prevalence was 39%, 16% and 0%, respectively. 10 Similar to our findings, the prevalence of BiIN-3 has been very low, but they concluded that overall prevalence of lower grades of BilIN in HCV and alcohol-related cirrhosis is not low. 10 Another study from the United States, by Torbenson et al, 11 showed very similar results. The study, by Aishima et al 7 from Japan, revealed lower incidence of BilIN, that is, it was present in 11% of non-biliary liver cirrhosis cases (hepatitis B and hepatitis C related) and 51% of liver cases with biliary disease.
All of the BilINs in this study, that is, in our non-biliary cirrhosis cases, have been in the perihilar and segmental bile ducts, that is, in the bile ducts with the diameter more than 400 µm. This has been the same of our previous experience in biliary-type cirrhosis and also in the previous reports.5,7,10,11
According to the previous studies and our results, BilIN can occur in non-biliary conditions. It means that cirrhosis per se is a predisposition for neoplastic transformation of the biliary epithelium. 10 However, it seems that in certain causes of cirrhosis such as alcohol, the risk is higher than causes such as hepatitis B.7,10,11
Conclusions
Non-biliary cirrhosis can definitely be a risk factor for neoplastic transformation of biliary epithelium; however, its incidence is low and depends on several factors and may be related to geographic location or underlying cause of the cirrhosis. Further cohort studies with both histology and immunohistochemical methods are necessary to definitely identify the risk of ICCA in non-biliary cirrhosis and chronic non-biliary liver diseases.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by Shiraz University of Medical Sciences (grant number: 12991).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MZ: Sectioning of the livers, looking on the slides, analysis of data. AS, KK, MD, and SAM: Surgery of the cases. BG: Idea of the study, evaluating and diagnosis of the cases by looking at the slides, writing the paper.
Ethical Approval
This study has been reviewed and approved by the ethic comittee of Shiraz University of Medical Sciences.