
Abstract
Objective:
Women aged 40–65 years, who undergo predictable and important physiological transitions, feel that access in England to Women’s Health and Wellbeing Services (WHWS) is poor and inequitable. The barriers and enablers to WHWS, focusing on sexual health and sexual wellbeing services, for women aged 40–65 years, and feasible suggestions for development, were explored from the perspective of 11 providers of health and social care.
Design:
A qualitative study, using semi-structured interviews, was conducted with providers of WHWS. Framework Analysis, applying the Socio-ecological Model (SEM), through an intersectionality lens, was employed to analyse the findings. The study was reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ).
Setting and Participants:
Eleven providers of care were recruited by convenience sampling from health and wellbeing settings serving the most under-resourced areas in South-East England.
Results:
The intersectional disadvantage of belonging to underserved groups overlapped across the constructs of the SEM. The main themes that emerged were the lack of prioritisation of midlife women within society, and the inadequate knowledge about the health and well-being requirements, including the sexual health and sexual well-being requirements, of midlife women.
Conclusion:
Amongst policy makers, the sensitive, complex, and interlinked nature of health and wellbeing, including sexual health and sexual wellbeing, of midlife women must be recognised. Investment in public and Health Care Professionals’ education, together with a life-course approach to health research and policy, is required to destigmatise and improve access to WHWS for midlife women.
Introduction
Midlife, defined as the period of life between 40 and 65 years, 1 can be viewed as an opportune time to improve the health and well-being trajectory of women. It includes the predictable, yet diverse, physiological and psychological changes associated with the late reproductive to late menopausal transition for women, 2 which often coincides with demanding caring responsibilities and career roles, together with shifts in relationships. 3 Midlife women in England do not have adequate or equitable access to Women’s Health and Wellbeing Services (WHWS),4,5 including sexual health and sexual wellbeing services, and those who live in underserved coastal communities are a poorly researched population with unfavourable health outcomes. 6 WHWS provide support for conditions that are unique to women, as well as conditions in which there are differences between men and women in risk, presentation, and response to treatment. 7 WHWS that are most relevant to midlife women, which require research, service, and policy investment, include: 8 sexual health services; sexual wellbeing services; preventative services (contraception, Human Papilloma Virus [HPV] screening, breast screening); and gynaecology services, including continence management and menopause treatment. 9 Evidence from high-income countries demonstrates disproportionately lower prescribing rates for Hormone Replacement Therapy (HRT) in deprived geographic areas, 10 rising rates of sexually transmitted infections (STIs) in older women in underserved areas,11–13 and poor access to care for urinary incontinence, particularly for older women in underserved areas.14,15
A range of interlinking factors affect adequate and equitable access to WHWS, including sexual health and sexual wellbeing services, for midlife women. 16 These include women’s knowledge about symptoms and services,16–29 their interpersonal skills, 30 competing priorities for their time, 31 stigma and community norms,32,33 and healthcare organisation resources and policies, 34 including a knowledgeable and skilled workforce. 35 Health care providers in WHWS, particularly sexual health and sexual wellbeing services, work with midlife women to address complex intimate issues and can offer a granular understanding of how to address the barriers to WHWS for midlife women. Many providers of WHWS in England have dual insights into the enablers and barriers to WHWS, as both professionals and midlife women. 36 The aims of this study were to explore the barriers and enablers to accessing WHWS, focusing on services for sexual health and sexual wellbeing, for midlife women from the perspective of providers of care in one region of the UK, and to project their suggestions to improve access to these services. This study was conducted in tandem with, and strengthens, a project which explored access to women’s health services from the perspective of women aged 40–65 years living in the same region. 37 The Socio-ecological Model (SEM), 38 which has successfully been deployed in women’s health and sexual health research to conceptualise the multiple, dynamic, and interconnecting physical, social, and political factors that influence access to health as affected by the interaction between the person and their environment,39–41 was chosen to categorise the data into the intra-personal, inter-personal, organisational, and public policy, enablers, and barriers to services, for midlife women. An intersectionality lens 42 was used to consider the different axes which may contribute to health inequalities 43 from the perspectives of providers of WHWS in one region of the UK, including sexual health and sexual wellbeing services.
Methods
Study Design
This was a qualitative study which used in-depth interviews informed by topic guides to produce a granular description of the enablers and barriers to WHWS, focusing on sexual health and sexual wellbeing services, for midlife women from the perspective of the providers of care in one region of the UK. It was reported in line with the Consolidated criteria for Reporting Qualitative research checklist (COREQ) 44 (Supplementary file 1). The SEM 38 and an intersectionality lens 42 were utilised to enable an appreciation of how systems of privilege at the macro social-structural level within healthcare research and health care services maintain health disparities. 45
Setting and Participants
WHWS in England, UK, that serve midlife women are mainly commissioned by local authorities, and provided by primary care and sexual Health Care Professionals (HCPs), who are able to refer patients to secondary care services. 46 This study was conducted in East Sussex, a region in the Southeast of England which has significant disparities in access to health care and health care outcomes for midlife women, with particular geographic areas experiencing high levels of deprivation. 47 The inclusion criteria were English-speaking primary and secondary care health and social care professionals, commissioners, community, and charity workers delivering, or signposting people who self-identified as women and trans-masculine or non-binary gendered individuals (TGNB), aged 40–65 years who lived in East Sussex, to WHWS.
Data Collection and Procedure
Convenience sampling 48 was employed. The sample size was determined by theoretical saturation- the point at which no new themes or concepts were likely to emerge related to the aims and objectives of the study, 49 and information power—the potential of the available empirical data to provide access to new knowledge by means of analysis and theoretical interpretations. 50 This resulted in the inclusion of 11 participants in this study. Providers were recruited using education sessions and posters in community health and wellbeing settings in the most underserved areas in East Sussex, defined as the lowest two deciles according to the English Indices of Multiple Deprivation (IMD). Participants were offered the choice between face-to-face or virtual interviews (via Microsoft Teams). Consented participants completed a brief socio-demographic form prior to the interview. A topic guide, co-produced with our Patient and Public Involvement, Engagement, and Participation (PPIEP) group, and based on the findings of previous work by our group, 16 enabled both systematic coverage of key topics and new themes to emerge. In-depth interviews were audio-recorded, and field notes were made. The first author (KS), with the assistance of Microsoft Teams transcription, transcribed verbatim; three authors (KS, DH, CL) independently cross-checked two transcripts for consensual validation. 51 Interviews were analysed iteratively, to enable sampling until theoretical saturation for breadth of data and information power for depth of data. Our PPIEP group, five midlife women from a range of different socio-economic backgrounds in East Sussex, supported the development of the objectives and the methodology. KS, who works as a sexual health/ HIV physician and a PhD researcher, and identifies as cis feminine, conducted the interviews. Regular consultations with the PPIEP group and the steering committee (KS, JH, DH, CL,SB, CI ), and ongoing documentation in field notes, maintained reflexivity. 52
Data Analyses
Three authors familiarised themselves with two datasets. They employed Microsoft Word tables to manage the data and independently identified emerging themes and sub-themes. Guided by the SEM, 53 employing an intersectionality lens, 42 they compared results for the purpose of structural corroboration, 54 and determined upon a coding framework in the form of a coding tree and a matrix. The Framework Analysis Approach, 55 through which recurrent and important themes are identified using an iterative process of coding themes and sub-themes, was employed in five stages: familiarisation, identifying themes, indexing, charting and summarising, interpretation and mapping. 55 The steering committee (KS, JH, DH, CL, SB, CI) compared the themes and sub-themes and the coding framework and agreed on the final analysis. Member checking, in which the matrix and analysis were discussed with one participant, and peer debriefing, which entailed the data and research process being reviewed by a researcher (CL) familiar with the research being explored and with expertise in qualitative research, enhanced accuracy, validity and credibility.
Ethical permission was granted by the Health Research Authority and Health and Care Research Wales Committee (Ref no: 24/EE/0032).
Results
Participant Characteristics
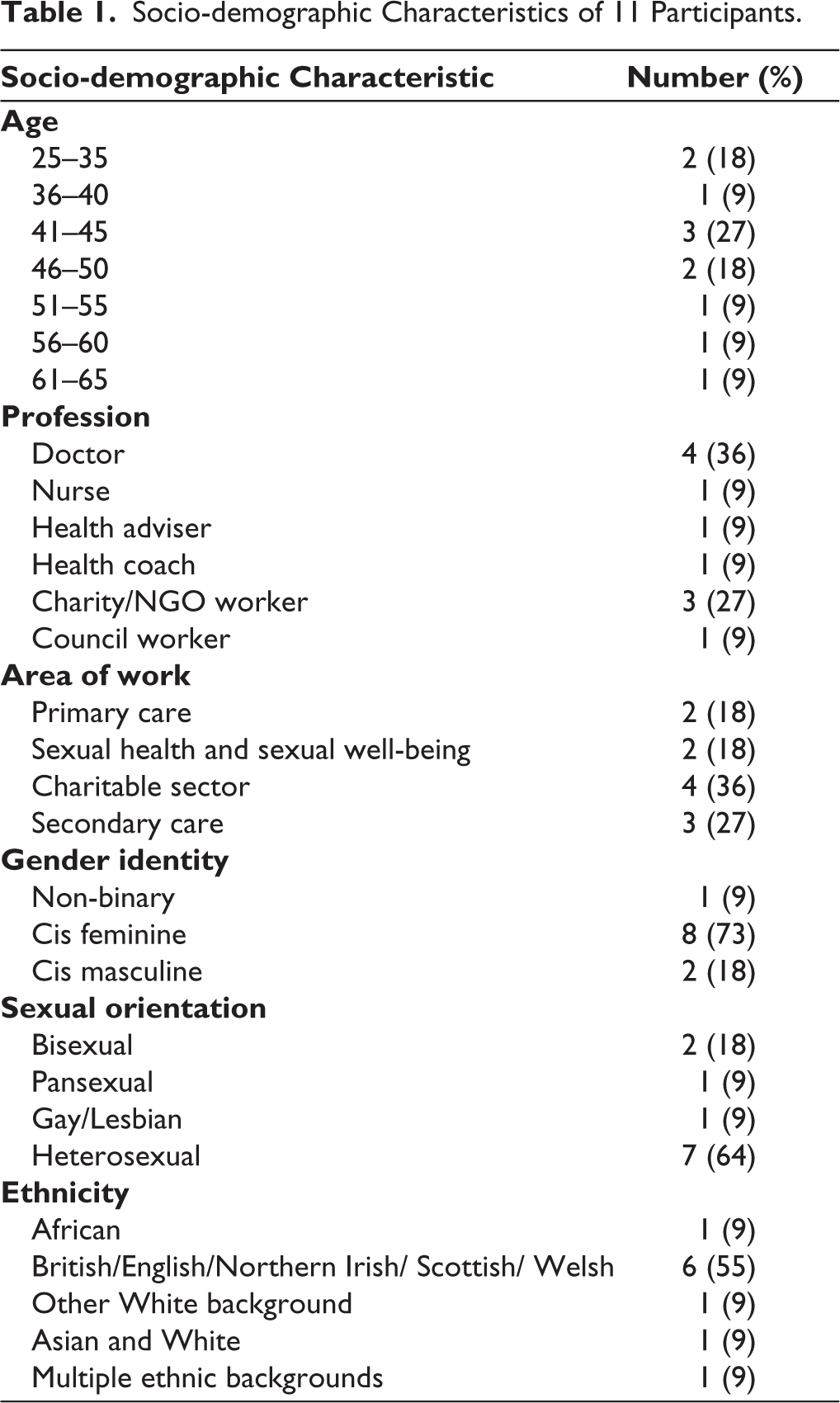
Interviews were conducted between March 2024 and June 2024. Eleven providers were recruited to the study, and there were no dropouts. Interviews lasted between 50 and 75 minutes. Providers worked in a variety of sectors and specialities (Table 1) and ranged in age from 25 years to 63 years. 8 (73%) of participants identified as cis feminine, and 6 (55%) of participants identified as cis feminine people aged between 40 and 65 years.
Socio-demographic Characteristics of 11 Participants.
Overview of Findings
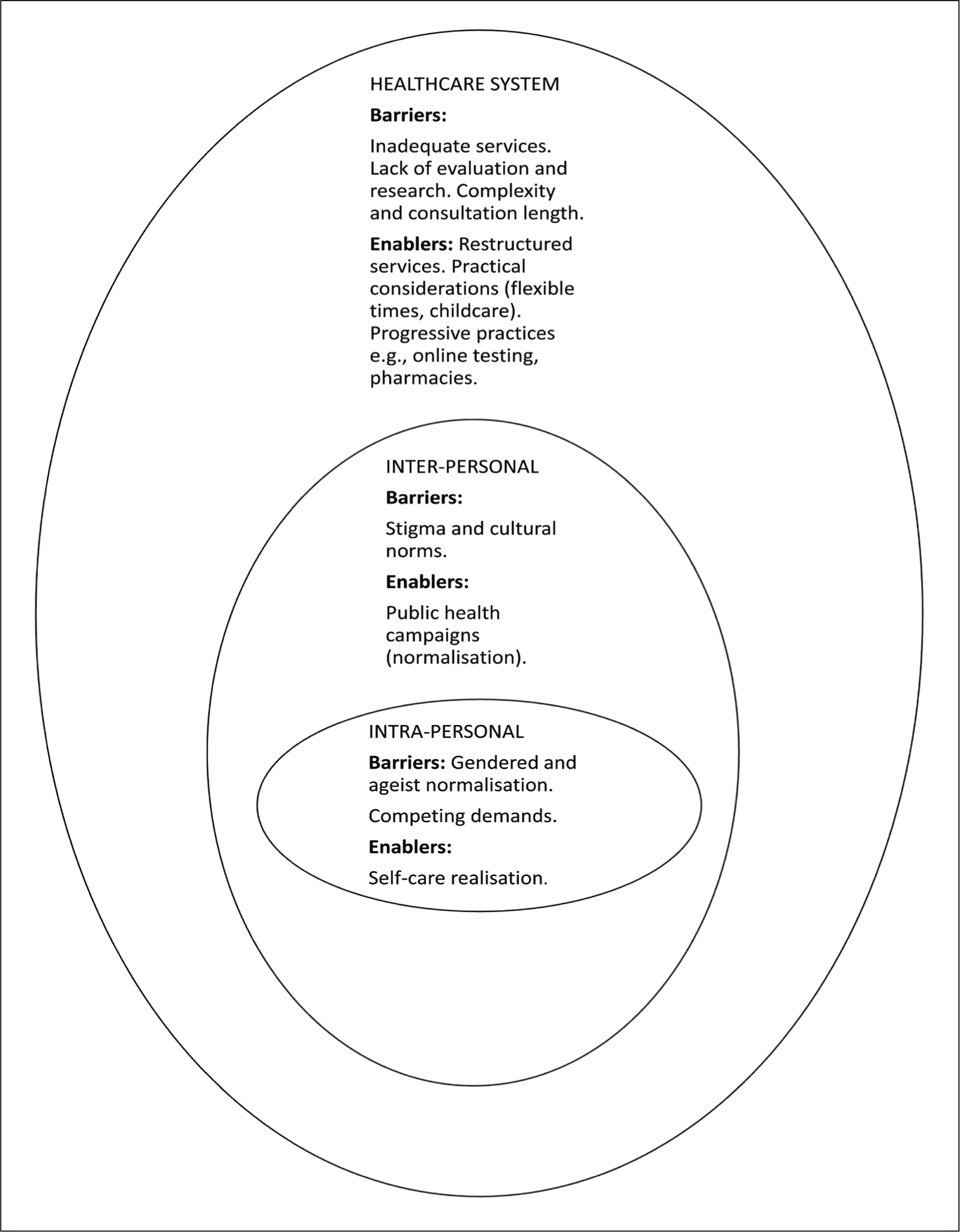
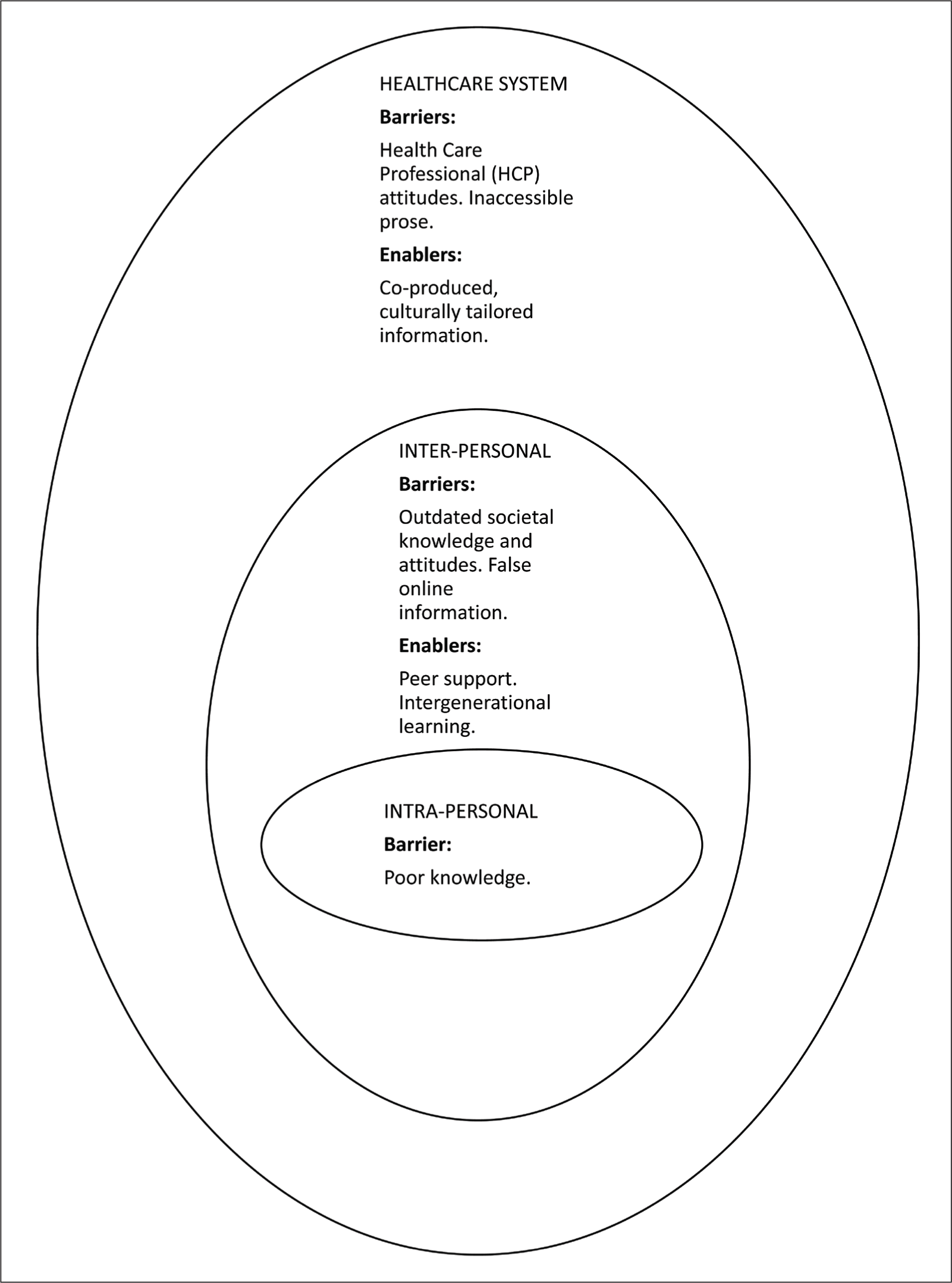
The data are presented within the two themes that have been identified: the insufficient prioritisation of midlife women in society, and the role of education around midlife women’s health and wellbeing (Figures 1 and 2). Each theme is separated into subheadings which fit under the inter-personal, intra-personal, organisational and public health policy constructs of the SEM. 38 Barriers and enablers for each theme are discussed in parallel, employing an intersectionality lens. Quotes are presented as supporting evidence, with the interview number cited. Strategies that are currently being considered by local authorities, including the development of regional ‘Women’s Health Hubs’, 56 as well as more innovative facilitators to access, such as the featuring of midlife women in STI self-testing public health messages, were suggested.
Cross-constructs Theme 1: The Prioritisation of Midlife Women
Intra-personal Construct
Gendered and Ageist Normalisation
Although a small number of providers had witnessed an awakened interest in self-care in many midlife women, most providers felt that women often diminished their own health and well-being problems (Figure 1). This had resulted in delays in women accessing care until the symptoms had a severe impact on their quality of life. Providers attributed this to culturally conditioned gendered stoicism and normalisation of symptoms that were related to ageing. The lack of feeling of entitlement to receive timely care was particularly apparent among women who lived in underserved areas.
People just say “Oh, it’s age. This (vaginal dryness) is natural.” Provider 2.
So, if they (women in under-served areas) are told that there’s a two year wait to see a (vulval) dermatologist, they just accept that. And they don’t keep re-presenting if they have ongoing issues. (They) just think that’s what I have to put up with. Provider 5.
Cross-construct Enablers and Barriers (Theme 1).
Competing Demands
Most providers recognised the impact of the multiple responsibilities that many midlife women carry, including careers, childcare, and elder care, on their time and (economic) resources to access WHWS, including sexual health and sexual wellbeing services. The possibility of attempting to remedy housing, food, money and other social problems at the same time and in the same location as healthcare was viewed as a rarely employed enabler to WHWS.
It’s not on people’s radar to go to a (cervical) screening appointment because they’re spending this time while the kids are at school to get some food for them. That’s the priority. Provider 9.
Their own needs come at the very bottom of the pile. Provider 5.
Inter-personal Construct
Instigation by (Male) Partners
Although inherently linked to their prioritisation of others, in this context, acting as an enabler to services, providers reported that the impetus for many midlife women to access WHWS in relation to sexual health challenges had been when their problem had affected their intimate relationships. Indeed, their help-seeking behaviour had sometimes been instigated by (male) partners.
It’s often the point at which it’s interfering with their relationship. That’s the real trigger for them going to seek help. (They) feel horrendously guilty, and they want to fix that for others. Provider 5.
Stigma and Cultural Norms
Providers worried about the lack of utilisation of sexual health and sexual wellbeing services by midlife women. This was often attributed to the societal stigma attached to midlife women being seen accessing sexual health and sexual wellbeing services. They had witnessed that many midlife women had ‘othered’ themselves from their sexual risk-taking behaviour, particularly when embarking on new relationships after long-term monogamy, and had not accessed sexual health and sexual wellbeing services. Public health campaigns to normalise sexual intimacy in midlife and issues that may occur in midlife were suggested.
But when you introduce the conversation about Sexually Transmitted Infection (STI) testing you find shame or embarrassment. Provider 2.
The late HIV diagnoses that we have seen have been in white middle-aged to older women with no sort of the inverted comma traditional risk factors for HIV. Provider 2.
Health Care System and Policy Construct
Inadequate Services
Providers discussed the absence of services which they viewed as essential for midlife women, including psychosexual services, sexual assault and domestic violence support, sexual pleasure advice, pelvic physiotherapy, vulval dermatology care, complex contraception, post-termination support, equitable access to menopause services, and trans and gender non-binary (TGNB) services.
We provide vulval pain care only. Obviously, that doesn’t encompass anywhere near the full range of sexual wellbeing and sexual dysfunction services that (midlife) women may need. Provider 2.
Lack of Evaluation and Research
The lack of research prioritisation and therefore evidence-based knowledge around women’s health and wellbeing issues, in particular the inadequate management strategies for many sexual health and sexual wellbeing issues related to the menopause, and the lack of contraceptive options for older women, were discussed.
The whole sort of systemic misogynistic, patriarchal sort of health service we have, I think, turns up, particularly in midlife and menopause, where there’s not been enough funding research interest. Provider 8.
Providers worried that basic demographic information was not being recorded by complex menopause services, which had been hastily established in response to the realisation (and public outcry) of the lack of WHWS. This made it impossible to ensure equity of access for underserved groups.
Complexity and Consultation Lengths
Acknowledgement of the economic challenges that were facing the National Health Service (NHS) did not detract from criticism of the lack of prioritisation of the needs of midlife women within the design and delivery of health services.
They (midlife women) rarely tend to come up in kind of funding remits as being of interest. It’s that kind of bit in the middle (age) that tends to not be of such interest to policy makers and funders. Provider 6.
Most providers felt that the complex, intimate, and interlinked nature of the challenges that midlife women encounter, and the consequent diagnostic and management uncertainty, were impossible to tackle without adequate consultation lengths. For example, they had often been required to sacrifice important holistic care, such as discussions about sexual wellbeing, to cover pressing clinical needs.
They’ve a contraceptive need, but actually what you then find out is that there’s a whole lot that goes with that, you know, having ended a relationship, started something new, feeling embarrassed about being newly sexually active, maybe struggling with no libido. Provider 2.
Our health services are not set up to spend time exploring or helping us live with the uncertainty that we’re not necessarily going to know what’s going on with us. Provider 8.
Restructured Services
Several providers advocated for the restructuring, using a co-design approach, of WHWS, including sexual health and sexual wellbeing services. A multidisciplinary service, with the reinstatement of direct referral pathways between specialities, consisting of primary care, sexual health, gynaecology (including urogynaecology and specialised services such as Female Genital Mutilation [FGM] care), pelvic physiotherapy, cervical and breast screening, mental health, and social services (including support for gender-based violence), was favoured. This would help to tackle protracted waiting times for the growing number of women with multiple morbidities. The current siloing of services in England curtailed the skills of many providers, and had precluded opportunistic preventative care, particularly important for underserved women, such as cervical screening in sexual health clinics and HIV Pre-Exposure Prophylaxis provision (PREP) in primary care.
A sex worker or an asylum seeker will have other health problems. It might be the only opportunity to see them- they wouldn’t necessarily re-present or come back for follow-up or referrals. It’s very much “we provide this care and I’m sorry we don’t do this”. Provider 2.
Several providers discussed the advantages, in terms of safety and lived-experience empathy, of HCP who identify as women working in sexual health and sexual wellbeing services. The heightened vulnerability during intimate procedures due to the communication challenges associated with living with a learning disability or neurodiversity was also highlighted. A suggestion to support anxiety, and thereby enable access, was standardised procedures within facilities that provide WHWS.
Practical Considerations
Flexibility in appointment times, childcare provision (recommended to be fully funded and on-site), and outreach provision to empower underserved women to access services were viewed as key components to improving access. Several providers felt that locating WHWS within underserved communities would contribute to feelings of safety and trust, reduce costs (financial and time), and therefore improve access to care.
It’s actually quite daunting. It’s going to be painful, probably. And I’ve got to go to somewhere that I’ve never been on my own. If you (midlife woman) could do that half a mile from their house, their mate (friend) can stand outside. Provider 9.
Progressive Practices
Providers felt that the recent regional change in STI self-testing kits, from being based on gender to anatomy, and the option of online testing methods (although not well-advertised for midlife women) had improved access for some midlife women. Several providers welcomed the increased access to contraception that community pharmacies now provide in England. They proposed further utilisation of community pharmacies to improve access to some forms of sexual wellbeing treatment, menopause treatment, and HIV PREP.
Cross-constructs Theme 2: Education About Midlife Transitions for Women
Intra-personal Construct
Poor Knowledge
Providers described poor knowledge among midlife women (Figure 2), particularly those living in underserved areas, about the health and well-being changes that are associated with midlife. This was felt to be partly due to the complexity of distinguishing treatable symptoms from the impact of lifestyle stressors. Women had often unsuccessfully self-managed conditions such as genitourinary syndrome of menopause (vulvovaginal and lower urinary tract symptoms related predominantly to low oestrogen levels) and incontinence, while believing that WHWS would not provide satisfactory management options, or due to outdated fears about side effects, for example, the commonly inflated breast cancer worry associated with HRT.
Often, they don’t think there’s a solution (for urinary incontinence). If it’s going to be a referral to urology and then an operation. It’s like actually those things are big things, aren’t they? Provider 4.
Cross-construct Enablers and Barriers (Theme 2).
Inter-personal Construct
Societal Knowledge and Attitude
Peer support, in the form of group work, information sessions, and community engagement, such as working with faith leaders, was viewed as the most effective way of disseminating information about midlife changes and services. The introduction of menopause to the English National Curriculum had been welcomed by many providers, particularly for communities where cultural norms result in less discussion of midlife changes. Several providers discussed the effect on access to WHWS of the unhelpful spread of false information among peers in the online sphere. One provider had encountered outdated attitudes from editors of local newspapers and magazines who had deemed the content of posters inappropriate when she had attempted to advertise Human Papilloma Virus (HPV) screening and menopause information sessions.
You have people sitting on those committees that don’t like talking about those things. You get your fair share of gatekeepers in the community. Provider 9.
Health Care System and Policy Construct
Attitudes (Health Care Professionals)
Several providers recounted consultations in which women had described how they had been deterred from care by paternalistic-style consultations in which they had not felt heard, their symptoms had been trivialised, or their concerns about medication had been dismissed. Several providers attributed delays, both in care that they had received and WHWS that they and their colleagues had provided to midlife women, to poor knowledge among HCPs about the diagnosis of menopause, the breadth of menopause symptoms, and management strategies for genitourinary syndrome of menopause. Providers advocated for developments in medical and nursing curricula and professional development education as methods to reverse the negative cycle of midlife women not accessing services due to their lack of trust in HCPs.
This lady had migraines, anxiety, she was forgetting words, having mood swings. She actually thought she was getting early dementia. And she had been to see her doctor (General Practitioner). And her doctor has said, oh, you’re too young for menopause. And she absolutely was perimenopausal. Provider 5.
Inaccessible Education
The prevalence and impact of inaccessible prose within healthcare information, and the lack of culturally appropriate co-produced information on access to WHWS, including sexual health and sexual wellbeing services, for women who spoke English as a foreign language or had low literacy levels, were highlighted. A community prescriber described several women who had been overwhelmed by cervical screening information and suggested that women who did not respond to invitations for preventative healthcare should have the process and benefits explained using individualised and evidence-based face-to-face methods.
Discussion
A diverse group of 11 providers, from different sectors and specialities, contributed a granular description of the enablers and barriers to WHWS, focusing on sexual health and sexual wellbeing services, for underserved midlife women in a region of South-East England. This study augmented evidence in the field of women’s health, 57 sexual health, 16 and public health,56,58 by outlining the perspectives of 11 providers of care who have insight into current and societal norms, organisational priorities, including the allocation of resources, and are able to contribute institutional memory to the analysis of policies within healthcare.
Comparison of Findings with Existing Research
This study corroborates findings from previous work that health care provision has not kept pace with the evolving sociocultural landscape for midlife women, 16 and that equity in access to WHWS, including sexual health and sexual wellbeing services, mainly attributable to the social determinants of health, continues to widen. 59 This study supports the evidence which has contributed to the aims of the Women’s Health Strategy for England, 60 together with recent work conducted by our group, which specifically projected the views of midlife women, 37 in advocating for a life-course paradigm in women’s health, 61 with specialist, holistic, multidisciplinary services (‘Women’s Health Hubs’) for women. Although providers in this study acknowledged the possible risks of ‘Women’s Health Hubs’ regarding the deskilling of General Practitioners (GPs), and the importance of ensuring that the long-term relationship-based knowledge that GPs provide for women is not eroded, concerns which have been highlighted in previous studies, 55 providers in this study felt that these risks were outweighed by the benefit of integrated services to midlife women. Indeed, the perspectives of providers of care, who have sometimes been viewed as enablers of systemic inequities, 55 share many similarities with those of the midlife women that they serve. 37 Substantiating previous evidence from midlife women, 37 they advocated for education for midlife women and Health Care Providers, 16 and commissioning changes, including a renewed emphasis on outreach provision 28 and that services are placed in the most underserved locations, 37 in order to address societal and organisational sexism and ageism, which affect access to health services globally. 29 Providers in these interviews also offered new feasible suggestions for improved access to WHWS, including sexual health and sexual wellbeing services, such as standardised (across regional clinics) procedures for midlife women living with neurodiversity, and tailored face-to-face interventions for midlife women who have repeatedly not responded to cervical/ breast screening invitations.
Strengths and Limitations
To the best of our knowledge, this is the first study to use the SEM, with an intersectionality lens, to explore the enablers and barriers to accessing WHWS, focusing on broader sexual health and sexual wellbeing services, for midlife women in the UK from the perspective of providers of care. By recruiting 11 providers who work in areas with significant disparities in access to WHWS and employing an intersectionality lens, this study highlights the specific experiences of those who work with the most underserved midlife women. Their insights from attempting to support and advocate for midlife women in challenging, vulnerable situations reinforced and augmented the evidence provided by midlife women in many high-income countries. 16 Qualitative studies which employ interviews are considered appropriate for eliciting views on sensitive topics such as sexual health and well-being. 62 The use of convenience sampling may have introduced selection bias. Although providers of health and well-being care are more likely to be women, and 55% of participants in our study were able to provide a valuable dual perspective (provider and midlife woman), negative personal experiences may have impacted their objectivity. Although the study reflects providers’ interpretations of patient experiences rather than first-hand accounts, it strengthens findings from a larger umbrella project, which is exploring access to women’s health services, including a qualitative study with women aged 40–65 years. 37 A disproportionate number of managers and leaders in this sector are men, 63 and their views on access to care for midlife women continue to significantly shape the healthcare system. If greater numbers of male-identifying providers had chosen to participate, this may have provided an additional lens to the work. Similarly, further work is planned to address the limitation of the lack of policymakers who choose to participate, as their considerations when evaluating evidence generated to improve or commission services are important. While it can be postulated that workforce and economic pressures and priorities correlate nationally, the generalisability of the results of this study is limited by the fact that regions in the UK are at different stages in their response to the first Women’s Health Strategy. 56 The sample size was relatively small, comprising only 11 participants, which limits the generalisability of the results. The exclusion of non-English language speakers among third sector providers may have resulted in a lack of representation of different cultural and national perspectives. Further work is needed to address the disparities in access to care for this group of women.
Implications for Research and/or Practice
Providers of care, reinforcing the view of midlife women, propose that the development of multidisciplinary, holistic, accessible (extended hours, childcare facilities), community-based (in the most under-served communities, emphasis on outreach and peer support), safe (predominantly providers who identify as women) WHWS, which offer increased pharmacy and self-testing options, and innovative public health education about midlife changes, are required to improve access to WHWS for this population. The lived experience of providers, many of whom are midlife women, must continue to be harnessed to co-design (with midlife women) and implement evidence-based strategies which address these challenges in sexual health and sexual wellbeing research and services.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors would like to thank the providers of care who participated in this study and the members of the Public Participant Involvement group.
Authors’ Contributions
KS: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, visualisation, writing.
JH: validation.
DH: validation.
CI: supervision, validation, writing-review and editing.
SB: supervision, validation, writing-review and editing.
CL: conceptualisation, formal analysis, supervision, validation, writing.
Data Sharing Statement
Due to the nature of the study, the data generated are considered confidential, and the study participants have been assured that the data are unavailable to anyone other than the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Ethical permission was granted by the Health Research Authority and Health and Care Research Wales Committee on 4.3.2024 (Ref no: 24/EE/0032). Respondents gave written consent for review and signature before starting interviews.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the University Hospitals Sussex NHS Foundation Trust (sub-project code WF003-16).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.