
Abstract

Introduction
Anorgasmia (AO), or orgasmic dysfunction, is a form of male sexual dysfunction characterized by the absence of or significant reduction in orgasmic sensation.1–3 According to the International Society for Sexual Medicine (ISSM), anorgasmic ejaculation is defined as the perceived absence of orgasm despite the presence of ejaculation. 3 It can be classified as primary (lifelong) or secondary, the latter occurring after a period of normal sexual function. 3
Prevalence data varies widely. In the Global Study of Sexual Attitudes and Behaviors (GSSAB), the estimated prevalence of male orgasmic difficulties was around 10%, with rates increasing significantly with age (with odds ratios reaching up to 7.7 in older men). 1 Although the European Male Aging Study (EMAS) reported self-reported orgasmic impairment in approximately 6% of men, the clinically diagnosed prevalence in Asia remains low (0.4%), likely reflecting cultural stigma, communication barriers, and reluctance to seek help for sexual health concerns, particularly in Southeast Asia.1,4
In primary care, sexual dysfunction, particularly anorgasmic ejaculation, often goes unrecognized due to limited physician training, with additional challenges posed by Malaysian cultural norms that hinder open discussion; yet its complex nature requires a multidisciplinary evaluation addressing psychosocial, relational, medical, and lifestyle factors, as it can cause a significant impact on quality of life and intimate relationships.3,5
This case underscores a delayed presentation of anorgasmic ejaculation in a Malaysian male, highlighting the nuanced diagnostic and management role of primary care in addressing under-recognized aspects of male sexual health through a holistic approach.
Case Presentation
A 61-year-old male has experienced absent orgasmic sensation despite preserved ejaculation for two years, but only sought help in primary care two months ago due to personal discomfort and cultural stigma. He fathered six children in his first marriage and had no prior sexual dysfunction. After separating, he remained sexually inactive for approximately 20 years before beginning a new relationship with his current 42-year-old partner two years ago.
The patient described ejaculating without the accompanying sensation of orgasm, which significantly reduces his sexual satisfaction. He has normal morning erections, preserved libido, and satisfactory foreplay, with sexual activity lasting about 15 minutes once weekly.
In his clinical background, his comorbidities are well controlled: stable chronic hepatitis B, dyslipidemia, gout, pre-diabetes, and mild benign prostate enlargement. He is on one tablet daily of the following: Metformin XR 500 mg, Allopurinol 300 mg, Rosuvastatin 10 mg, Tadalafil 5 mg, Entecavir 0.5 mg, Coenzyme Q10, and glucosamine/chondroitin.
However, he had major depressive disorder (MDD) with anxiety during his first marriage, in remission without treatment. He exhibits performance-related anxiety in satisfying his current partner.
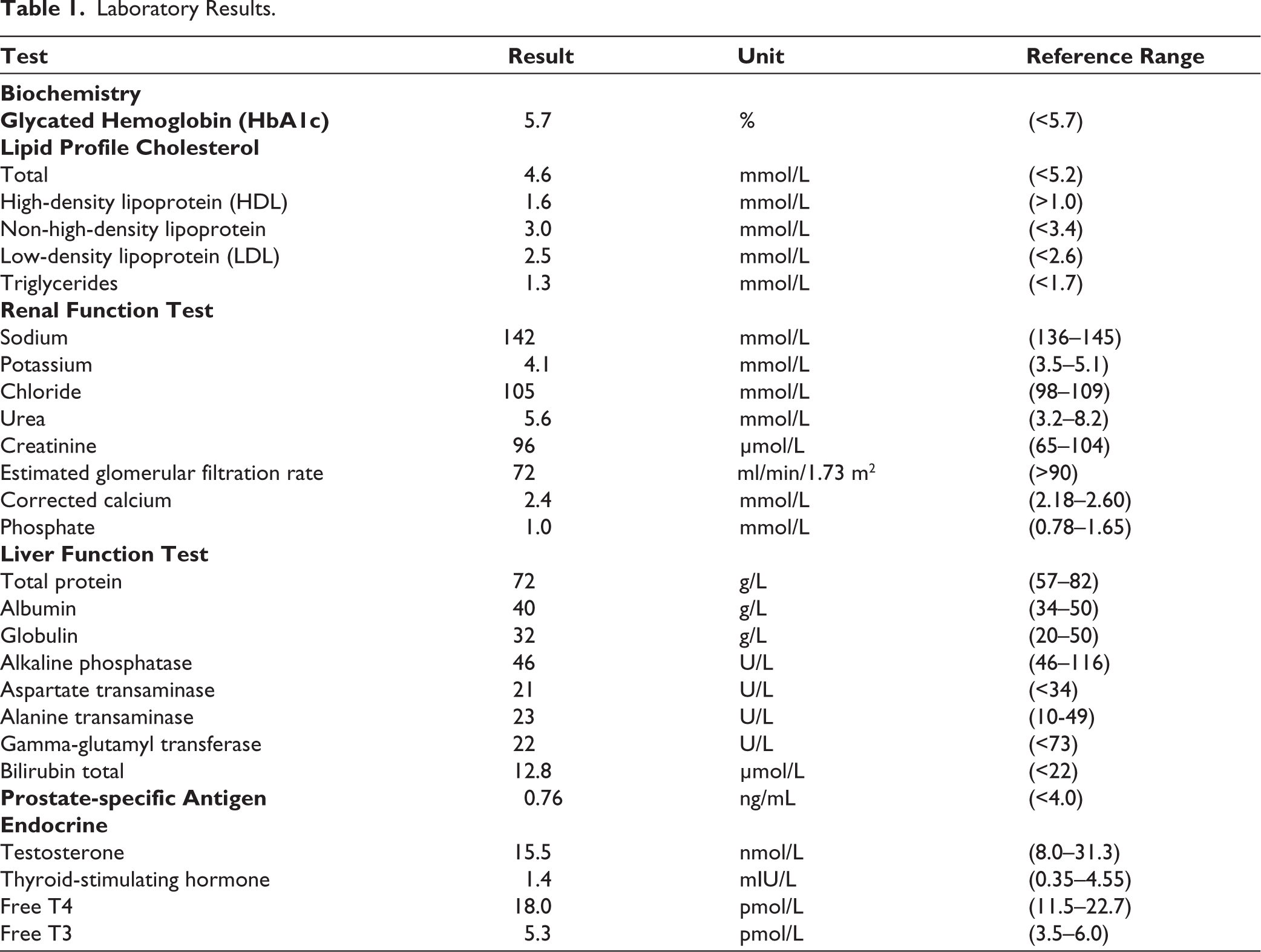
Mental state examination showed no major psychopathology, aside from mild anxiety and thought content focused on performance expectations. The Brief Sexual Performance Anxiety Scale (BSPAS) indicated moderate to high anxiety, particularly regarding fear of inadequate performance, partner dissatisfaction, and unpredictability of sexual function. Focused neurological, genitourinary, and systemic exams were unremarkable. Laboratory investigations, including serum testosterone, thyroid function tests, and metabolic profile, were all within normal limits (Table 1).
Laboratory Results.
Management included psychoeducation, cognitive behavioral therapy (CBT), and relaxation techniques targeting cognitive distortions around performance expectations. He is currently showing gradual improvement, reporting partial return of orgasmic sensation.
Discussion
In this patient, the normal sexual function during his previous marriage and the emergence of anorgasmic ejaculation only after initiating a new relationship support the diagnosis of secondary anorgasmia.2,3 The etiologies are often multifactorial: psychogenic, organic (neurologic, endocrine, vascular), medication-induced, or genitourinary pathology.1–3,6,7 In this patient, extensive evaluation revealed no organic cause, and none of his medications are commonly implicated in orgasmic failure as per published reviews.8–12 Instead, the clinical context, reinitiation of sexual activity, performance-related anxiety, and desire to satisfy the partner point toward a psychogenic origin.
Psychogenic anorgasmia requires empathetic, multidisciplinary care supported by thorough sexual, psychological, and relational assessment.3,5,13 Therefore, in this patient, the BSPAS findings highlighting moderate to high anxiety related to perceived performance inadequacy, partner dissatisfaction, and unpredictability helped pinpoint key cognitive distortions, guiding targeted psychotherapeutic intervention. 14
In many parts of Malaysia, limited training and access to sexual health services pose challenges, but as shown in this case, with trained primary care physicians, psychosexual issues like anorgasmia can initially be managed at the primary care level. However, it is often underdiagnosed in primary care, as physicians tend to prioritize physical comorbidities and rarely screen for sexual health. 4 Cultural taboos, conservative values, and patient reluctance to discuss sexual concerns further hinder timely recognition, as seen in our patient who delayed disclosure for two years. This challenge is compounded by the lack of training, robust evidence, screening tools, and standardized treatment protocols, limiting effective management in primary care. 3
Treatment includes psychosexual education, CBT, relaxation techniques, sensate focus, and partner involvement, with this patient showing gradual partial improvement through CBT and breathing exercises.3,7 The next step includes sensate focus and partner involvement, with pharmacotherapy—such as selective serotonin reuptake inhibitors (SSRIs) or cabergoline—considered if his progress remains insufficient.3,13,15
A holistic, patient-centered approach is vital. Primary care physicians should routinely normalize sexual health discussions. In resource-limited settings, integrating sexual health into existing clinics or setting up dedicated men’s health services, alongside improving physicians’ training, can support earlier detection and better outcomes.
Conclusion
This case highlights the need for primary care to routinely screen for sexual dysfunction, normalize sexual health conversations, and strengthen services through targeted training and integrated men’s health clinics.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient provided written informed consent for the publication of this case report, including all relevant clinical information and anonymized details.