
Abstract
Sub-acute liver failure is a term that describes the relatively sudden loss of liver function, usually >21 days and <26 weeks, with impaired synthetic function and associated encephalopathy in a person with no pre-existing liver disease or cirrhosis. It is commonly caused by viruses and drugs, less so by malignancy. Our patient is a 71-year-old Japanese man who presented with signs of sub-acute liver failure. A subsequent liver biopsy demonstrated involvement by B-cell non-Hodgkin lymphoma. Evaluation of the bone marrow demonstrated significant marrow involvement by B-cell lymphoma. The fluorescence in situ hybridization (FISH) returned positive for t(14; 18). Noted was the patient’s clinical presentation of cholestasis secondary to hepatic lymphoma with no evidence of lymphadenopathy or peripheralized lymphoma. Given the disease distribution, the overall findings are consistent with primary hepatic follicular lymphoma as described in few case reports and small case series in the literature.
Introduction
Primary hepatic lymphoma is a lymphoma confined to the liver. It is a rare entity of which diffuse large B-cell lymphoma is the most common subtype. Sub-acute liver failure is an uncommon presentation of primary hepatic lymphoma. Herein, we present a patient who presented with sub-acute liver failure and jaundice due to primary hepatic follicular lymphoma. Follicular lymphoma is a very rare subtype of primary hepatic lymphoma with a single case series published to date. 1 We discuss the case and review the literature.
Case Presentation
A 71-year-old Japanese man was admitted with new onset jaundice, leg swelling, abdominal distention, pruritus, multiple ecchymotic lesions, and mild behavioral changes. He reportedly had history of easy bruising, epistaxis, and bright red blood per rectum, which worsened around 3 days prior. He reported recent intake of 1600 mg of ibuprofen and 4 g of acetaminophen, taken over a period of 3 days, about 8 days prior to presentation. In addition, patient reported a 20-year history of alcohol abuse. On examination, patient was icteric, with multiple ecchymotic lesions.
Labs showed severe thrombocytopenia and moderate neutrophilic leukocytosis. He had elevated total bilirubin (9.7 mg/dL), Aspartate Transaminase (AST) of 645 U/L, Alanine Transaminase (ALT) of 175 U/L, and Alkaline Phosphatase (ALP) of 834 U/L. Prothrombin time (PT)/International Normalized Ratio (INR)/activated partial thromboplastin time (APTT) were 13.6/1.29/43 seconds, respectively. Toxicology screen was negative. Creatinine was 5.33 mg/dL, estimated glomerular filtration rate 11 mL/min, sodium 124 mmol/L, and blood urea nitrogen 42 mg/dL. Ammonia was <10 umol/L, ceruloplasmin level was normal at 39.9 mg/dL. Hepatitis panel, Quantiferon tuberculosis gold assay, and Human Immunodeficiency Virus antibodies were negative. Cytomegalovirus (CMV) IgG Ab was 2.5 U/mL, Epstein Barr Virus (EBV) capsid Ag IgG Ab was 225 U/mL, and EBV Nuclear Ag Ab titer was 224 U/mL. Autoimmune markers were within normal limits.
Computed tomography (CT) scan of the abdomen showed hepatomegaly with mild diffuse hepatic fatty change and mild anasarca characterized by small volume ascites and small bilateral pleural effusions. Magnetic resonance (MR) imaging of the abdomen showed hepatomegaly without evidence of diffuse infiltrative process or hepatic mass, but there was nonspecific peri-portal edema, which was favored to be secondary to hepatitis. Computed tomography of the chest did not show any visible lymphadenopathy but showed small bilateral pleural effusions.
Drug induced liver injury and alcoholic cirrhosis were initial considerations. Over the course of hospitalization, patient’s condition deteriorated with worsening coagulopathy, neutropenia, and anemia requiring multiple transfusions of blood products including factor concentrates. Progressive renal failure required hemodialysis.
A liver biopsy was performed and pathology revealed an atypical proliferation of small/medium-sized lymphoid cells involving the hepatic parenchyma (Figure 1). Immunohistochemical studies (IHC) showed a marked predominance of atypical CD20-positive B-cells consistent with B-cell lymphoma (Figure 2). The lesional cells were predominantly distributed within sinusoids with expansion and forming medium-sized atypical aggregates involving portal tracts, evidenced by intact bile ducts centered within the aggregates (Figure 3). There was no evidence of large nodules or sheets of large cells. Additional IHC studies showed aberrant co-expression of BCL6 and fluorescence in situ hybridization (FISH) studies positive for t(14; 18) most consistent with follicular lymphoma, grade 1 to 2. A bone marrow biopsy showed significant involvement by lymphoma. Epstein Barr Virus in situ hybridization studies were negative. The background liver showed features of obstructive cholestasis. There was no evidence of peripheralized lymphoma by flow cytometry.

The liver is involved by an atypical small lymphoproliferation within sinusoids and forming atypical expansile aggregates involving portal tracts. There was no evidence of large nodules or sheets of large cells. The histologic differential includes acute hepatitis (hematoxylin-eosin, original magnification ×10).
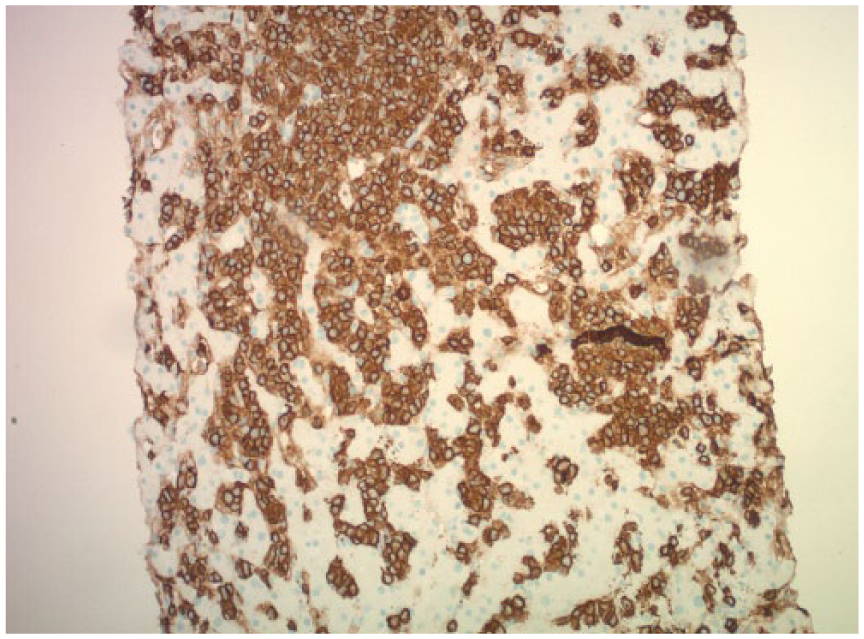
CD20 immunostaining highlights the atypical lymphoproliferation extensively involving the sinusoids (original magnification ×10).
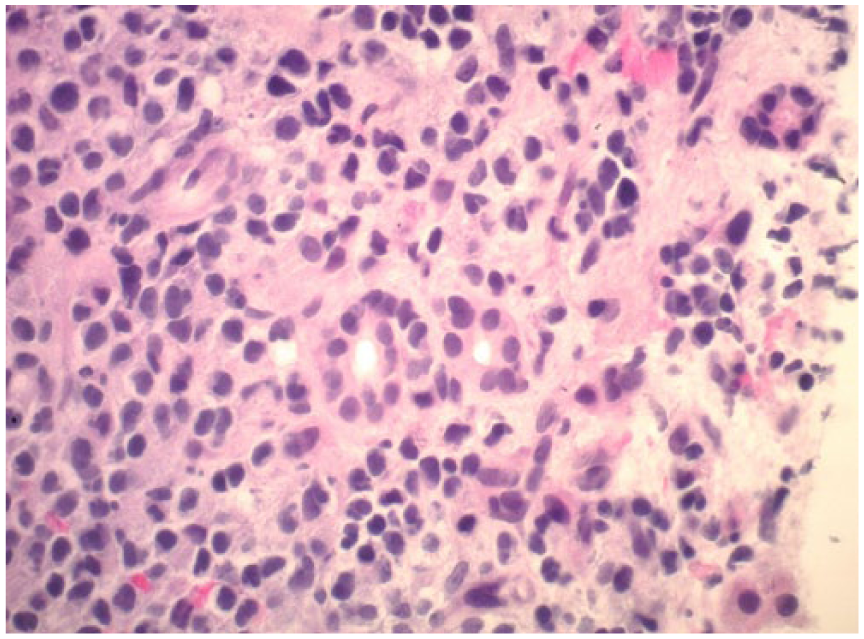
The atypical lymphoid cells are small/medium in size with variable irregular hyperchromatic nuclei. Note the bile ducts in the center of the field (hematoxylin-eosin, original magnification ×40).
He received a total of 4 weeks course of rituximab and 2 weeks course of melfalan chemotherapy. Adriamycin was not started due to significant hyperbilirubinemia. During hospital stay, total bilirubin was elevated up to 48.9 mg/dL which slightly improved after commencement of chemo, in addition to reduction in transaminases. He remained coagulopathic with INR of 2.03, APTT of 126 seconds, and PT of 21.4 seconds. Lactic acid increased up to 16.3 mmol/L. He also developed increasing ascites and paracentesis showed elevated polymorph nuclear cell count of >250 cells/mm3. Because of this, appropriate treatment for spontaneous bacterial peritonitis was initiated.
Our patient died 40 days after admission due to septic shock, atrial flutter, acute renal failure, and eventual hypoxic respiratory failure.
Discussion
Follicular lymphoma is a very rare subtype of primary hepatic lymphoma with a single case series published to date. 1 It is a routinely diagnosed lymphoma with a typical presentation of peripheral lymphadenopathy and involves malignant histologic transformation of follicular B-cell and chromosomal rearrangements of BCL-2. Due to the unique pathologic and genotypic features, follicular lymphoma is a well-defined entity easily distinguished from other small B-cell non-Hodgkin lymphomas, such as chronic lymphocytic leukemia or mantle cell lymphoma. Follicular lymphoma is graded by counting the number of centroblasts in neoplastic follicles. In contrast, primary hepatic follicular lymphoma is a very rare disease.
To our knowledge, only 9 cases have been reported in the literature. 1 Similar to our case, most cases were patients from Japan. Our case is unique because of its uncommon presentation of sub-acute liver failure without any nodular involvement of the liver or lymphadenopathy on imaging studies.
Acute liver failure secondary to malignant infiltration and its association with hepatomegaly, lactic acidosis, and death soon after onset of symptoms were described in case reports. 2 Our patient’s lactic acid was not elevated on admission but increased prior to death. The mechanism of liver failure is likely from cholangitis, ischemia, and necrotic injury following infiltration of small hepatic bile ducts.3,4 Microscopy of liver biopsy sections demonstrated liver parenchyma partially obliterated by an atypical lymphoid infiltrate. These lymphoid cells were mostly small to medium in size with irregular nuclear contours and mature chromatin features. The uninvolved portions of liver showed features of obstructive cholestasis. In addition, the release of IL-6 and other circulating cytokines from cancer cells possibly contribute to abnormal liver function tests, reflecting presence of cholestasis, similarly occurring in Stauffer syndrome.
In our patient, the FISH returned positive for t(14; 18) BCL2/IgH rearrangement. No evidence of a “double/triple hit” lymphoma was identified. The high risk “double/triple” hit lymphomas are characterized by a MYC translocation combined with a BCL2 and/or BCL6 translocation in the appropriate morphologic setting.
Summary
In summary, our patient was a 71-year-old man who presented with signs of sub-acute liver failure due to primary hepatic follicular lymphoma. This was a clinicopathologic diagnosis as there was no clinical or radiologic evidence of lymphadenopathy or other mass lesions. There was no evidence of peripheralized lymphoma confirmed by flow cytometry. Due to the insufficient number of cases, the entity is not recognized by the World Health Organization (WHO) 2017 tumor classification of hematopoietic and lymphoid tissues. Primary hepatic follicular lymphoma do not always present with nodules or radiological findings. We hope that by reporting this case and adding to the literature about primary hepatic follicular lymphoma presenting as acute or sub-acute liver failure, this rare entity will be considered in the clinical and pathologic differential. An association with people from specific regions such as Southeast Asia can be correlated. Knowledge of atypical presentations should be considered in patients with acute liver failure to provide earlier initiation of treatments and an adequate window for treatment and liver transplantation.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
M-JW contributed to the conception and design; acquisition, analysis, and interpretation of the data; drafting of the article; critical revision of the article for important intellectual content; and final approval of the article. HA contributed to the critical revision of the article for important intellectual content and final approval of the article. OK contributed to the drafting of the article, critical revision of the article for important intellectual content, and final approval of the article.
Informed Consent
Informed consent was obtained for this case report.