
Abstract
Background:
No clear consensus exists on the optimum management of vaginismus. Although vibrator therapy is of anecdotal use in vaginismus, the acceptability to patients is unknown.
Methods:
A mixed-methods study was conducted with 30 cis-women aged >18 presenting to a psychosexual clinic. The control group received standard care, including dilators, whilst the intervention group, in addition, received a vibrator. Initial questionnaires, including FSFI and FDS, were repeated after treatment at a minimum of 6 months, together with a semi-structured interview. Analysis included descriptive statistics and thematic analysis.
Results:
Data from 19 participants were suitable for analysis. The intervention group rated the vibrators as ‘mostly’ acceptable on a 5-point Likert scale (M = 4.3 (0.67)) and were more likely to report them as acceptable compared to the dilators (90% vs. 70%). Both the intervention and control groups showed an improvement in severity of pain scores, with the intervention group showing a greater improvement (M = 1.40–3.36 vs. control group: M = 1.96–2.62). Qualitative analysis identified key themes: (a) the challenges of dilators, (b) increased confidence, (c) vibrators compared with dilators and (d) other helpful elements of therapy.
Conclusions:
The use of patient-administered vibrator therapy was acceptable as an addition to existing treatment for vaginismus. Vibrators were more positively perceived than dilators by the intervention group. Results from this pilot study are encouraging and indicate that vibrators in the treatment of vaginismus may be beneficial when offered as part of a multi-modal approach, although a full comparison study is required to investigate the effectiveness of using vibrators to improve outcomes in vaginismus.
Keywords
What Is Already Known on this Topic
The prevalence of vaginismus is variable across different female populations, ranging between 0.5% and 17%. Approaches to treatment are varied and lacking in clear evidence of acceptability and effectiveness, and a multi-modal approach to management is currently standard.
What this Study Adds
Acceptability to patients of the use of vibrators in the treatment of vaginismus has not been specifically investigated until this point.
How this Study Might Affect Research, Practice or Policy
The findings identify the need for further investigation into the effectiveness of vibrator therapy in the management of vaginismus. It supports the inclusion of patient-controlled at-home vibrator therapy as an adjunct to current treatment for vaginismus. Further studies investigating the effectiveness of any intervention should be co-produced with patients.
Introduction
Vaginismus results from the involuntary spasm of the pelvic floor muscles surrounding the vaginal wall. 1 This can make sexual intercourse painful, difficult, or impossible, thereby impacting sexual pleasure, relationships, and the ability to conceive. 1 There is often overlap with vulvodynia, defined as vulval pain of at least three months’ duration, which may be provoked or unprovoked. 2 Vaginismus, vulvodynia, and vestibulodynia are now grouped under the umbrella term of genito-pelvic pain disorder (GPPD). 3
There is little consistent evidence on the effective treatment of vaginismus and the patient perspectives of current treatment methods.4,5 Vaginal dilators may be recommended by medical practitioners 6 ; however, patients frequently report anxiety or frustration whilst using them. 7 This study aimed to explore the feasibility and acceptability of the use of patient-controlled external vibrators as an adjunct to existing therapy, which included vaginal dilators, and patient attitudes toward self-treatment with dilators and vibrators.
Treatment for vaginismus often incorporates medical and psychosocial interventions alongside self-help and practice. 6 Current medical therapy may include topical local anaesthetic gel, and sometimes oral medications such as low-dose Tricyclic Antidepressants, where there is co-existing vulvodynia. 8 In vaginismus, self-administered progressive vaginal dilator therapy and physiotherapy may be recommended. 6 Psychological therapy may consist of group psychoeducation or one-to-one psychosexual therapy.9–12 The fact that there is not a clearly culpable aetiology (causes are likely to be multifactorial) means that there is no ‘gold standard’ treatment for vaginismus and vulvodynia. 13 A multi-modal approach is recommended in national guidelines to manage vulvodynia, 14 and is recommended to manage vaginismus.6,15
Anecdotally, some women find that clitoral stimulation can sometimes have a positive impact on the ability to progress with vaginal dilator treatment as well as the general enjoyment of sexual intimacy, but this, in the context of vaginismus has not yet been evaluated in a research setting. In the general population, vibrator use has been positively correlated with more positive sexual function, higher levels of desire and arousal and lower levels of pain. 16
Clinical guides for the role of mechanical devices in treating female sexual dysfunction have previously acknowledged the paucity of clinical evidence of effectiveness, but also highlight the fact that these are safe and without significant adverse effects. 17
This study is the first exploration of the use of vibrators as an acceptable treatment for vaginismus. It aimed to use standardised and novel questionnaires and semi-structured interviews to explore patient perspectives around vibrators to inform whether a fully powered trial in future would be beneficial.
Methods
Design
The study used a mixed-methods design to explore the acceptability, feasibility and effectiveness of vibrators as an adjunct to standard care.
A non-randomised controlled study compared current local standard care to standard care plus intervention (vibrator). The standard care included being given a set of dilators, signposted to the clinic’s vaginismus workbook website containing useful resources and being offered care through a psychosexual therapy group. The intervention group were given a vibrator at the same time as the dilators. The comparison allowed data to be collected on the acceptability of the vibrator to determine whether an intervention is appropriate for further testing. 18 Effectiveness and acceptability were assessed using self-report questionnaires and thematic analysis of qualitative data.
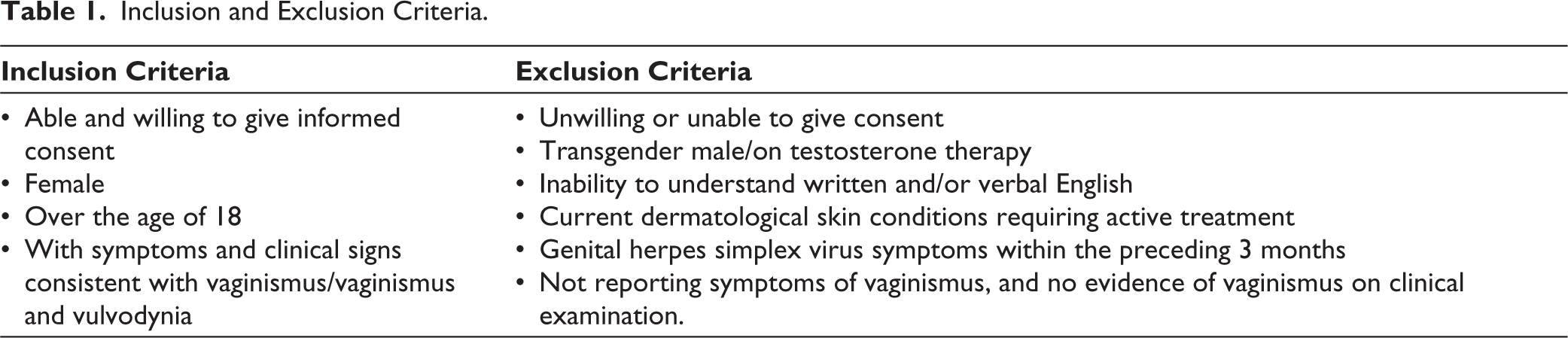
Participants were screened and recruited from a single clinic in a diverse area of East London. Inclusion and exclusion criteria are listed in Table 1.
Inclusion and Exclusion Criteria.
Due to clinical service constraints, randomising was not possible for this pilot study. Patients enrolling on the study were not told at recruitment which arm they would be placed into until after consent. The research was granted full NHS ethical approval by Camden and Kings Cross REC.
Initial questionnaires were completed by participants either on the day of enrolment or via phone call shortly after, per participant preference. To investigate effectiveness, two validated questionnaires were administered at baseline: Female Sexual Distress Scale (FSDS) 19 and Female Sexual Function Index (FSFI). 20 To assess acceptability, a third study-specific questionnaire captured demographic information and initial attitudes to aspects of genital touch and penetration via responses to a 5-point Likert scale. After the intervention period and after group therapy between 6 and 12 months, the initial three questionnaires were repeated. At this follow-up, a semi-structured interview was included, which enquired into the patient perspectives and acceptability of vibrators and dilators. All follow-up questionnaires were carried out via phone call per patient preference.
The FSDS is a 13-item questionnaire designed to measure sexually related personal distress, including the psychological impact of sexual dysfunction, and feelings of anger, frustration, and worry related to sex. The reported internal consistency of this measure is adequate (Cronbach α = >0.86), along with an adequate test-retest reliability (r = >0.74). 19
The FSFI is a 19-item questionnaire which uses 5-point Likert scales to investigate different domains of desire, arousal, lubrication, orgasm, satisfaction and pain. FSFI gives a score out of 36 with severe FSD (2–7.2), moderate (7.3–14.4), mild to moderate (14.5–21.6), mild (21.7–28.1) and no FSD (28.2–36). Each domain is weighted, resulting in an overall score of sexual function, but it can also be analysed separately. Each of the six domains presented high test-retest reliability (r = >0.79) and a high degree of internal consistency (Cronbach α = 0.82). 20
The study-specific questionnaire asked demographic information about current attitudes towards genital touch using a 5-point Likert scale responding to statements, for example, ‘I feel comfortable touching my vulva (genitals)’, and assessing overall acceptability of the dilators and vibrator, their perceived helpfulness in managing symptoms, and if they would recommend them to others with similar issues to them. Participants were also asked whether the vibrator and dilator were used together or separately, and how often these were used. Following this, open-ended questions were asked as per Table 2.
Open-ended Questions Were Used in the Final Patient Questionnaire.
Setting
The study was recruited from one London sexual health clinic. Data were collected from August 2021 to June 2024.
Data Collection
The three initial and three follow-up surveys lasting 15–30 minutes were conducted via telephone or paper-based, depending on participants’ preference.
Three or four semi-structured interview questions elicited general feedback about treatment, helpfulness and acceptability of the dilators and for the intervention group, the vibrator. Survey responses were transcribed verbatim.
Participants
Participants were recruited from an East London Sexual Wellbeing Clinic.
Participant Recruitment
Eligible patients were offered enrolment in the study. It was not discussed with the patient prior to enrolment which study arm the patient would be in. A Patient Information Leaflet (PIL) was provided in person for the participant to read, with an option to either enrol in the study on the day or shortly afterwards. Contact details for the researcher were provided on the PIL in case the participant requests withdrawal from the study at any time. It was clarified that participation in the study was voluntary; declining involvement would not negatively affect care. All study participants gave informed consent to participate before taking part.
Patient and Public Involvement
This project was informed by the author’s work with patients with vaginismus and responding to the desire of the patient group to feed into further research in the area. Study results will be disseminated to study participants who have requested to see the findings.
Analysis
Due to the sample size <30, the data did not meet parametric assumptions, 21 and so tests for normality were therefore not completed. Bivariate comparisons of quantitative data were conducted using Mann-Whitney U tests.
Qualitative data were analysed using a thematic analysis approach using Braun and Clarke’s method. 22 Two authors independently read the data, and once familiarised, coded the data, met to discuss and, following consensual agreement, redefined themes. Detailed qualitative statistical analysis was not planned due to this being an acceptability study.
Results
Quantitative
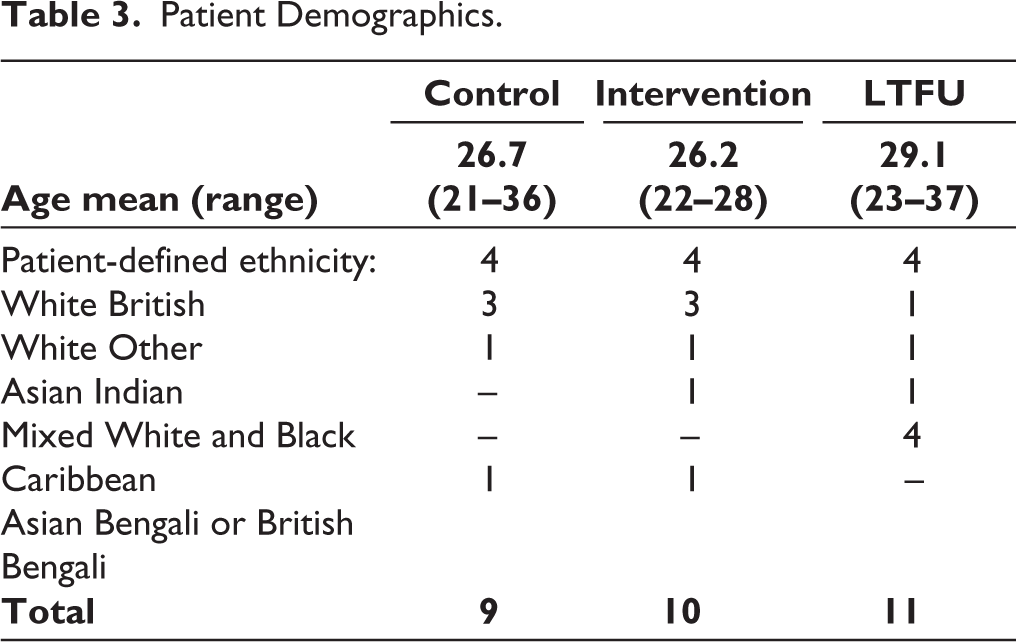
A total of 30 eligible participants were enrolled and completed the consent form. 19 patients were suitable for final data analysis. A total of 11 patients were unresponsive to contact at the time of the initial or follow-up survey. Table 3 presents participant demographics.
Patient Demographics.
For both groups, we waited until any group therapy had been completed prior to final surveys and interviews (intervention M = 10 months vs. control group M = 11.5 months). No control group participants reported vibrator use, and all intervention group participants had used the vibrator. Study results are collated in Table 4.
Comparison Scores Along Multiple Domains for Control Versus Intervention Group at Initial Appointment and at Follow-up.
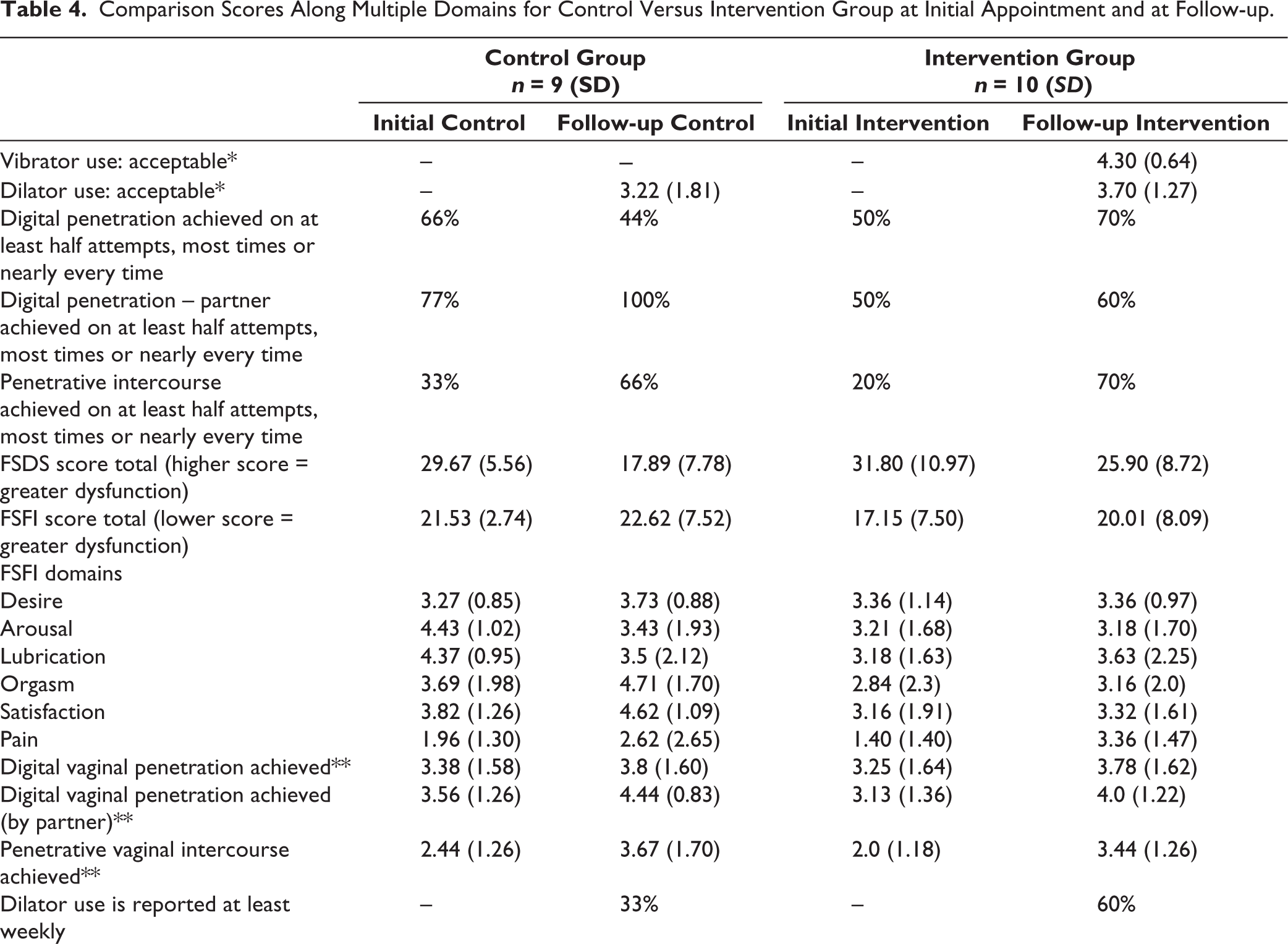
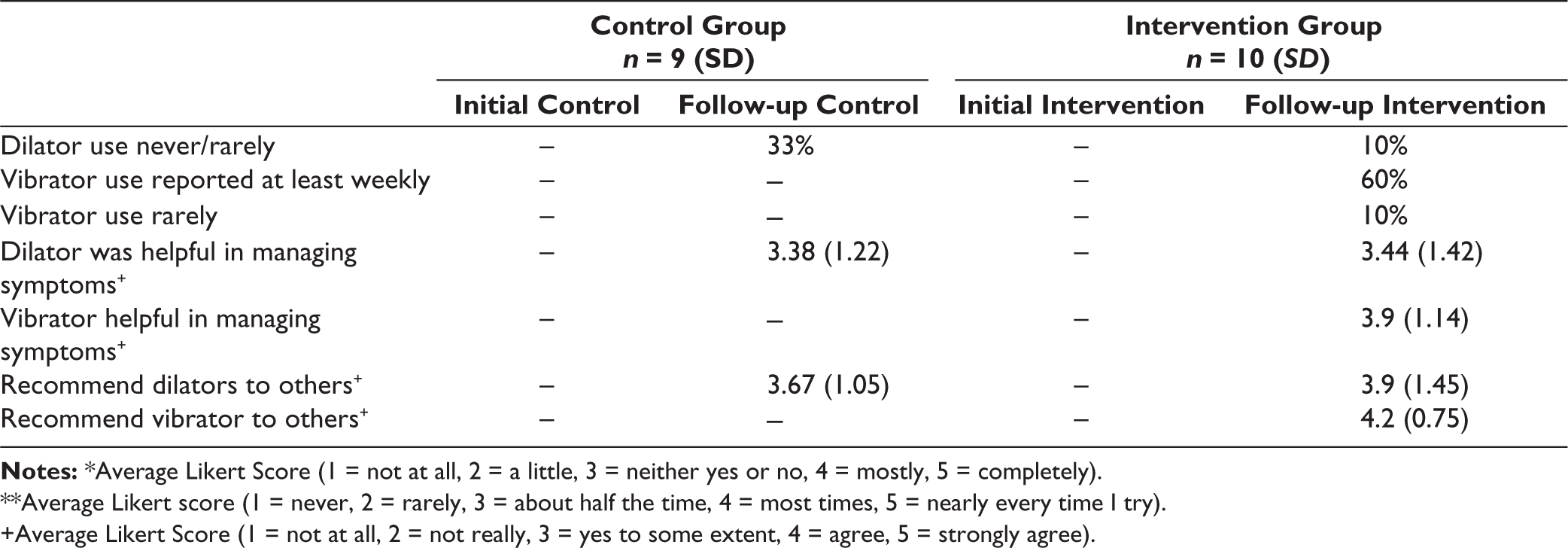
**Average Likert score (1 = never, 2 = rarely, 3 = about half the time, 4 = most times, 5 = nearly every time I try).
+Average Likert Score (1 = not at all, 2 = not really, 3 = yes to some extent, 4 = agree, 5 = strongly agree).
Acceptability
The intervention group rated the vibrators as more acceptable than the dilators (M = 4.30 (0.67) vs. 3.70 (1.34)) on the 5-point Likert scale. A larger proportion of the intervention group rated the vibrator as ‘mostly’ or ‘completely’ acceptable compared to the dilators (90% (n = 9) vs. 70% (n = 7)), whereas this fell to 56% (n = 5) for those in the control group using the dilators.
In response to the statement, the vibrator has helped me manage my symptoms 80% (n = 8) of the intervention group agreed to some extent, agreed or strongly agreed, compared to 60% (n = 6) regarding dilators (M = 3.9 (1.20) vs. M = 3.4 (1.5)). In the control group, 77% (n = 7) also agreed that the dilators helped manage their symptoms (M = 3.38 (1.30)).
The majority of participants either ‘agreed’ or ‘strongly agreed’ that they would recommend dilators to people with similar issues to them (control: 75%, n = 6 vs intervention: 60%, n = 6), however 80%, (n = 8), stated they would recommend vibrators, with the remaining two women agreeing to some extent that they would recommend vibrators to those with similar issues to themselves (dilator: control M = 4.1 (1.13) vs. intervention: M = 3.9 (1.52), vibrator M = 4.2 (0.80)).
Secondary Outcomes
FSFI Pain
Both the intervention and control groups showed an improvement in severity of pain scores, with the intervention group showing a greater improvement in the adjusted domain score from M = 1.40 to 3.36 (control group: M = 1.96 to 2.62).
FSFI
Diagnosis of FSD was not a requirement for enrolment. A score of below 26.55 on the FSFI indicates FSD. 88% (n = 9) of the control group and 80% (n = 10) of the intervention group scored below this threshold at the initial survey. Both control and intervention groups showed an average improvement in FSFI total score (control M = 21.53 to 22.62, intervention group M = 17.15 to 20.01).
FSDS
Both groups showed a reduction in the FSDS scores, indicating a reduction in reported severity of sexual dysfunction throughout the intervention period (control: initial M = 29.67 (5.89) to M = 17.89 (8.25), intervention: M = 31.80 (11.56) to 25.90 (9.19)).
Penetration
Likert scales were used to measure digital penetration either solo or with a partner, and penetrative vaginal intercourse. In both the control and intervention groups, there was an increase in partnered digital penetration (increase in those scoring most or nearly every time, control: 23%, intervention: 10%). For penetrative vaginal intercourse, again, there was an increase in those engaging in this half the time, most times, nearly every time at follow-up, with this being higher in those in the intervention group (control: 33% increase, intervention: 50% increase). By the end of the study, 60% of those in the intervention group were engaging with partnered digital penetration and 70% vaginal penetration following treatment.
Qualitative
Qualitative analysis identified three key themes: (a) challenges of therapy, (b) feelings of increased confidence or comfort in the body, (c) positives of vibrators compared to dilator therapy, and (d) other helpful aspects of the therapy. There were a variety of experiences, but an underlying theme of positivity regarding perceived treatment-related improvement was identified throughout the narratives.
Challenges of Therapy
Time constraints were mentioned more in the control group than in the intervention group. Both groups expressed challenges of therapy and spoke about their mixed feelings around dilators, some finding them helpful but feeling scared of using them and were frequently described in negative terms, such as ‘not being comfortable’ or ‘painful’. One participant spoke about dilators ‘bringing up past trauma’. ‘Difficult’, ‘not my favourite thing’, ‘mechanical’ were also used to describe experiences with dilators. Alongside the challenges, participants mentioned relaxation or breathing exercises, which helped them to feel more comfortable with dilators. The difficult emotional side of using dilators is well illustrated in this quote:
I found it (using dilators) - once I got used to it - … a little mechanical. If I’m too focussed it separates from enjoyment. I feel like it lowers my desire. I feel like I use it to get over my problem, but it feels disconnected from enjoyment. I think I made progress physically but not in terms of connecting my body to pleasure. I feel like it is a chore. (IG14)
Feelings of Increased Confidence or Comfort in the Body
This theme came entirely from intervention group participants (those receiving vibrators). Numerous mentioned feeling more comfortable and confident in their sexuality. Participants also attributed vibrator use to decreased experience of pain and learning about their bodies ‘for themselves’.
Very, very helpful … (The vibrator) really helped me become more comfortable with my sexuality, sex life and not feeling shameful about it.
Positives of Vibrators Compared to Dilators
The intervention group participants, unprompted, would often compare the dilators and vibrators, expressing more positive opinions towards the vibrator than the dilators. Comments included the vibrator being more helpful, less scary, and making self-treatment more comfortable. A common thread was participants finding the vibrator helpful with relaxation prior to attempting dilators. Participants reported the variety of ways that they used vibrators alongside, or instead of, dilator therapy, which supports the role of the vibrator as a tool for self-exploration in this group.
I think vibrator was good and helped with insertion. It really helped to use it with my partner rather than on my own. The dilators I never used. (IG11)
Um … I think it (vibrator) was very useful at the beginning. It was the extra piece that was missing. As I was progressing with dilators more and more I just couldn’t make myself associate the pleasure aspect. (IG14)
The vibrator was most helpful. The dilator was less helpful - I felt like they are not something I wanted to engage with. Vibrator was the most helpful. Just because I don’t have a problem with having an orgasm. It helped with lubrication, and relaxing before attempting penetration. (IG15)
Um … yeah I didn’t get on too well with the dilators. I wasn’t in the headspace to try them …. I liked it (vibrator) and found it really helpful when using it externally. (IG15)
I often use the vibrator before dilators or penetration and I feel that helps …. I really liked using it especially when going up a size, it helps me to relax and slightly numbs the skin before inserting which I find really helpful. It is really useful. (IG16)
Dilators and vibrator together were super useful and helped me overcome the vaginismus …. I found the vibrator really straightforward, and really helpful for using the dilators. (IG17)
Other Helpful Aspects of the Therapy
The women in both the control and the intervention group spoke widely about how helpful the group therapy and the workbook they were provided with were in improving their understanding of vaginismus. Participants mentioned the role of relaxation and mindfulness exercises in managing vaginismus, as well as learning about ways to communicate with their partners. The community element of group therapy, in particular feeling like they ‘weren’t alone’ as well as having an opportunity to ‘hear other women’s experiences’ were mentioned as a central part of the benefits of the therapy.
… learning … about the impact on relationships and how to talk to a partner was helpful. Realising I wasn’t alone and penetrative sex is not the only way of enjoying sex was helpful for me to learn. (CG5)
Discussion
This study is the first study to assess the acceptability of vibrators as an adjunct to treatment for women with vaginismus. It aimed to explore patient perspectives around the use of vibrators. In this patient group, the great majority of participants receiving a vibrator found using a vibrator to be acceptable, with all participants reporting that they would recommend vibrators at least to some extent, if not more, to others with similar issues to themselves. This study suggests vibrators are an acceptable addition to the current multi-modal approach for management of vaginismus.
As it was a small acceptability study, the sample size was not sufficiently powered for statistically significant differences to be found. However, some encouraging results were seen using validated measures. Both the FSFI and FSDS showed a reduction in pain and severity for both groups, with a greater reduction in pain scores for those who used the vibrators. This not only supports the effectiveness of the local standard care, but it is encouraging to see that most participants were engaging in some form of penetration by the end of the study, and that this increase was more pronounced in those who used the vibrator.
These initial positive findings cannot be put down to the dilators nor vibrators alone, as the study is measuring the whole programme, including medical review and access to an online workbook, followed by short-term group psychology input. When questioning the role of the vibrators alone, participants unprompted compared the dilators and vibrators, expressing more positive opinions towards the vibrators than the dilators, highlighting a preference and acceptance of the vibrators.
The women in this study expressed time constraints and challenges associated with both vibrators and dilators, with remarkably positive feedback regarding the vibrator in terms of increasing confidence in self, but also as a complementary tool to the other components of the treatment, for example, mindfulness and breathing, and psychoeducation about vaginismus and the normalising of this. This supports current advice and guidance, which recommends a multi-modal approach to managing vulvodynia and vaginismus.
Limitations
This is an acceptability study at a single site with a small sample size, which limits the generalisability of these results as significance testing could not be completed. However, the encouraging acceptability of the vibrators was found with a relatively diverse patient population in an area of high poverty and deprivation. Randomisation was not possible due to the group therapy aspect, and blinding was not possible due to the nature of the intervention. Although approximately one-third of enrolled study participants were lost to follow-up, this rate was consistent in both study arms.
The FSDS and FSFI are the most used scales in female sexual wellbeing, 23 but both have been shown to be less accurate in patients who do not have sex due to the focus that the FSFI places on partnered sex. 24 Fifteen of the 19 items in the FSFI have a zero category for ‘no sexual activity’ or ‘did not attempt sex’, which may be conceptually distinct from the assessment of sexual functioning. 24 A few of the participants reported no partnered sex, which might have impacted the usefulness of FSFI. Survey responses were taken over the telephone for patient convenience, which might have impacted responses; however, participants were encouraged at the start to give truthful answers.
The study clearly considers the holistic programme of medical review, followed by group psychology input and not just the provision of dilators/vibrators to patients. It is therefore difficult to dissect the impact that the vibrators alone had on the participants. The very positive participant testimonies regarding the acceptability of vibrators do support their use as an adjunct to existing therapy for managing vaginismus.
Conclusion
Research remains sparse within the field of sexual health and sexual pain,4,5 so although this is a small-scale study, results are encouraging and indicate that the use of vibrators in the treatment of vaginismus is acceptable to patients. Vibrators were more positively perceived than dilators in the intervention group participants. Patient-controlled vibrators are likely to be useful when offered as part of a multi-modal approach, although a full comparison study is required to investigate the effectiveness of using vibrators to improve outcomes in vaginismus.
Footnotes
Acknowledgements
Grateful thanks go to all the patients who participated, and clinicians and psychologists who were involved in the study. Thanks for Dr Jill Zelin for providing expertise and support. Thanks also to MV.Health, who kindly provided the vibrators used in the study.
Author Contributions
J Gaddie: Study design, ethical proposal, consenting, data collection, analysis. F Saunders: Consenting, data collection, analysis, statistical analysis. J Vosper: Editing, study limitations, advice on qualitative analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study involves human participants and was approved by the Camden and Kings Cross REC.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Participants gave informed consent to participate in the study before taking part.
Registration Database
Study details: Feasibility of Use of Vibrators With Vaginal Dilators for Vaginismus (Vibrator Therapy and Dilators in Vaginismus). ClinicalTrials.gov identifier: NCT04635345. Sponsor: Barts Health NHS Trust. Information provided by Barts Health NHS Trust (responsible party). Available at: