
Abstract
Background:
Sexual health and sexual quality of life are integral to a person’s physical and mental health as well as well-being. Nevertheless, there is a dearth of literature on how South Asian healthcare professionals perceive offering sexual health education and counseling to patients within the South Asian context, where discussion of sexuality is considered taboo.
Purpose:
The aim of this article was to explore healthcare professionals’ perspectives regarding approaches to enhance delivery of sexual counseling to cardiac patients.
Methods:
A qualitative descriptive study was conducted. Healthcare professionals were recruited using maximum variation sampling and interviewed using a semi-structured interview guide from June to September 2023. Reflexive thematic analysis was used for data analysis.
Results:
Analysis of the 11 interviews revealed three main themes: (a) gaps in patients’ sexual health knowledge and receipt of counseling, (b) need for health professional training to promote open discussion about sexual health with patients, and (c) activating organizational action to support the provision of sexual counseling.
Conclusion:
Structural and cultural barriers impede consistent implementation of sexual health assessment and counseling of cardiac patients, despite needs. Sexual health education of professionals across relevant disciplines, structural changes to support healthcare professionals in sexual counseling, provision of sexual health assessment checklists, tools, and practice guidelines, patient education, and providing written sexual health education material in local languages are potential strategies.
Introduction
Sexual health and sexual quality of life are integral to a person’s physical and mental health as well as well-being. Cardiovascular events can negatively affect sexual health and sexual quality of life and can lead to sexual dysfunction in these patients. 1 According to the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5), sexual dysfunction is defined as a disruption in the sexual cycle or painful sexual intercourse. The problems included in sexual dysfunction are premature ejaculation, sexual desire disorder, sexual pain, female sexual arousal dysfunction, male and female orgasm dysfunction, and male erectile dysfunction. 2
After having a cardiac event, a high prevalence of sexual dysfunction has been reported in men (40–70%) 3 and women (43 to 87%). 4 Commonly reported sexual dysfunctions in men are impotence, loss of libido, as well as premature ejaculations, and orgasm. In women, vaginal dryness, lack of sexual desire, arousal difficulty, pain, and sexual dissatisfaction were frequently reported. 5 The factors that are associated with sexual dysfunctions and poor sexual activity in cardiac patients include fear of sexual activity initiation, emotional distress, poor lifestyle behaviors, relationship problems, depression, anxiety, medications, lack of knowledge about initiating sexual activity after a cardiac event, and lack of sexual counseling from healthcare professionals.1,6
The effectiveness of sexual counseling to improve sexual quality of life after experiencing a cardiac event is well-established. 7 Sexual counselling aims to assess patients’ sexual needs, clarify their sexual concerns, and facilitate their safe resumption of sexual activity. 8 Sexual counseling is crucial for both cardiac patients and their partners because it reduces fear, anxiety, and depression, and improves relational well-being.1,9–12 Mohsen et al. 11 conducted a randomized controlled trial (RCT) and identified that the mean sexual quality of life was significantly higher (60.7) in patients who received sexual counseling compared to a control group (48.2) who received conventional treatment (P < .001). Tuncer and Oskay 13 also conducted an RCT to determine the effect of sexual counseling on sexual quality of life and sexual function among women undergoing open heart surgery. Results showed that after sexual counseling, the rate of sexual intercourse increased significantly (65.6% vs. 18.8%), more women were sexually satisfied (66% vs. 19%), fewer women reported sexual problems (34% vs. 81%), and few women (34% vs. 81%) raised concerns regarding returning to sexual activity after surgery (P < .001).
Despite the proven effectiveness of sexual counseling in improving sexual quality of life, studies suggest that patient sexual health or needs are rarely assessed by healthcare professionals due to several personal, organizational, and social barriers.14–17 However, numerous studies reported that patients want education about resuming sexual activity 18 and these concerns are even more evident among their partners.1,6 This lack of assessment of sexual health and needs presents a missed opportunity in delivery of holistic sexual healthcare, thereby affecting the overall well-being and individual and family life of individuals with post cardiac events.
Several approaches and tools for the sexual assessment of cardiac patients have been reported in the literature. 7 Nevertheless, there are limited studies to explore the perspectives of healthcare professionals regarding approaches to enhance the implementation of these tools and to deliver sexual counseling in cardiac patients. Some previous research has pointed to issues regarding lack of time, lack of training, and a taboo; these studies have generally been undertaken in North America and Europe. 19 Specifically, there is a dearth of literature on how South Asian healthcare professionals perceive offering sexual health education and counseling to patients within the South Asian context, where discussion of sexuality is considered particularly taboo. 20
Purpose
The purpose of this study was to explore healthcare professionals’ perspectives regarding approaches to enhancing sexual assessment and delivery of counseling to cardiac patients.
Methods
Design
A qualitative descriptive design was used. Qualitative description is the best methodological choice when the primary purpose is to explore participants’ unique perspectives through developing a firsthand account of their perspectives.21,22 The Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines were used to report study findings (Supplementary file A). Research ethics approval for the study was obtained from the review committee of Riphah International University (Riphah/IIMC/IRC/23/3042). All participants signed written informed consent.
Study Setting, Sample, and Recruitment
The study was conducted in Pakistan, a country where sexuality dialogue is considered taboo. 20 Healthcare professionals from various public (government) hospitals in Islamabad and Rawalpindi were invited to participate in the research. Participants were also recruited from a specialized public institute of cardiology in Rawalpindi. Public hospitals and healthcare institutions in Pakistan are significantly different in terms of funding, care access, facilities, quality of care, and patient experience. The population of interest was healthcare professionals (cardiologists, nurses, and physiotherapists) who have worked in the last five years or are currently working in coronary care units or cardiology wards. Healthcare professionals who did not have experience working with cardiac patients were excluded. The maximum variation nonprobability purposive sampling technique was used to recruit participants. 23 This sampling method is particularly useful when researchers are interested in studying perspectives of people with various backgrounds and experiences. 23 Brochures that contained the study title, purpose, eligibility criteria, interview method, approximate interview time duration, and primary researcher contact information were placed in various hospitals. In addition, social media outreach strategies were also used.
Procedures
Data were collected between June to September 2023. The lead author conducted in-depth interviews via Zoom with healthcare professionals from diverse backgrounds and with distinct experiences using a pre-developed interview guide. The data collector is PhD prepared with rich experience and skills in conducting interviews and qualitative research. Interviews were audio-recorded with consent. They were held in the English or Urdu language; the majority of the participants used both during the interview. The interviewer created an environment of open discussion so that participants could share their in-depth views regarding the subject under discussion. The interviews lasted for 32 to 58 minutes.
Data Collection Instrument
The interview guide was developed following the five-step framework for designing a semi-structured interview guide outlining the purpose, nature, and need for semi-structured interviews. 24 The preliminary guides (both in English and Urdu) were pilot tested with two healthcare professionals to assess the comprehensibility and construction of the questions, language, and overall flow of questions. Based on the participants’ feedback, the guide was revised, and the final version was used in the study. The revision included minor changes in words and phrases and addition of a few questions regarding organizational norms concerning sexual health counseling.
Data Analysis
Data were analyzed using reflexive thematic analysis, which enables a thorough understanding of interconnected themes in data.25,26 Content analysis is also an appropriate method of data collection in qualitative descriptive studies.21,22 However, reflexive thematic analysis was chosen because it aligned with the constructivist stance of the researchers, acknowledges researchers’ subjectivity and reflexivity, and allows for more nuanced interpretation of data. 26 Two researchers worked together during data analysis. The audio-recorded interviews were transcribed, and to gain a deeper understanding of the data, written transcripts were read several times. Initial codes were developed using semantic orientation and inductive orientation. Preliminary codes were evaluated for appropriateness and relevance to the data, and subthemes and themes were generated after arranging codes with similar meanings. 26
Rigor
To establish rigor, we implemented analytical moves following the methodological bricolage metaphor. 27 It calls for cobbling multiple methodological decisions and choosing a combination of analytical moves to promote competence, integrity, and benevolence. 27 We used several analytical moves: prolonged engagement with participants during interviews; peer debriefing through regular meetings within the team to discuss the design analysis processes; and rigorous translation and transcription of interviews into the English language was completed to ensure that the essence of participants’ experience was captured without losing the linguist meaning. 28 During analysis, it was ensured that themes were developed by staying close to the data. 29 Decisions about the analysis process were explicitly outlined to maintain an audit trail. Both researchers who completed the analysis kept reflective journals and jotted down any biases about participants and the phenomenon. The MIRACLE narrative framework was used to provide authentic, interpretative, and contextualized narrative of participants’ experiences. 30
Findings
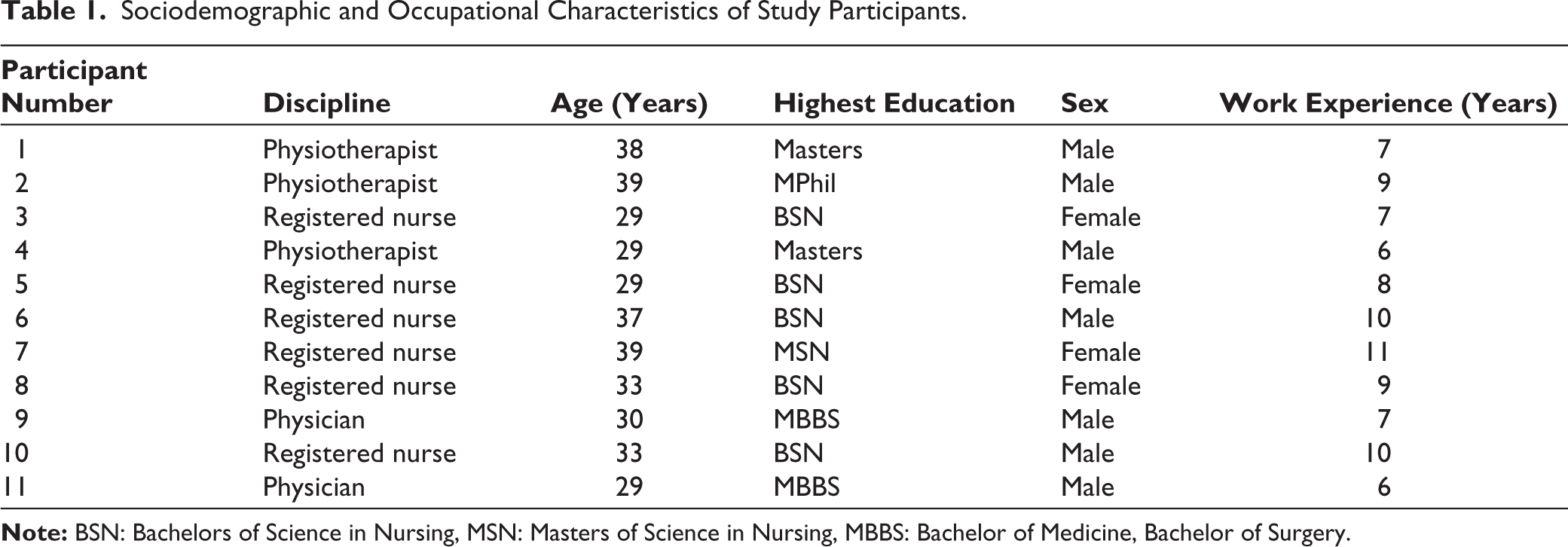
Overall, 11 interviews were conducted. Data saturation was achieved after ten interviews; however, one additional interview was conducted to see if there were any further useful perspectives. Of these, six were registered nurses, three physiotherapists, and two cardiologists all working with cardiac patients. The ages of these participants ranged between 29 and 39 years, and seven were male. Demographic and occupational information is summarized in Table 1.
Sociodemographic and Occupational Characteristics of Study Participants.
Themes
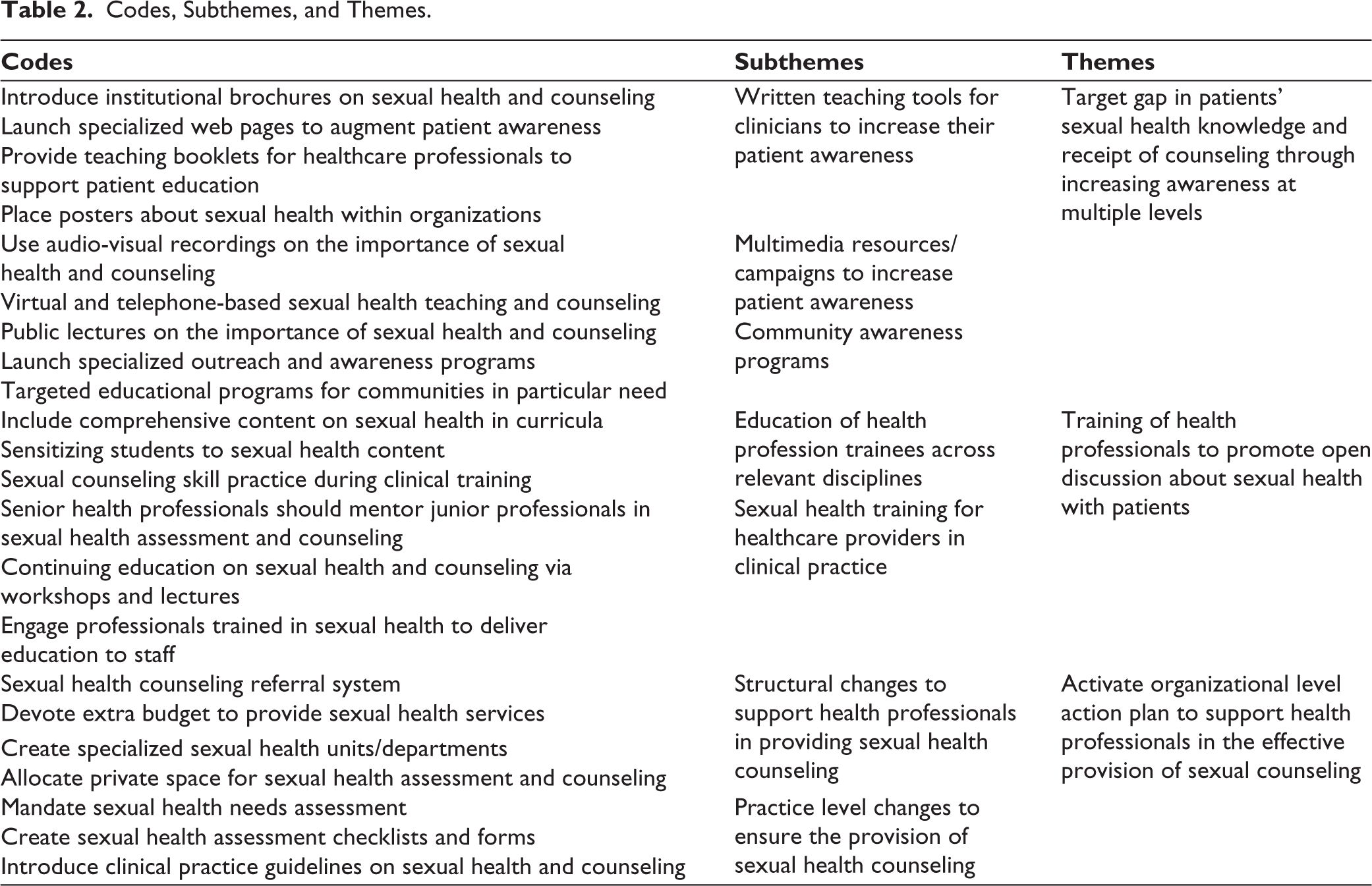
Three themes related to the healthcare professionals’ perspectives regarding approaches to enhancing sexual counseling were generated. A detailed description of these themes is provided below, and a summary of codes, subthemes, and themes is given in Table 2.
Codes, Subthemes, and Themes.
Target Gap in Patients’ Sexual Health Knowledge and Receipt of Counseling Through Increasing Awareness at Multiple Levels
Heath professionals discussed that patients are mostly unaware of the importance of sexual health in cardiac disorders or after surgeries/procedures, or that they are not comfortable talking about sexual health because of social unacceptance of open discussion. They highlighted that targeting gaps in patient sexual health knowledge is critical to promote awareness and hence an open discussion of sexual health and counseling needs is required.
There is a need to educate patients and the community on sexual health and its importance to promote open discussion on these issues. For patients, educational material in the form of pamphlets should be distributed, and educational material should be posted in various places in the hospital. (Registered Nurse, Female)
Health professionals highlighted a range of organizational to individual-level approaches to increase patients’ knowledge and awareness. Most commonly noted suggestions included developing and distributing booklets on sexual health and counseling services to patients and healthcare professionals, introducing institutional brochures on sexual health and counseling, launching specialized web pages, and placing posters about sexual health within organizations. They also emphasized that booklets should be written in simple, accessible, and culturally sensitive language to ensure that patients do not find them intimidating. Health professionals also noted that multimedia should be effectively leveraged to increase awareness, such as providing virtual sexual counseling services.
Health organizations should conduct lectures and improve our knowledge, then we will be confident; like we cannot even talk to the cardiologists with opposite-sex about sexual health. (Registered Nurse, Female)
Regarding community awareness, health professionals placed a great emphasis on public lectures on the importance of sexual health and counseling, specialized outreach and awareness programs, and targeted educational programs for communities in particular need. They highlighted that passive awareness methods such as posters, brochures, talk shows, and audio-video aids should be supplemented with active outreach methods to increase awareness about the importance of sexual health and sexual counseling to mitigate social unacceptance and stigma about sexual health. For example, one of the health professionals elaborated on how community awareness programs can be implemented:
There should be community awareness [raising] through social media, news channels, and new newspapers, and even doctors should take the initiative to organize programs for people in remote areas or areas where there is low literacy. Healthcare professionals need to provide education to the general population about discussing these issues so that we can help them. At the provincial level, the health minister and other people involved should highlight this issue as a big issue. (Cardiologist, Male)
Training of Health Professionals to Promote open Discussion About Sexual Health with Patients
Health professionals indicated the need for comprehensive education across their training and continuing through their practice. First, they highlighted the need to offer adequate education during clinical training to ensure that graduates are confident and competent to care for patients’ sexual needs and offer sexual counseling. Second, health providers highlighted the need for continuing professional education on sexual health, sexual quality of life, sexual needs, and sexual counseling approaches. The need for adequate training was considered important to prepare professionals for open discussion about patients’ sexual issues and delivery of services.
The main strategy is that health professionals need to be educated. At the departmental level, we should organize seminars and conferences. We need to educate healthcare professionals that sexual counseling and sexual health is not a taboo topic, and we should discuss with patients rather than patient approach quacks for their sexual issues. So, it is important for the person who is delivering counseling to understand sexual education and how to do that. (Registered Nurse, Male)
Sexual assessment and counseling training were emphasized to sensitize healthcare students to content. Health professionals indicated that this sensitization is critical because talks about sexual health are often not encouraged within healthcare settings in particular, and society in general. Therefore, it was noted that sensitizing students is critical to ensure that they feel comfortable talking about the sexual health and sexual needs of patients upon entering clinical practice. Health professionals also indicated a need to revisit educational curricula to ensure that adequate content is included on sexual health and counseling. They also highlighted that theoretical education should be supplemented with adequate hands-on training opportunities for students on the delivery of sexual counseling. One health professional discussed why sexual counseling should be better incorporated into students’ training.
Sexual counseling should be included in courses such as nursing, physiotherapy, pharmacy, doctors [cardiologists] and MBBS, so that students know that sexual counseling is very important, and complex diseases patients have these problems… and even heart patients are important. Students will feel comfortable, aware of sexual counselling in clinical practice, and can ask patients’ questions confidently. (Physiotherapist, Male)
Regarding continuing education on sexual health and counselling, health professionals emphasized the importance of mentorship of novice and junior professionals. They noted that mentors should prepare novice professionals in sexual health needs assessment, planning, and counselling approaches to foster their confidence, enhance their skill set, and offer them real-life practice opportunities to offer counseling to patients in need.
At a personal level, senior to junior [mentorship] education is required in hospital, as we are trained about diet, exercise, education, and treatment. So, there should be classes for staff first on this topic [sexual health] and then training on how to approach patients and how to educate them about sexual contact, also guidelines around sexual counseling. This training and education are important so that when we talk to patients our words and sentences are clear, our concepts are clear, and we are clear in what and how we should communicate to patients. (Registered Nurse, Female)
Activate Organizational Level Action Plan to Support Health Professionals in the Effective Provision of Sexual Counseling
Health professionals highlighted that for effective delivery of sexual counselling to patients’ healthcare organizations should provide adequate support and resources to frontline care professionals. They emphasized the need to activate an action plan to address structural and practice-level gaps that limit healthcare professionals’ capacity to deliver sexual counseling. They highlighted the need of structural and organizational changes such as private space, combating taboo surrounding discussion of sexual health within healthcare system, funding to change infrastructure for sexual health counseling sessions. Health professionals noted that delivery of comprehensive sexual health counselling is a collaborative endeavor including many team players such as patients, front-line health professionals, and the organization.
In my view, whenever you want to improve your practice or enhance your standards, organizations should take responsibility for it. At the organizational level, healthcare professionals and organizational leaders should consult and plan regular meetings to discuss sexual health issues and what could be done to improve delivery of sexual health care and counseling. (Registered Nurse, Female)
When highlighting structural gaps within their organizations, health professionals raised concerns about limited private space to offer sexual counseling, as well as a lack of trained mentors and health professionals as outlined above. They indicated that there should be a sexual health referral system with specialized units for sexual counseling for patients in need. Therefore, financial resources should be provided for ensuring the availability of advanced and digitalized services and virtual counseling sessions. Health professionals noted that since sexual health is a private matter and patients are often reluctant to talk about these issues, it is critical to have space devoted to offering these services.
Having a specialized department will give opportunities to all patients who need sexual counseling. Patients will also not feel shy about going there because they would know that there are other people who also have similar issues, and this is a normal thing to ask about. In addition, patients should have opportunities to talk over the phone with health professionals. If a patient cannot come to hospital, he/she can approach healthcare professionals remotely. (Registered Nurse, Female)
In addition to structural changes, health professionals indicated that more concrete and actionable steps must be taken to ensure that sexual counseling is delivered to patients. They emphasized the need for mandatory sexual health needs assessment and discharge teaching, development and implementation of assessment forms and checklists for cardiology units, and provision of clinical practice guidelines to health professionals on how to offer effective sexual health counseling.
We need to ask patients and explore their sexual needs, sexual history, and current sexual issues through mandatory assessments. In addition, when a patient is going to be discharged, sexual education and counseling should be part of the post-operative teaching booklet. Healthcare professionals should explain to patients in detail and use dummies to demonstrate the best positions for sex after surgeries. Also, patients should summarize what they learned and if they are confident before they are discharged from the hospital. Compulsory sexual education should be part of discharge teaching. (Cardiologist, Male)
Discussion
This first qualitative study in a setting where sex is particularly taboo and sex and gender inequality is high, revealed healthcare professionals need culturally sensitive and person-centered training and institutional support for the delivery of sexual counseling to cardiac patients. 31 Healthcare professionals perceived it imperative to target gaps in patients’ sexual health knowledge, as well as gaps in the provision of sexual assessment and psychoeducation through a multi-level approach. Organizations should play a pivotal role in creating conducive environments to support healthcare professionals in the effective provision of sexual counseling.
For effective delivery and receipt of sexual counseling, foremost is that both healthcare providers and patients feel comfortable while they interact and discuss sexual health and related issues. In almost all societies, discussion about sexual health is not common and people feel shy or uncomfortable to discuss such issues. Indeed, in a study of European cardiologists, the findings revealed that cardiologists do not discuss sexuality in their routine practice and more than 70% of cardiologists never recommend patients resuming sexual activity after myocardial infarction. In addition, 63% of cardiologists acknowledged having trained health professionals to refer patients for sexual assessment, counseling, and treatment. 19
One of the strategies that healthcare professionals recognized as valuable and practical was their training, including promoting open discussion of sexual health and related issues with patients. The training should be embedded in health professions curriculum so that these professionals are sensitized to sexual health content. However, the training should be sensitive to the needs of healthcare professionals as well as prepare them to be sensitive to the needs of their patients. In addition, scenario-based practical education, using clinical case studies, experiential learning approaches, and simulated experience can assist them in learning how to interact with patients in a professional and culturally sensitive manner while navigating sociocultural mores. 13 Health organizations should facilitate opportunities for continuous education through conferences, workshops, and continuing educational courses.
The significance of health professionals’ training for enhancing the delivery of sexual counseling to cardiac patients is well-reported in the literature. Mc Sharry et al. 8 developed interventions to change healthcare professionals’ behavior to promote sexual counseling in cardiac patients. These authors recognized that a lack of knowledge of sexual health problems among health professionals and the absence of sexual counseling guidelines are major barriers to providing sexual counseling. To overcome such barriers, the first step is to educate healthcare professionals regarding the significance of sexual counseling and sensitize them to sexual content while they are receiving their professional training. 8 Training through demonstration and real-world practice can be effective. The use of videos, delivering sexual counseling through demonstration and role plays, and evidence-based checklists and guidelines can be useful training resources.1,8
Providers perceived that organizations need to take responsibility and create favorable environments where both healthcare professionals and patients feel comfortable discussing sexual health problems. At the unit level, the availability of a private place for sexual health assessment and counseling can promote delivery. A separate dedicated sexual health and counseling department with trained professionals is essential, so providers can refer their patients when needed. Professionals at the bedside can request a consultation with these experts for comprehensive assessment and effective sexual health counseling. Cardiac rehabilitation can also be an important setting for sexual health assessment and counseling.32,33 The Cardiac Health and Relationship Management and Sexuality (CHARMS) intervention may be a useful model. In their guideline, Steinke and Jaarsma 7 discussed practical approaches for sexual counseling of cardiac patients, and their recommendations should be implemented. RCTs are also needed to assess culturally-sensitive sexual counseling interventions in the cardiac context. 34
Where applicable and consensual, given the plethora of issues related not only to those outlined in the introduction but also to cardiac medications and devices, comorbidities such as depression or anxiety, as well as cardiac complications of sexually-transmitted infections, cardiac patients should expect sexual discussion as a normal part of their recovery process. Patients must have adequate awareness of how sexual health problems are exacerbated by cardiovascular disease and their consequences. 35
Sociocultural factors such as sexism, sexual taboos, patients and health professionals discomfort, and lack of confidence in healthcare professionals to initiate sexual discussions are constraints and can be addressed via patient and provider education. Further research is warranted to develop and test interventions considering patients’ sociocultural and religious values in various contexts and settings. Issues of history of sexual violence, sexual consent, sexual mutuality, and diversity in sex/gender, as well as bias related to age among other factors should be considered.
Limitations
Representative generalizability is not established through qualitative research, so while rigorous sampling was used and saturation was achieved, the applicability of these findings to other settings cannot be known. Indeed, the study sample consisted of South Asian healthcare professionals, where the sociosexual context is likely different than in other jurisdictions. The sample comprised of healthcare professionals from only two cities in Pakistan. Therefore, the transferability of study findings to rural or other socioeconomically diverse settings in Pakistan is limited.
Conclusion
Sexual health is essential for psychological and relational well-being and promotes cardiovascular health, yet cardiac patients rarely undergo sexual assessment and face barriers in receiving effective sexual counseling. Healthcare professionals perceive that several strategies can be implemented to overcome those barriers to promulgate the efficient delivery of sexual counseling to cardiac patients. Sexual health education of professionals across relevant disciplines, structural changes to support healthcare professionals in sexual counseling, provision of sexual health assessment checklists, tools, and practice guidelines, patient awareness and education through continuous community awareness campaigns, and providing written sexual health education material in local languages are potential strategies. Health organizations need to take the initiative to develop and implement individual and professional strategies based on their available resources to promote sexual health counseling of cardiac patient which will ultimately improve their sexual quality of life and overall health. As discussion about sexuality is considered a taboo, it is critical that healthcare professionals are trained to delivery culturally sensitive care to patients who may not be comfortable discussing this topic.
Footnotes
Authors’ Contribution
SI, AY, and FA designed the study.
SI and IA helped in data collection.
SI and AY analyzed data.SI, AD, FA, IA, and SG supervised the study.
SI, AY, and AD helped in manuscript writing.
FA and SG were involved in critical revisions for important intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Research ethics approval for the study was obtained from the review committee of Riphah International University, Islamabad, Pakistan (Riphah/IIMC/IRC/23/3042).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed Consent
All participants signed written informed consent.