
Abstract
Background:
Masturbation is a common and normal sexual behavior, also observed among children. Despite its benign nature, childhood masturbation (CM) often causes parental concern. However, literature on CM from South Asia remains scarce.
Objectives:
We aimed to see the available clinical evidence on CM in South Asia, considering clinical presentation, diagnosis, and management.
Methods:
This narrative review was conducted through comprehensive searches of PubMed, Scopus, Google Scholar, and Google without time restrictions, using both Medical Subject Headings and free-text terms. Eligible studies included original articles, case series, and case reports involving CM from South Asian countries.
Results:
Eighteen studies (2006–2025) comprising 148 children were included, mostly from India (n = 11). Case reports (n = 10) and case series (n = 5) predominated. Ages ranged from 4 months to 7 years, with a female predominance (62.2%). Common presentations were rhythmic body movements, leg crossing, facial flushing, grunting, sweating, and seizure-like episodes. Pediatricians were consulted as the first level carer in most of the cases, and laboratory tests were usually normal. Non-pharmacological interventions, behavior therapy, psychoeducation, and parental counseling were frequently used (n = 16) and found effective.
Conclusions:
CM in South Asia is a relatively less-reported clinical entity. Increasing awareness, promoting culturally sensitive interventions, and prioritizing non-pharmacological management can improve the status quo. Future research should move beyond case reports toward population-based studies that explore the prevalence and psychosocial impacts of CM in South Asia.
Keywords
Introduction
Masturbation is a common and normal sexual behavior that occurs in 90%–94% of males and 50%–60% of females in their lifetime. 1 This sexual behavior can also be seen in children2–6 which is also referred to as gratification disorder or infantile masturbation, and it first came to light in 1909.2,7 Although it is considered benign, its presentation often causes significant concern among parents.3,4 Childhood masturbation (CM) is usually characterized by self-stimulation of the genitalia with unusual posture and movement, and in most cases, there is an absence of direct hand stimulation of the genitalia, which makes diagnosis difficult.8,9 Clinical features of CM, such as rhythmic movements, facial flushing, grunting, posturing, and behavioral alterations, can resemble seizures, abdominal pain, or urinary tract infections, and may cause diagnostic challenges.9–11 It has been reported as early as 2 months of age, with peak occurrence at 4 years and adolescence.2,12
This is an important health issue for infants; however, medical literature remains underreported in South Asia (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka), which share certain overlapping socio-cultural and historical contexts relevant to sexual health.13,14 As a result, parents of the children develop anxiety or shame, or they even punish their children in response.15,16 Families may seek medical advice under the presumption that the child is suffering from a pathological condition, and when doctors inform them about the disease and suggest non-pharmacological treatment, they sometimes do not want to accept the diagnosis or the treatment. 16
Most of the literature about CM in South Asia is confined to case reports, case series with small sample sizes, or isolated clinical observations published in national or regional journals. These studies provided important information about how CM manifests in South Asia. In addition to that, qualitative studies have documented parental interpretations, physician responses, and socio-cultural factors shaping help-seeking patterns. For example, research from India and Pakistan has shown that healthcare consultations for CM are often delayed due to parental fear of stigma, reliance on informal advice networks, and misconceptions about sexual behavior in children. 17 However, no systematic attempt has yet been made to synthesize this evidence across countries and over time, making it difficult to draw relevant conclusions or develop appropriate clinical guidelines for South Asian countries. The region represents a unique socio-cultural and sexual health context in which childhood sexual behaviors are often interpreted through moral, religious, or honor-based frameworks rather than developmental science. This frequently leads to underreporting, misinterpretation as pathology, and delays in seeking or accepting appropriate medical advice. 17 The region is also characterized by limited sexuality education, strong intergenerational authority structures, and a healthcare environment where physicians may have variable training in pediatric sexual health, all of which influence the clinical approach to CM. 18 In this backdrop, a focused review was necessary not only to collate the evidence but also to inform culturally sensitive clinical interventions, improve physician-parent communication, and guide public health messaging. This review therefore, aims to provide a comprehensive synthesis of available evidence on CM in South Asia.
Methods
Search Strategy
A comprehensive web-based search was conducted without any time restrictions on publication date. The search was performed in PubMed, Scopus, Google Scholar, and Google using both Medical Subject Headings and free-text terms to ensure sensitivity and relevance on August 2, 2025. Boolean operators were applied to formulate the search string:
(“CM” OR “infantile masturbation” OR “genital self-stimulation in children” OR “masturbation in children” OR “gratification disorder”) AND (“South Asia” OR “Afghanistan” OR “Bangladesh” OR “Bhutan” OR “India” OR “Maldives” OR “Nepal” OR “Pakistan” OR “Sri Lanka”)
Inclusion Criteria
Research articles eligible for inclusion were original studies, quantitative analyses, case reports, and case series available in full-text form. Only peer-reviewed articles published in English were included. The study was included if it focused on CM, infantile masturbation, gratification disorder, or genital self-stimulatory behaviors in children aged from 1 month to 10 years that occurred in eight South Asian countries: Afghanistan, Bangladesh, Bhutan, India, the Maldives, Nepal, Pakistan, and Sri Lanka, without any consideration of the basis of diagnostic tools/criteria.
The below 10-year age group was selected because most developmental frameworks and international child health definitions classify “childhood” as extending from birth until 10 years, after which the pubertal transition and early adolescence begin. 19 This age bracket also captures the period when CM is most frequently reported in pediatric and psychiatric literature.
Exclusion Criteria
Studies were excluded if they were review articles, editorials, opinion pieces, qualitative studies, multiple reports published from the same data, or reports based solely on media coverage. In addition, studies on migrant populations residing outside the South Asian region were excluded to ensure geographic specificity. Duplicate records were removed, and all retrieved studies were manually screened for relevance based on titles, abstracts, and full texts.
Outcome Variables
From each included study, the following variables were extracted:
Study, publication year, country, study design, setting, sample size, age, sex distribution, first consulted physician, investigations performed, treatment options, and key findings. All extracted data were analyzed descriptively using Microsoft Excel for Windows, version 2011.
Analysis
This work was conducted as a narrative review, allowing for a descriptive synthesis of published evidence without performing formal meta-analytic statistical pooling. Such an approach is appropriate for collating data from heterogeneous case reports, case series, and small observational studies where standardized effect sizes are unavailable.
Results
Study Characteristics
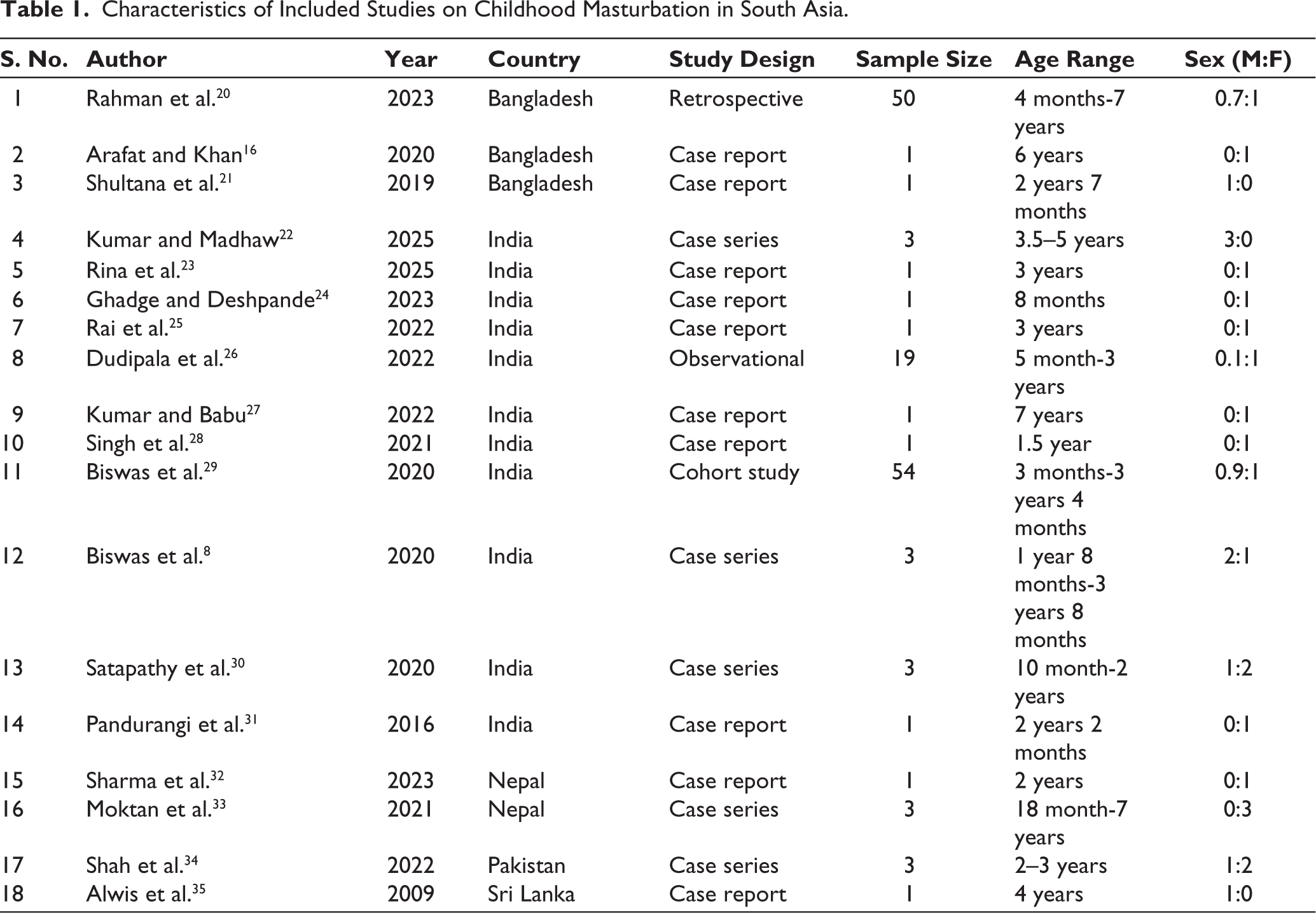
A total of 22 studies were assessed in full-text, of which four were excluded for not meeting the inclusion criteria. Final, 18 studies were included in this review8,16,20–35 from five different South Asian countries (Table 1). There were 11 studies from India, three studies from Bangladesh, two studies from Nepal, and one study from Pakistan and Sri Lanka each. The studies were published between 2006 and 2025, with a marked clustering of publications after 2019, suggesting a recent increase in academic recognition of this topic in the region. The majority of included studies were case reports (n = 10) and case series (n = 5), and the remaining three were original articles. All the studies were conducted among clinical samples.
Characteristics of Included Studies on Childhood Masturbation in South Asia.
Sample Profile
After analyzing data from 18 studies, we found 148 children who showed masturbation or genital self-stimulatory behaviors. Sample sizes varied widely, ranging from single-child case reports to studies involving up to 54 participants. The age range of the children was from 4 months to 7 years, with reported cases (over two-thirds) being below 5 years of age. Among the studies, female predominance was seen, 92 females (62.2%) and 56 males (37.8%).
Clinical Presentation, First Consultation, and Diagnostic Evaluation
Children most commonly present with rhythmic body movements, grunting, facial flushing, distant facial expression, excessive sweating, and seizure-like activity. Posturing patterns such as leg crossing or scissoring, pelvic rocking, or prone positioning were frequently described, often in combination with autonomic signs including flushing and tachypnea. These variable clinical symptoms created challenges and often led to a longer time to reach diagnoses. Notably, some children were initially treated for epilepsy, scabies, worms, or abdominal pain before arriving at a diagnosis of gratification behavior (Table 2).20–24
Clinical Presentation, Diagnostic Evaluation, and Treatment Approaches of Childhood Masturbation Cases in South Asia.
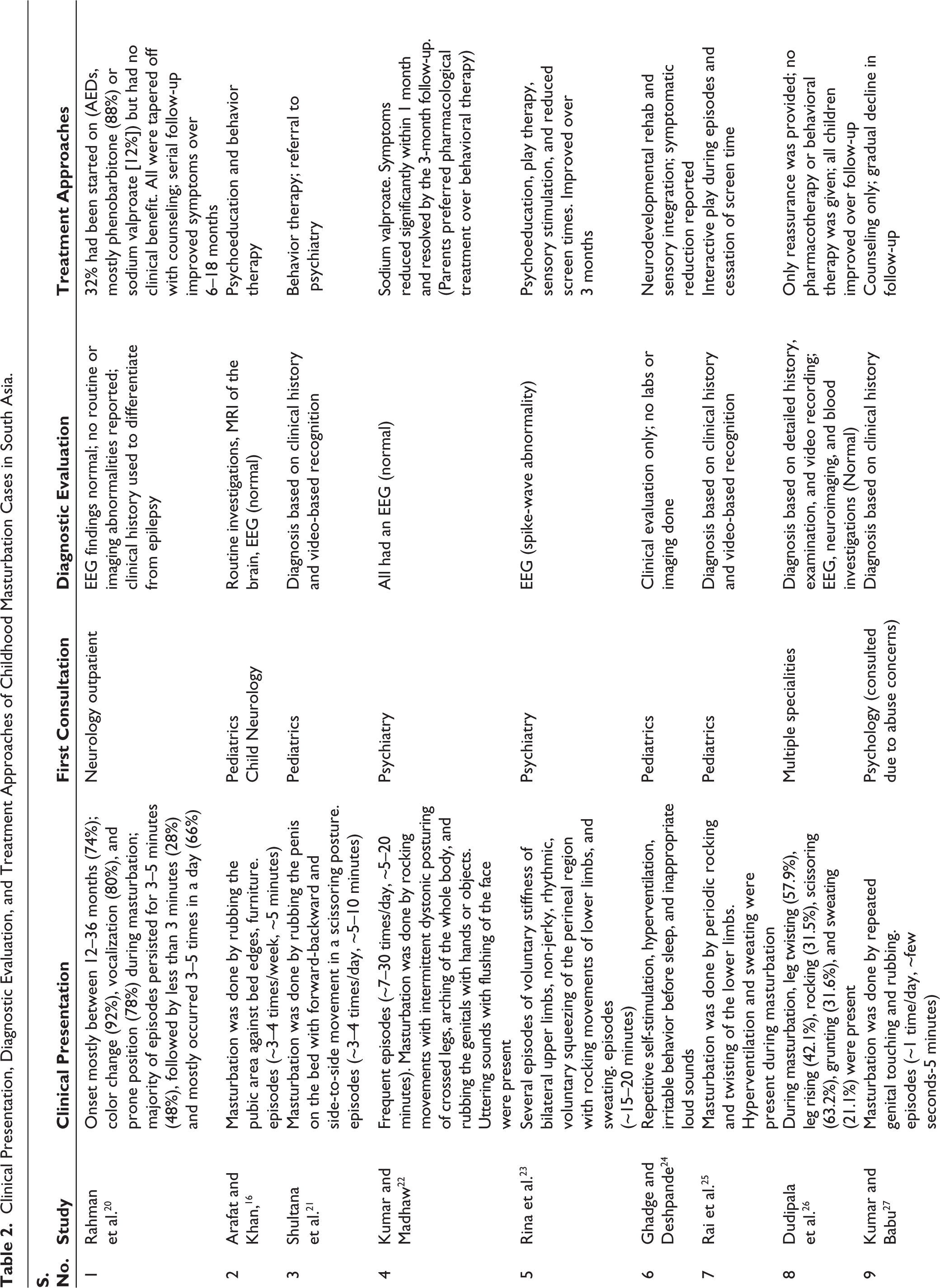
In most of the cases, the first point of medical contact was a pediatrician (n = 13), though referrals to psychiatrists, dermatologists, and other physicians were also reported in some cases. In a minority of cases, the first point of medical contact was made to specialists due to concerns of possible sexual abuse, reflecting another dimension of parental anxiety in such presentations. The diverse presentation and lack of awareness delayed the diagnosis and treatment process.
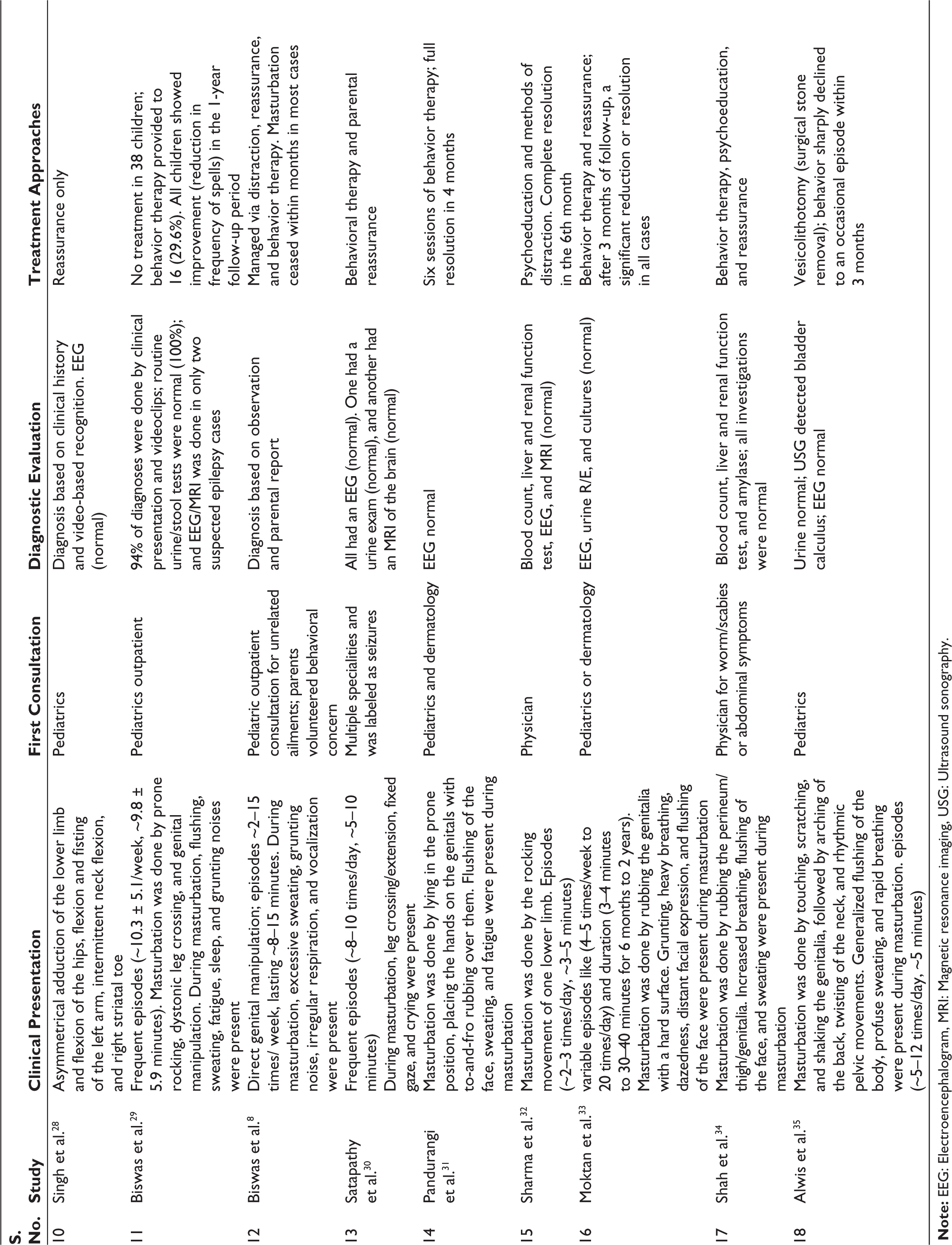
Most cases were diagnosed based on a detailed history, examination, and video recording. Various investigations were also done, including electroencephalograms (EEGs), which were reported in 12 studies and consistently found to be normal except in one case report. 25 Routine blood, urine, and stool examinations were also commonly conducted to exclude urinary tract infections or helminthic infestations, and found nothing contributory. Similarly, brain imaging, particularly magnetic resonance imaging (MRI), was selectively performed, but it revealed no abnormal findings in all cases.
Treatment Approaches
Multiple treatment approaches were noted. However, non-pharmacological interventions were most frequently advised (n = 16) and found effective. These included behavior therapy, psychoeducation, parental reassurance, and counseling, alongside other methods such as sensory integration therapy, play therapy, and distraction techniques. Follow-up data from multiple studies showed substantial to complete resolution of behaviors within 3–6 months in most cases, underscoring the benign and self-limiting nature of the condition when appropriately managed.
Pharmacological treatment (anti-epileptic drugs [AEDs]) was documented in one study where all three of the study subjects showed rapid improvement, and most of them were completely free from gratification disorder after 3 months of follow-up. 26 Since misdiagnosis is common in this phenomenon, in some cases (n = 4), children were already receiving AEDs such as sodium valproate or levetiracetam, but their condition did not improve, and the doctor advised them to use non-pharmacological interventions, and they also tapered down the AEDs.20,30,32
A rare surgical intervention was reported in one study, conducted in Sri Lanka, where the child was showing masturbation behavior secondary to a bladder stone that was resolved completely following vesicolithotomy. 35
Discussion
Major Findings of the Review
This review analyzes published articles on CM in South Asia in the last two decades, and the findings reveal that it causes diagnostic dilemma and parental distress in South Asia. Our synthesis shows a recent rise in publications after 2019, but overall reporting remains sparse, suggesting that CM remains a clinically under-recognized. One of the challenges is that the diagnosis is made after exclusion. Another challenge is the availability of video recording, which is invaluable in the diagnosis.
Despite the growing number of studies about CM in South Asia, which has been increasing since 2019, the total number of published reports remains low. The majority of studies found were case reports or case series from India8,22–25,27–31 and Bangladesh,16,21 with a smaller representation from Nepal,32,33 Pakistan, 43 and Sri Lanka. 35 No study was identified from Afghanistan, Bhutan, or the Maldives. This geographic gap likely reflects underreporting due to sociocultural stigma, absence of formal sexuality education, and healthcare system limitations, consistent with patterns seen in other sexual health research from South Asia. 36
Clinical Profile and Diagnostic Challenges
There were various types of clinical presentation of CM were found, but typically included rhythmic body movements, facial flushing, grunting, and sweating, often mistaken for neurological or gastrointestinal conditions. Distinctive posturing, such as leg crossing or scissoring, prone rocking, or pelvic thrusting, was commonly observed, sometimes with autonomic signs including tachypnea and hyperhidrosis. Many children in these studies were initially labeled with epilepsy,20,30,32 abdominal pathology, or parasitic infections 34 and were treated with anti-epileptic drugs, anti-parasitic drugs, or antibiotics. Such labeling delays proper psychosocial interventions and increases the suffering of the children and their parents. Not only in South Asia, but also in other countries on different continents, CM are mislabelled, and that leads to the use of antiepileptic drugs and delayed treatment. 37
In several cases, the diagnosis was established after video recordings provided by parents by which doctors were able to assess detailed behavioral changes of the child during the episode. This finding shows the importance of video documentation in suspected CM cases because these diagnostic methods were also seen in case reports of CM from all over the world.38–40
Sex Distribution and Age Patterns
In adolescents and adults, lifetime masturbation prevalence is 90%–94% in males and 50%–60% in females. However, CM reports show a consistent female predominance, with studies from outside South Asia reporting 72.4% 41 and 68% 42 female cases. Our review similarly found 62.2% of cases to be female, which may reflect a true sex difference in presentation or cultural and reporting biases, such as heightened parental concern for perceived “inappropriate” behaviors in girls. The majority of cases occurred in children under five, consistent with global literature.5,41 One study even documented intrauterine self-stimulatory behaviors, 43 underscoring the developmental origins of such activity.
Parental Reactions and Cultural Context
Discussions of childhood sexuality remain taboo, and masturbation is often considered shameful or morally unacceptable. Such stigma can lead to delayed help-seeking, concealment of behaviors, and reluctance to accept non-pharmacological management. These barriers are not confined to the region; British South Asian communities, for example, also show reluctance to disclose sexual matters due to cultural taboos. 44 In some cases, parents actively resisted a CM diagnosis and behavioral therapy, instead requesting medication. 22 These findings highlight the need for culturally sensitive psychoeducation to build parental trust and adherence.
Diagnostic Workup and Avoidable Investigations
Most children underwent EEG, MRI, and routine laboratory tests, all normal except for one EEG abnormality. 23 This reinforces that CM is a diagnosis made clinically, and excessive investigations can be avoided unless history or examination suggests organic pathology. Similar conclusions have been drawn in international literature.6,9,12
Management and Outcomes
Non-pharmacological interventions, behavior therapy, psychoeducation, parental counseling, and reassurance were the mainstay and led to improvement in 3–6 months in most cases. These approaches also help normalize developmental sexual behaviors and reduce parental anxiety. Pharmacological treatment was rare, except when misdiagnosis led to antiepileptic use or when parents specifically requested medication. 22 The single surgical case 35 was directed at an underlying bladder stone rather than CM itself, reminding clinicians to exclude organic causes when presentation is atypical.
Implications for Practice and Policy
Greater awareness among pediatricians, psychiatrists, and primary care physicians could improve diagnostic accuracy and reduce unnecessary interventions. Multidisciplinary collaboration and the inclusion of CM in pediatric sexual health training are recommended. Public health messaging on normal childhood sexual development, tailored to cultural contexts, could reduce stigma, and encourage early consultation. Future research should include larger, prospective studies to assess cultural determinants of parental responses and the long-term psychosocial impact of CM. Some recommendations are made in Box 1).
Key Recommendations for Clinical Practice and Policy in South Asia.
Early recognition and diagnosis
Include CM in pediatric and psychiatric training curricula. Promote the use of parental video documentation to differentiate CM from pathological conditions.
Minimizing unnecessary investigations
Base diagnosis primarily on history and examination; reserve EEG, MRI, and lab tests for atypical presentations or when organic pathology is suspected.
Culturally sensitive psychoeducation
Provide parents with non-judgmental, evidence-based explanations of CM as a benign developmental behavior. Address cultural stigma and misconceptions proactively during consultations.
Appropriate management
Prioritize non-pharmacological interventions such as behavior therapy, parental counseling, reassurance, and distraction techniques. Avoid pharmacological treatment unless required for comorbid conditions or in rare, justified cases.
Public health and policy initiatives
Integrate childhood sexual development topics into community health education programs. Develop culturally adapted informational materials in local languages to improve parental awareness and reduce stigma.
Research priorities
Conduct larger, multicenter studies to better understand the epidemiology, cultural determinants, and long-term outcomes of CM in South Asia. Investigate gender-related reporting patterns and their sociocultural underpinnings.
Strengths and Limitations
To the best of our knowledge, this is the first review on CM in South Asia providing a temporal perspective on evolving clinical awareness and diagnostic practices. However, limitations should be acknowledged. First, the majority of the studies were case reports and case series that be a source of bias when generalizing the study findings. Second, sample sizes were small, which may restrict the generalization of findings. Third, the sociocultural diversity across South Asian countries means that findings from this review may not apply universally. Fourthly, although we made an extensive search, due to the search terms, some articles may be excluded. Fifth, studies published in printed-only journals published before 2016 could be excluded from featuring in the search. Sixth, we included all articles on CM without considering the measuring tools and diagnostic criteria, which may be a source of potential biases because children may produce masturbation-like behaviors for various reasons.
Conclusion
CM is a normal developmental behavior in infants and children, yet it remains underreported due to cultural stigma and limited clinical awareness. This review underscores the need for increased recognition, culturally sensitive psychoeducation, and standardized diagnostic practices to avoid misdiagnosis and unnecessary interventions. Emphasis should be placed on non-pharmacological management strategies, which effectively reduce both the child’s symptoms and parental anxiety. Future research should move beyond isolated case reports toward well-designed, population-based, and multicenter studies that examine the prevalence, cultural determinants, and psychosocial impacts of CM in South Asia.
Footnotes
Authors’ Contribution
SM Yasir Arafat: Conception.
Sadeed Hossain: Data curation.
All authors: Writing original draft.
All authors: Writing review and editing.
All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study used data from publicly available published academic literature. No human participants were directly involved in this study. Therefore, no formal ethical clearance was sought for conducting the review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.