
Abstract
Background:
Sexual dysfunction is frequently observed among individuals with mental illnesses and is usually not given due importance in routine clinical practice. Existing rating scales are limited by narrow domain coverage, a lack of proper quantification, complex language, and poor cultural adaptability, particularly in the Indian context. Hence, there is a need for a comprehensive and culturally sensitive instrument to assess sexual dysfunction, including medication-related problems in the Indian context.
Aim:
To develop a new scale for the assessment of sexual dysfunction and establish its face and content validity.
Method:
The study was conducted in three phases at a tertiary care hospital. In Phase I, expert discussions identified core domains relevant to sexual functioning. In Phase II, items were generated through literature review and focused group discussions, followed by translation, back-translation, and linguistic simplification into English and Hindi. In Phase III, 16 mental health professionals initially evaluated the preliminary version for subjective content validity. This was followed by an evaluation of face validity among 20 sexually active participants, and 11 psychiatrists evaluated the content validity.
Results:
The final scale comprised 38 items for males and 34 items for females, covering six domains: availability of safe space for sexual activity, sexual encounter(s), sexual functioning, change in sexual practices with onset of illness and starting medications, sexual inquiry in doctor-patient interaction, and sexual functioning during the ongoing medications. Most items demonstrated high face validity (item impact score >1.5) and satisfactory content validity (CVR ≥ 0.59 for 30 items).
Conclusion:
The newly developed scale showed strong face and content validity and appears suitable for assessing sexual dysfunction in psychiatric populations. Further studies are warranted to evaluate its test-retest reliability, and clinical applicability.
Keywords
Introduction
Rating scales play an integral role in assessing various aspects of sexual functioning. Over the years, various rating scales have been designed to evaluate different aspects of sexual dysfunction and other sexual disorders. Some of these scales assess a specific aspect of sexual functioning, a specific sexual dysfunction, or other aspects of sexual disorders. In contrast, others are more general and assess multiple domains of sexual functioning. 1
When one looks at the scales available for the assessment of sexual dysfunction, these can be broadly divided into generic scales, those that assess multiple domains of sexual dysfunction, and scales that are specific to the evaluation of a single domain of sexual functioning (such as erection, ejaculation, etc.). All these scales have their advantages and disadvantages. 1 Due to the same, any one given scale does not provide a comprehensive assessment of sexual dysfunction. When one takes a close look at these scales, most of them do not cover all the aspects of sexual dysfunctions, especially those associated with the use of psychotropic medications, for example, retrograde ejaculation. Furthermore, most of these scales have not been validated in India, and these are also not available in local languages. The ratings for many of these scales also lack descriptions of the anchor points. This often limits patients’ understanding, making it difficult for them to choose the best possible option that applies to them. Hence, there is a need to develop a rating scale for the assessment of various sexual dysfunctions, including those associated with psychotropic medications. Accordingly, this study aimed to develop a scale for the evaluation of sexual dysfunction and assess the face and content validity of the same.
Methodology
This study was conducted in a tertiary care hospital, and all the participants were enrolled after obtaining informed consent. The study was approved by the ethics committee of the institute where it was conducted and all the participants were enrolled after obtaining informed consent. The study was conducted in three phases, as described below.
For Phase I of the study, at the first step, a focused group discussion was conducted involving five experts to discuss the various aspects of sexual functioning and various contextual factors that are important for understanding proper sexual functioning or any sexual dysfunction in persons with mental illnesses. Based on this focused group discussion, the areas that were considered to be important while evaluating sexual functioning/dysfunction included: availability of safe space for sexual activity, sexual encounter(s), sexual functioning, change in sexual practices with onset of illness and starting medications, sexual inquiry in doctor-patient interaction, and sexual functioning during the ongoing medications.
In Phase II, all the available scales were reviewed for the description of the “stem of the questionnaires,” and based on this review, the different questions were framed. For the areas for which guiding questions were not available in any scales, the questions were framed de novo after having focused group discussions. Initially, the questions and response options were framed in English. Three experts reviewed the English items, and a consensus version was made (initial English version). While framing the various items, the primary focus was to keep the language as simple as possible. Then, the questions and responses were translated into Hindi by three bilingual experts (psychiatrists/psychologists), and a consensus was drawn to finalize a Hindi version. For ease of understanding, if necessary, during translation, further adjustments were made to the Hindi version to keep it simple and understandable. Once the Hindi version was finalized (initial Hindi version), it was compared with the initial English version, and necessary changes were made (edited English version). The initial Hindi version was also back-translated to English by a separate set of three experts (psychiatrists/psychologists), and these back-translated versions were compared with the edited English version. Depending on the need, further changes were made in the Hindi version (edited Hindi version) if required. Finally, the English and Hindi versions were reviewed by bilingual experts to ensure their comparability and simplicity of language; the final versions were then accepted. While framing the various items, the primary focus was to keep the language as simple as possible, so that the questions could be easily understood by lay persons with a primary level of education. While framing the responses, descriptions were formulated for each response for better understanding.
The initial final English and Hindi versions were sent to 16 mental health professionals (who were themselves sexually active) to evaluate the initial subjective content validity. They were also asked to provide any further suggestions regarding the inclusion/exclusion of any item and the language of the scale. Based on the inputs, the questions and responses of the scale were further modified.
The final version of the scale consisted of 38 items for males and 34 items for females. The first section consisted of two questions covering the availability of a safe space for sexual activity. The second section covered sexual encounters with four questions, and the third section had 20 (16 for females) questions evaluating sexual functioning. Depending on gender, this section had different questions for males and females. The fourth section has two questions assessing the change in sexual practices with the onset of illness and starting medications. The fifth section has seven questions assessing discussion about sexual problems during the clinical encounters and a final section that evaluates the association of sexual functioning and medications, including three questions. The response categories for each question were framed in such a way that, wherever possible, these could be quantified by using percentages. Further, the items of the scales are worded in such a way that this could be used as a clinician-administered questionnaire or a self-administered questionnaire.
In Phase III, the scale was sent to 11 experts (psychiatrists) to evaluate the content validity. They were asked to rate each of the items on a three-point scale, that is, not necessary, helpful but not essential, and essential. They were also requested to add any comments about the questions or give options, in terms of the simplicity of language or the type of responses.
The scale was also sent to 20 sexually active persons to assess the face validity, using a five-point scale for each item. Each item was rated by the participants on a five-point scale (1 = unimportant, 2 = slightly important, 3 = relatively important, 4 = important, and 5 = very important).
Statistical Analysis
All analyses were done using Statistical Package for the Social Sciences (SPSS) version 14. Descriptive analysis was done using mean, standard deviation, and range for continuous variables. Frequency and percentages were used for categorical variables. Face validity was evaluated for each item and the full scale. We also evaluated the content validity of each item.
Results
In the initial subjective content validity step, the questionnaire was sent to 16 sexually active persons (eight males, seven females, and one person with the same-sex orientation). As evident from Table 1, the majority of the participants considered that the questionnaire would be helpful in a large extent or very useful for clinicians dealing with psychiatric patients for assessment of sexual dysfunction. When asked “to what extent will this questionnaire be useful for the patients to report their sexual symptoms?”, the majority of the participants again rated the questionnaire to be helpful to a large extent or very useful. Similarly, when asked about coverage of the questionnaire in terms of detailed sexual functioning assessment and sexual side effects reported by the patients, all of the participants considered the same to be good or very good. In terms of the length of the Questionnaire, about half of the participants reported it to be lengthy. The language of the scale was reported to be average or simple by all the participants. The participants suggested the deletion/clubbing of five items from the questionnaire and proposed the inclusion of eight more items. The participants also gave an additional 14 suggestions with respect to the wording of questions and options.
Findings of Subjective Content Validity of the New Sexual Scale.
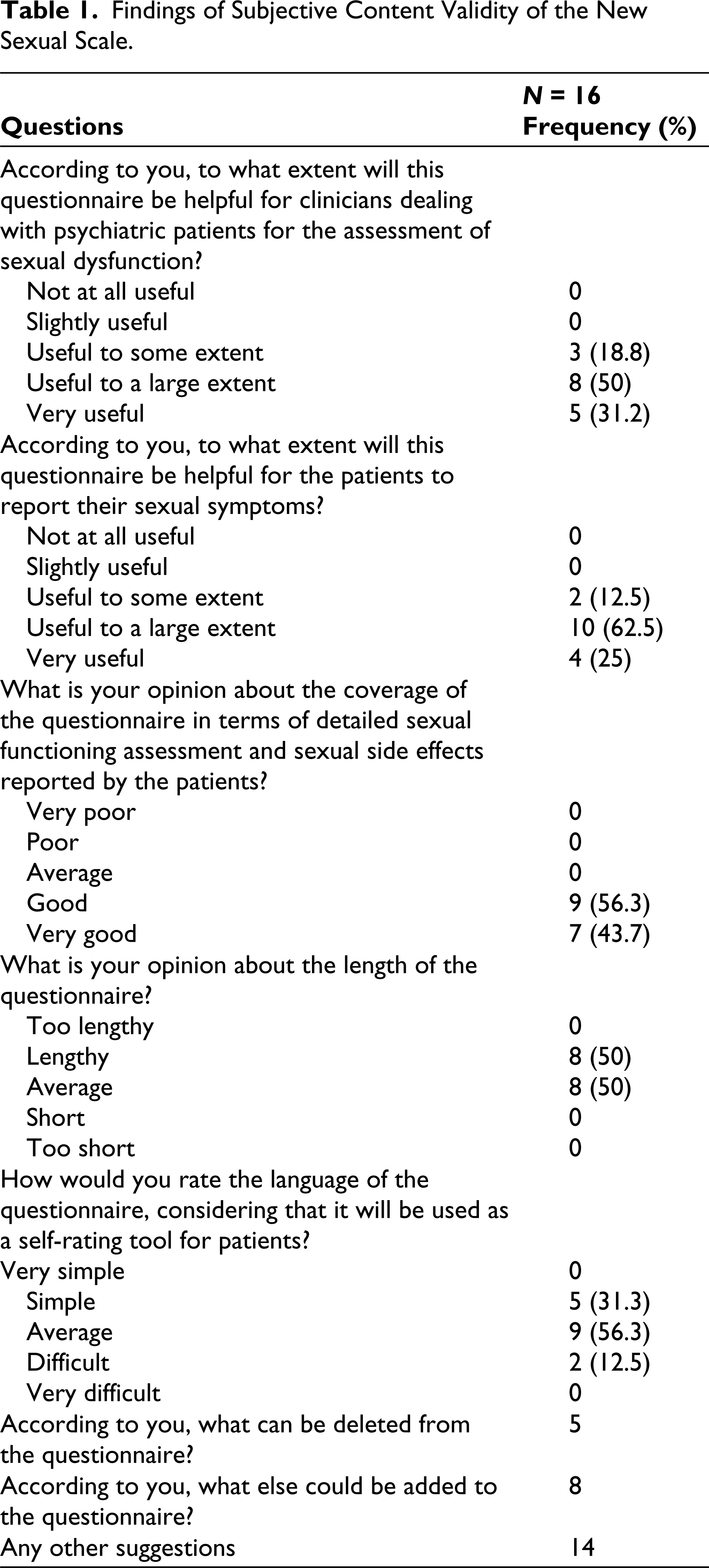
All the information from the initial subjective content validity step was used to refine the questionnaire based on further focused group discussion, before the final version was accepted. This information was also used to refine the language of the questionnaire.
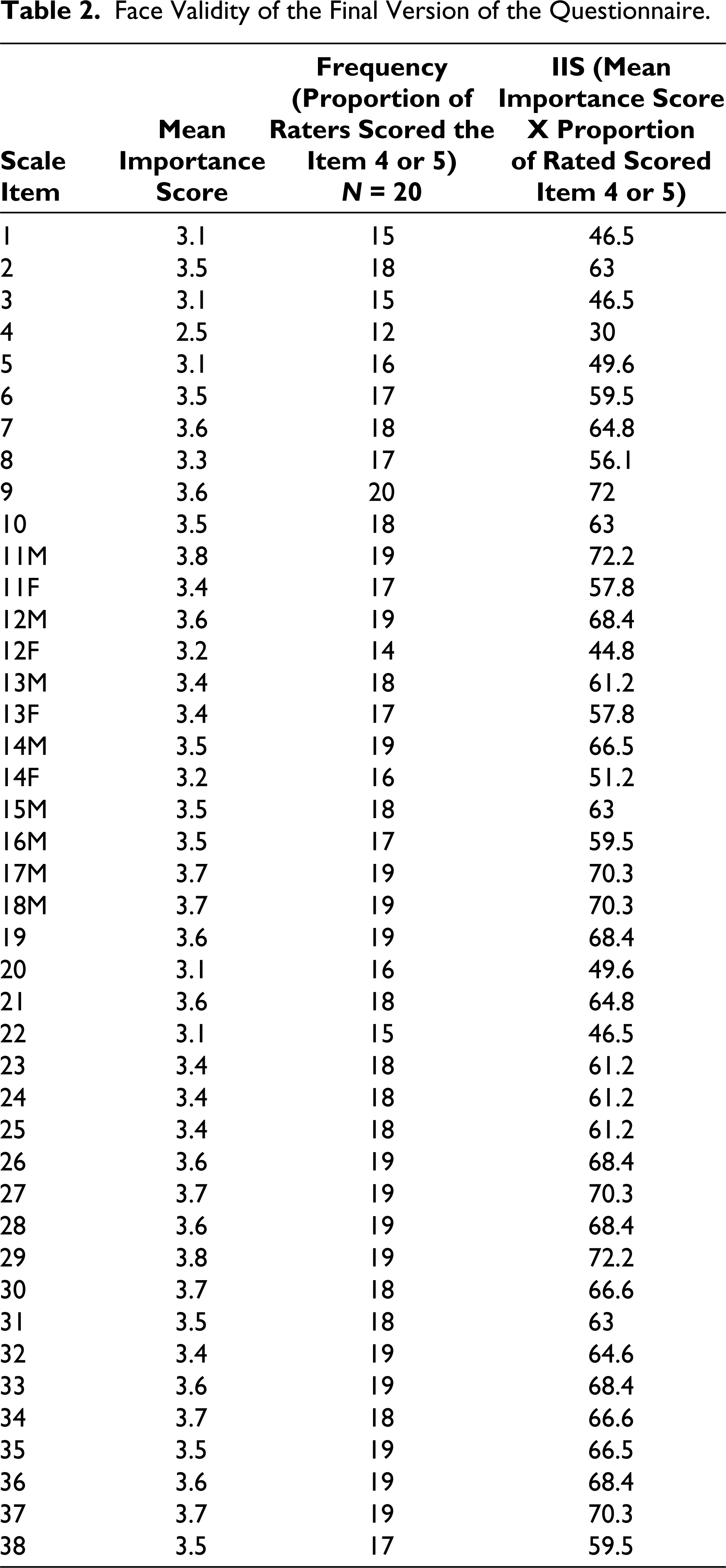
For the face validity, the scale was given to 20 sexually active persons (male = 5; female = 14; same-sex orientation = 1). All of them had at least a graduate level of education and were sexually active. All of them rated each item on a five-point scale (1 = unimportant, 2 = slightly important, 3 = relatively important, 4 = important, and 5 = very important). As evident from Table 2, except for Item 4 and Item 12 for females, all other items were rated as important or very important by 75% or more of the participants. The individual item impact score (IIS) for each item was more than 1.5, which is a recommended cut-off for retaining an item in the scale.
Face Validity of the Final Version of the Questionnaire.
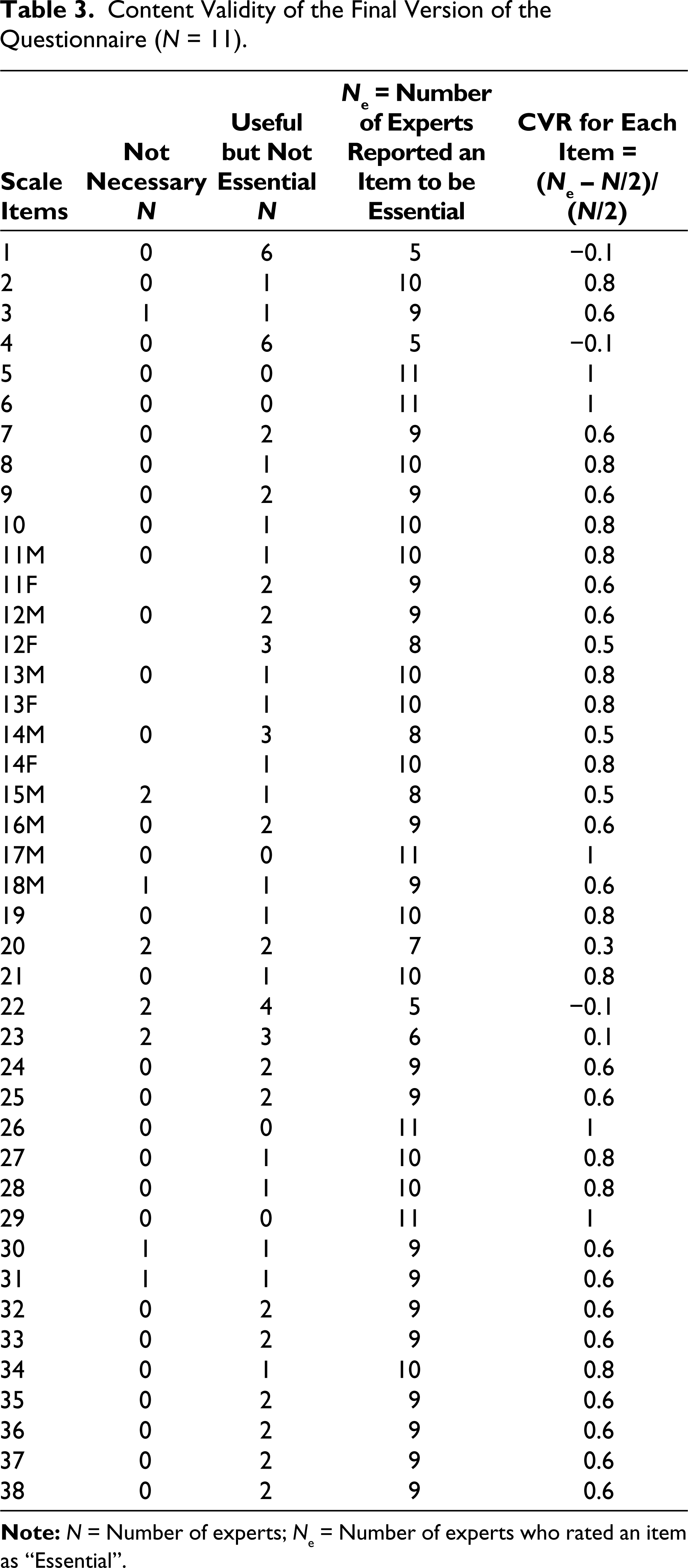
For the content validity, the scale was given to 11 psychiatrists with some interest in the area of sexual medicine. They were asked to rate each item as not necessary, useful but not essential and essential. Majority of the items were considered essential by at least seven out of the 11 experts. Further, none of the items was considered unnecessary by more than two psychiatrists. As per the Lawshe table for 11 experts, a minimum value of 0.59 is considered to indicate the essentiality of the item. 2 When we used this cut-off, six items had a value less than the cut-off (Table 3). Two items (item number 12 for the female version and item number 14 for the male version) had values less than 0.59; however, these were not consistent across both genders. The psychiatrists provided further suggestions regarding the language, and these changes were incorporated after being reviewed in a focused group discussion.
Content Validity of the Final Version of the Questionnaire (N = 11).
Discussion
In the present study, we attempted to develop a sexual dysfunction evaluation scale (SDES). We developed a new scale for multiple reasons. First, there are very few scales developed for the assessment of sexual issues in the Indian context.3–8 Furthermore, although some of the scales have been translated into various Indian languages, these translations have not been formally validated in the Indian context. An essential aspect of the assessment of sexual issues is the language barrier. Hence, keeping this in mind, we felt that the language of some of the available scales is complex for patients in the Indian context to understand. Another issue is the response options. The available scales often do not provide any specific kind of quantification for the persons responding to these scales, and it is left to their own interpretation of the responses. For example, while responding to an item with response options of “occasionally” and “sometimes,” the interpretation is left to the subject. This leads to considerable subjective interpretation and may potentially influence the findings. Scales assessing sexual dysfunction often do not take into account contextual factors, such as the type of sexual activity, including the availability of opportunity for being intimate, or the place where the consumer tries to be intimate. These factors are known to influence sexual functioning. Hence, understanding the sexual dysfunction, without understanding these factors, can lead to overdiagnosis of sexual dysfunction and can contribute to ignoring the core issues that may require attention while planning and carrying out interventions. It is often seen that clinicians managing patients with various illnesses often fail to assess sexual dysfunction as part of the ongoing illness and do not assess sexual dysfunction regularly as part of the side effects of the prescribed medications. The available scales also do not evaluate the attitude of the clinicians managing the patients for various ailments about the sexual dysfunction, and also the attitude of the patients about the medications, if these lead to sexual dysfunction. Considering all the above issues, we designed this scale, which comprises 34 items for females and 38 items for males.
We followed multiple steps during the development of the scale. These included a focused group discussion, review of available scales, and drafting the scale items. Different authors have suggested various steps to follow when constructing a rating scale. The first step that is usually proposed includes generating scale items and evaluating content validity. The second step involves identifying domains, pre-testing the questions/items, administering the survey, reducing the number of items based on the findings, and carrying out a factor analysis to understand the various factors or dimensions. Finally, the number of factors/dimensions and their reliability and validity are tested. 9
For this scale, we followed all the requirements outlined in the first step of scale development. Furthermore, for the generation of scale items, either a deductive approach (involving a review of the literature and assessment of available scales) or an inductive approach (involving focused group discussions and interviews) can be employed. For this scale, we followed a combination of both methods. For the items for which available scales had similar items, we reviewed them. For the items not covered by existing scales, we conducted a focus group discussion to develop the items. Although we initially framed the items in English, we followed the World Health Organization methodology to translate these items into Hindi. 10 Once these items were translated, the language was reviewed for simplicity, and further changes were made in the Hindi version to refine it even further. Based on these, further changes were made to the English version, and a back-translation was also performed for the Hindi version, which was then compared with the edited English version. These steps helped to simplify the language in both versions and ensured cross-language equivalence of the scale. We also made efforts to quantify the responses, wherever possible, to enhance the participants’ understanding while responding.
Once the initial scale was available, it was sent to 16 mental health professionals for initial subjective content validity and further suggestions. This step helped further refine the scale and its development. During this step, the majority of the participants reported that the scale would be useful to a large extent or very useful for clinicians for the assessment of sexual dysfunction and useful for the patients to report their sexual symptoms. In terms of coverage, all participants reported that the coverage of the scale was good or very good. However, half of the participants considered the scale to be lengthy. In terms of the language used on the scale, all participants reported it to be “average or simple.” Some suggestions were also made at this stage for the inclusion and exclusion of certain items and the refinement of language. This step helped refine the scale further before we proceeded to formally assess content validity and face validity quantitatively. This led to the development of a scale with 38 items for males and 34 items for females. At this stage, we did not remove any of the items, despite some participants reporting the scale to be lengthy, as we thought that the items could be removed at a later stage if required, based on the face and content validity and the application of scales to actual patients.
In the next step, we evaluated content validity and attempted to assess face validity using a quantitative method. For face validity, the scale was given to 20 sexually active persons to rate each item on a five-point scale as recommended. 11 At this stage, except for two items, all other items were rated as “important or very important” by 75% or more participants. The individual IIS for each item was more than 1.5, which is a recommended cut-off for retaining an item in the scale. These findings suggest that all the items of the scale have good face validity. The content validity of the scale was evaluated by requesting 11 psychiatrists with some interest in the area of sexual medicine. Out of the total items, a majority of the items were considered essential by at least seven out of the 11 psychiatrists. When evaluating the content validity of the scale, except for eight items, all other items were considered to have adequate CVR, as suggested by Lawshe’s table. 2 Based on the available findings, the scale developed has adequate face and content validity. However, administering the scale to the patients will help further reduce the number of items identified across various dimensions and factors of the scale. Accordingly, in the next step, we need to apply the scale to the patient group and attempt to refine the scale’s length.
It is essential to note the limitations of the present study. In this study, we only completed the first step of scale development. For initial face validity, we consulted with mental health professionals. This step could alternatively have involved the patients. Future studies should involve further validation of the scale, including testing its reliability, factor structure, and the development of cut-offs.
To conclude, the present study has led to the development of a scale with 38 items for males and 34 items for females to assess various aspects of sexual dysfunction. Compared to many of the existing scales, this scale has a broader scope and hopefully will improve the assessment of sexual dysfunction and also improve the management of sexual dysfunction.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.