
Abstract
Objectives:
Sex education continues to be inconsistently provided across the United States, with many states not even requiring that sex education be medically accurate. One population at high risk of experiencing the consequences of poor sex education is college students. The current study sought to assess the self-derived “sex facts” that college students feel they know.
Methodology:
Twenty college students were asked to name five things about sex, sexuality, sexual health, sexual behavior, sexual identity, or sexual anatomy that they were 100% sure were true, yielding a total of 96 answers for analysis.
Results:
Approximately 56% of their answers were true. The highest proportion of true answers was related to sexual identity topics (74%), while the lowest proportion (20%) was related to sensuality topics. The sexuality education implications of these results are discussed in detail.
Introduction
Sex education in the United States is not frequently described as progressive.1,2 Sex education is not universally required in K-12 education across the United States, and many states that do require it still opt to provide to students abstinence-based sex education, including several states that do not require that the sex education in their state be medically accurate.3,4 Additionally, the teachers who lead sex education discussions often lack the training and competency to do so effectively.5,6 When schools do offer sex education, parents often have the option of removing their children from having access to that education, a privilege rarely available for any other course or educational content. 7 In fact, one study 8 discovered that the common reasons parents chose to opt their children out of school-based sex education were personal biases or misunderstandings of sexological science. This leaves children and young adults across the United States ill-equipped to navigate the landscape of their own sexual health and wellness, having little to no reliable school-based information upon which to base their sexual decision-making.
The quality of sex education information these children and young adults receive at home may be equally problematic. For some, parents may avoid having any conversations about sex altogether. 9 When there are sexual health conversations occurring in the home, these conversations can be rife with inaccurate and/or stigmatizing language.10,11 For children and teenagers not receiving reliable sex education from their schools or from their parents or guardians, they turn to their peers and to the media for guidance.12-14 While peers can sometimes provide a more nonjudgmental atmosphere to discuss questions surrounding sex, their lack of accurate education and experience can lead to the transmission of incorrect and harmful information. 15 Equally problematic, learning about sex through media has been associated with reinforcing stereotypical gender roles, lower self-esteem in females, and little to no focus on safe sex.16,17
With no real systemic influences to correct sexual misinformation in the United States, a negative cycle is perpetuated, as those who received little to no sex education grow up and relay what they think they know about sex to their children through a process of intergenerational transmission. Intergenerational transmission is the process by which familial values, norms, knowledge, and beliefs are communicated to and instilled in the next generation, both explicitly and tacitly. 18 This means that the next generation must begin their lifelong journey of self-discovery from a point of origin roughly proximal to the previous generation. New values, norms, knowledge, and beliefs are only gained by straying from this point of origin. Intergenerational transmission has been evidenced in the conveying of sexuality-related norms, including gender roles, marital aggression, and attachment styles.19-21 It has also been responsible for the passing of more concrete knowledge between generations, including beliefs of whether climate change exists or not and anxiety regarding one’s ability to do math.22,23 This suggests that intergenerational transmission of sexual health knowledge is probable, meaning that young adults’ only hope for gaining accurate sexual health knowledge is to stray from this familial point of origin.
One such opportunity for young adults to stray from their familial point of origin is college. Congruent with the Life Course Health Development Model and the Input-Environment-Output Model,24-26 college represents a significant “turning point” in the health trajectory of a person’s life. The input of pre-college intergenerational transmission of sexual health knowledge can, during college years, be heavily influenced by the higher education environment, an environment in which young adults are often met with their first real opportunity to apply and test their knowledge independently.24,27 In a recent scoping review by Cassidy et al. 28 on the sexual health knowledge of college students, all of the studies used a direct measure of knowledge, usually a narrowly defined knowledge test/quiz of some kind. Although this approach does accurately assess knowledge (or lack thereof), it does so only with respect to the content predetermined to be important by the researcher (e.g., HIV, contraception). This ignores two important factors: (a) sexuality is a broad domain of health encompassing numerous facets of health and wellness, and (b) the role of self-efficacy in knowledge (i.e., self-derived sexual health knowledge).
The aim of the current study is to address this gap, serving as the first known study to elicit self-derived sexual health knowledge from college students. This study will do so by asking college students to recall any facts about sexuality that they are sure are true, thus inviting maximum self-efficacy in their answers and allowing for the broadest possible definition of sexuality. The Circles of Sexuality Model,
29
one such model presenting a comprehensive definition of sexuality, presents sexuality as having five constituent parts: (a) Intimacy, (b) Sensuality, (c) Sexual Identity, (d) Sexual Health and Behavior, and (e) Sexualization. The purpose of this model is to concretize the comprehensive definition of sexuality used by sex educators, sex therapists, and sex researchers.30,31 Such an approach is congruent with the World Health Organization
32
definition of sexuality as:
a central aspect of being human throughout life that encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction. Sexuality is experienced and expressed in thoughts, fantasies, desires, beliefs, attitudes, values, behaviours, practices, roles and relationships. While sexuality can include all of these dimensions, not all of them are always experienced or expressed.
Methods
Participants
Participants were recruited during the Spring 2021 semester at a public university in Florida. Flyers advertising the study were distributed online, in hallways, and via classroom announcements by faculty. The participants were required to be undergraduate students over the age of 18 and to have access to a webcam for the interview. There was no incentive for participating in the study. In all, 20 participants were recruited for the study. Seventy-five percent of participants were between 18 and 24 years old and 25% were between 25 and 39 years old; 75% identified as female, 15% identified as male, and 10% identified as genderqueer; 75% identified as straight, and 15% identified as gay, bisexual, queer, or questioning; and 62% identified as White, 14% identified as Black or African American, 5% identified as Asian, 14% identified as Hispanic or Latino, and 5% reported that their identity was not on the list and did not specify further.
Procedure
Participants, after completing the informed consent, scheduled their virtual interview via an online scheduling service and used an alias (i.e., each participant was asked to use the name of their favorite book/movie/TV character). They were then provided with the Zoom link to save for when their interview time arrived. At the time of the scheduled interview, the participant would join the Zoom interview with one of the authors. During the interview, the interviewer confirmed the alias, asked for the demographics reported above, and asked the participant, “What are FIVE things about sex, sexuality, sexual health, sexual behavior, sexual identity, or sexual anatomy that you are 100% sure are true? These can be anything that you may have heard, learned, been told, been taught, or discovered over the years. Take your time.” No further prompt or clarification was provided. If a participant asked for clarification, the question above was simply repeated. The interviewer entered the participant’s answers into a Qualtrics survey verbatim. This Qualtrics survey consisted of a series of five open-ended text boxes designed to allow enough space to capture the participants’ answers in full. The interview was not recorded and lasted approximately 7 min on average. Past research has used a similar single-question verbatim transcription approach.33,34
Data Coding and Analysis
Coders
The first three authors served as the data coders. The first author is a licensed mental health counselor, counselor education faculty member, and certified sex therapist. The second author is a counselor-in-training who completed a graduate course in sexual issues in counseling. The third author is a postgraduate student enrolled in a counseling sexology certificate program. All three coders operate from a sex-positive and medically accurate framework.
Coding and Analysis
Though each participant was encouraged to provide five answers, if they stated that they could not think of any additional answers, the interview was ended. Seventeen (85%) of participants provided five answers, two (10%) provided four answers, and one (5%) provided three answers. A total of 96 answers were recorded. The first three authors then met to review each answer. Using a consensus approach, each statement was identified as representing one of the circles of sexuality, 29 using operational definitions outlined in Table 1. This process identified 44 answers (45.8%) related to Sexual Health & Behavior, 27 answers (28.1%) related to Sexual Identity, 14 answers (14.6%) related to Sexualization, six answers (6.2%) related to intimacy, and five answers (5.2%) related to Sensuality. This approach is congruent with deductive summative content analysis.35,36
Operational Definitions Used for Circles of Sexuality.
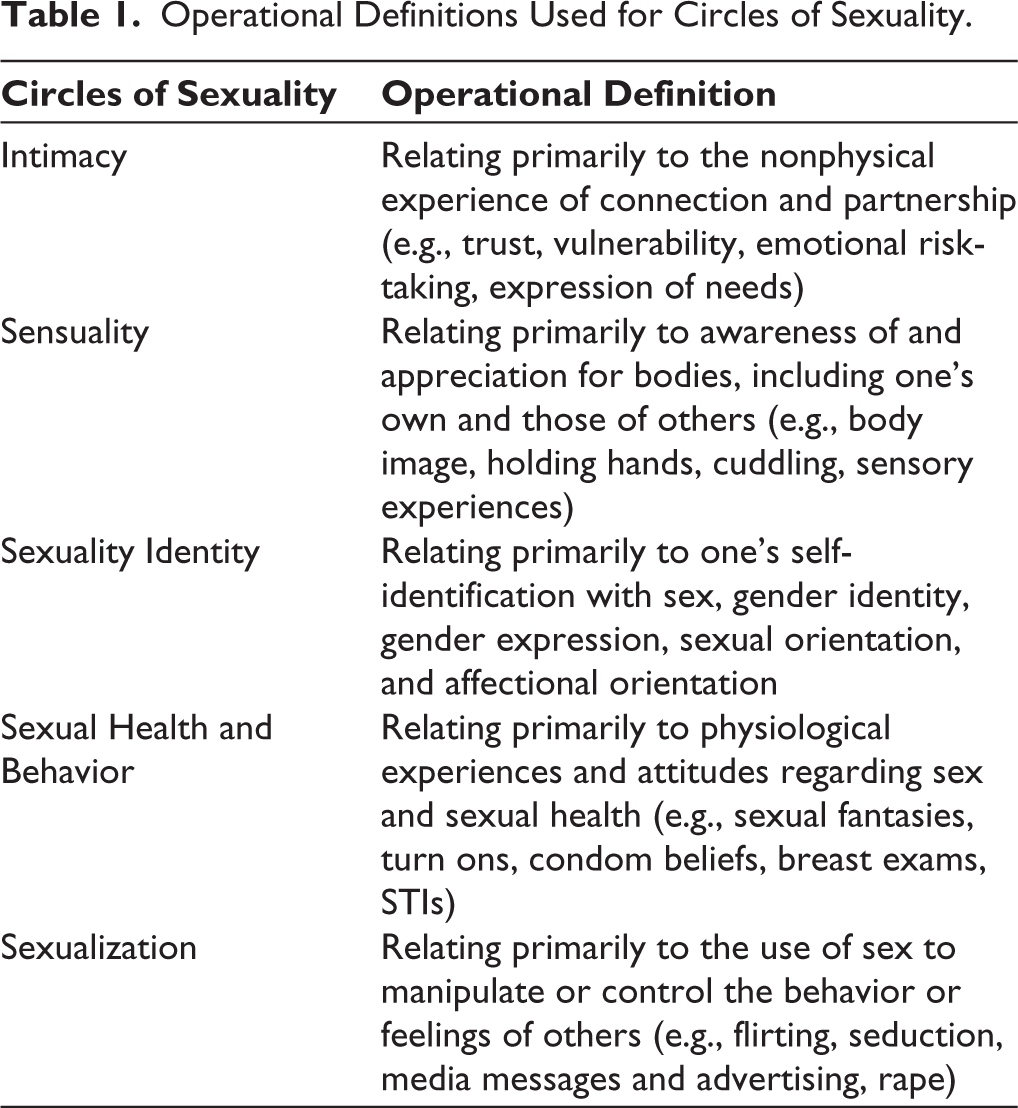
The first three authors then independently reviewed each answer for accuracy. They coded each answer as Completely True, Completely False, Opinion, or Incomplete/Partial using these operational definitions (example answers have been included in parentheses):
Completely True: A preponderance of extant research has shown this to be consistently true (Pulling out does not prevent pregnancy). Completely False: Little to no extant research shows this to be true, or a preponderance of extant research has shown this to be consistently false (There are three genders, female, male and intersex). Opinion: No pragmatic way for science/research to demonstrate the truth or falseness of the statement (Sexual health testing should be accessible to everyone). Incomplete/Partial: The statement has some parts that are true but also contains either inaccuracies and/or opinion (Contraception can save your life).
If two or more of the reviewers assigned the same code, that answer was labeled accordingly. If the reviewers did not agree on a code, a consensus approach was used, wherein each reviewer discussed their rationale for their assigned code. Because of the opportunity for the first author’s code to sway the conversation due to their position as senior author, they offered their code and rationale last. This process is congruent with deductive summative content analysis procedures.35,36 Between the three coders, Fleiss’ kappa was computed as 0.54, which considered moderate inter-rater reliability.37,38
Results
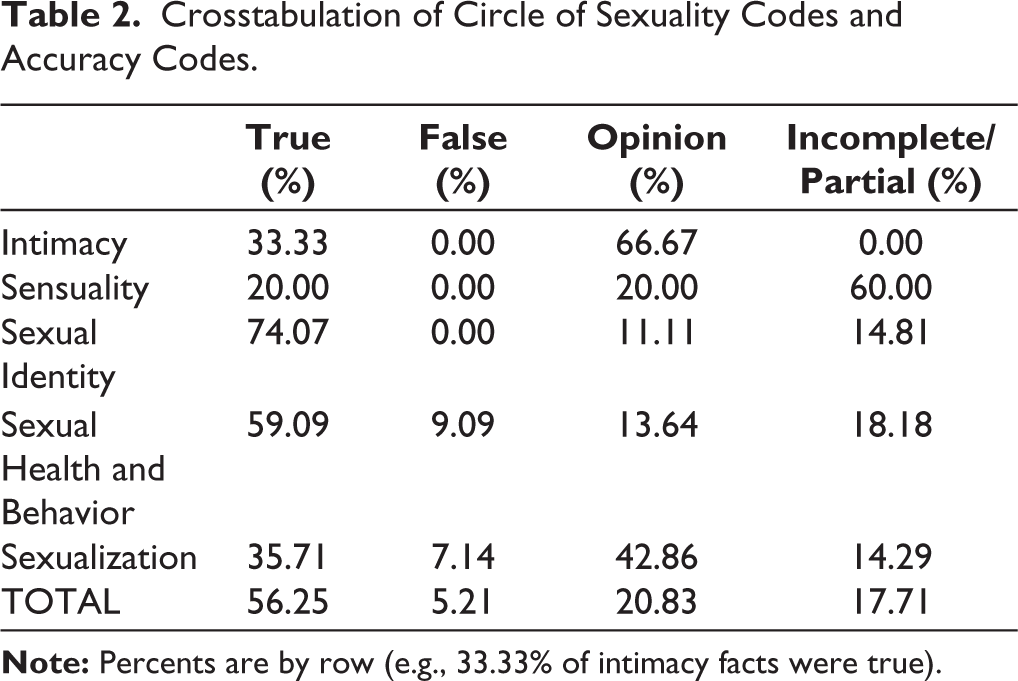
A crosstabulation of the data was conducted using SPSS, with the circle of sexuality codes as rows and the accuracy codes as columns (see Table 2). Of the 96 answers, 56.2% (n = 54) were coded as Completely True, 20.8% (n = 20) were coded as Opinion, 17.7% (n = 17) were coded as Incomplete/Partial, and 5.2% (n = 5) were coded as Completely False. In the end, each answer was assigned both a circle of sexuality code and an accuracy code. The highest proportion of Completely True answers was in the Sexual Identity domain (74%, n = 20) while the lowest proportion (20%, n = 1) was in the Sensuality domain. Completely False answers were only present in the Sexual Health and Behavior domain (9%, n = 4) and in the Sexualization domain (7%, n = 1). Opinion answers were most prevalent in the Intimacy domain (67%, n = 4) and least prevalent in the Sexual Identity domain (11%, n = 3). The Sensuality domain had the highest proportion of Incomplete/Partial answers (60%, n = 3), while the Sexualization domain had the lowest proportion of such (14%, n = 2).
Crosstabulation of Circle of Sexuality Codes and Accuracy Codes.
Discussion
Overall Accuracy
When asked to provide 100% accurate facts about sex, college students were successful in doing so only 56% of the time. In other words, roughly half of the sexual health facts that college students in the sample believed to be true were not. This is a worrisome statistic, especially considering that one’s perceived knowledge is one of the factors most heavily weighed when making health-related decisions. 39 There is clearly still much work to be done in (a) educating young adults on sexual health matters and (b) helping young adults reflect on and identify when their “knowledge” may be inaccurate.
Despite that only 56% of the facts were completely true, there is some reassurance in the fact that only 5% of participants’ answers were completely false, meaning that students are 10 times more likely to be right rather than entirely wrong. This does mean that roughly 40% of answers were something neither right nor wrong, which is discussed below, but it offers a not altogether bleak picture of the extent to which college students are making sexual health decisions based on completely wrong information. Put another way, nearly 95% of facts believed to be true by college students are not incorrect, and thus 95% of the knowledge being used by college students to make sexual health decisions is more or less valid. Considering the sizable body of literature showing that college students regularly engage in risky sexual behavior,40,41 have poor sexual health habits,42,43 and perpetuate sexual stigmatization,44,45 the current study would suggest that the ignorance catalyzing these poor outcomes seems extremely narrow but deeply profound. This makes for a confined yet resolute target for sex education efforts.
Opinions
Approximately 21% of the answers provided by participants were opinions. This suggests that much of sex knowledge is subjective. What is important to keep in mind is that participants were asked to provide facts about sex that they felt were 100% true; in approximately one-fifth of cases, they offered a personal opinion about sex. This, perhaps more than anything, shows that college students are less than adept at properly distinguishing fact/science from opinion/values on the topic of sex. Though the opinion may be valid and prosocial (e.g., sexual health testing should be accessible to everyone), it is incapable of being addressed with the scientific precision and rigor necessary to be called a true fact. As mentioned earlier, this calls attention to a significant need for sex education efforts to intentionally include methods by which young adults can continuously engage in a process of introspection to discern fact from opinion.46,47
An important derivative of this, however, is the recognition that sex educators have no jurisdiction over young adults’ sexual values. Having opinions about sex is not an issue; it is believing them to be fact that gives rise to problems. For example, it is imprudent for a sex educator to challenge the belief that masturbation is a sin (an opinion), but entirely appropriate for them to remediate the belief that it is unhealthy (a falsehood). Escaping the politicization (and therefore values-based thinking) regarding sex seems to be unlikely, as Foucault 48 wrote extensively on the social problemization of sex dating back centuries. It therefore seems to be a better use of time and skill for sex educators to intentionally teach students to use their opinions to guide sexual decision-making, thus better arming the students with a more comprehensive and valid decision-making process to utilize when the time comes. By doing so, though the opinions are unlikely to change at their core, they may become less likely to be masqueraded as truth, and therefore to a lesser degree interfere with fact-based decision-making.
Incorrect Answers
Though limited in number, 100% of the Completely False statements were in the Sexualization and Sexual Health and Behavior circles of sexuality. The overlap of these two circles is also where conversations surrounding consent would likely fall, given that consent is a process of negotiating what sexual behaviors will and will not be part of a sexual encounter. This would therefore include the constituent topics of sexual behavior, how sexuality is used and interpreted, and what constitutes safe and consensual sex. It is therefore alarming that all of the false answers provided by the participants would fall squarely at this intersection. This may be a partial explanation for the rampant confusion surrounding consent among college students.49,50 Given the overall small number of false answers, the ability to opine much further here is limited. However, there is a strong indication that college students are most frequently wrong about sex when being clear matters most. This is an opportunity for future research to explore more deeply and for sex educators to tackle aggressively.
Disproportionate Opinions in Sexualization
The sexualization circle evidenced twice as many opinion answers (43%) as the average (21%). This, again, is despite the prompt being to offer facts about sex that the participant was 100% sure were true. Some of this result may be the natural outcome of the subjectivity baked into the definition of sexualization, a definition that uses the words “manipulation,” “objectifying,” and “exploitative.”30,31,51 The sense of being manipulated, exploited, or objectified is an intrapersonal and subjective experience.52,53 This subjectivity can give rise to sexual health knowledge within this circle being more densely packed with values-based answers than would occur in the other domains.
However, it seems prudent to also consider an equally likely alternative explanation, one rooted in power differentials. One such notable power differential in US culture at present is that existing between the genders. The power to decide what is and is not sexualization often rests with men. 54 As Loughnan et al. 55 noted, “sexualized women are objectified through a denial of moral concern, and this reduced moral concern is linked to increased victim blame and tacitly reduced perceived victim suffering” (p. 459). The present study may offer some explanation for how such reduced moral concern begins: an overabundance of opinions cloaked as fact within the sexualization circle of sexuality. This is an important area for future research to elucidate more clearly, so as to fully equip sex educators to address this issue.
Partially True About Sensuality
Approximately 60% of the answers in the sensuality circle were coded as partially true, more than 3.3 times the average rate of partially true answers (17.71%). This was most frequently the result of a statement being physiologically true, but also containing some presumptive language (e.g., sex (intercourse) should not hurt). Though the example statement has physiological truth on the face of it, for those in the kink community, there may be an intentional attempt to introduce pain into the sexual encounter.56,57 Answers like this may evidence a fundamental conflict between physiological reality and personal values. This suggests a politicization of the body, whereby the body itself is offered the refuge of science, but the activity of that body is cast out into a value-laden wilderness. 58 College students appear to be ill-prepared to reconcile the interpersonal and intrapersonal dialectic of sensuality. As such, the present study may offer a preliminary justification for sex educators to speak candidly and specifically about both the physiological appreciation for bodies and the emotional awareness of the agency and autonomy of the owner of the body.
Intimacy is Personal
Over two-thirds of the answers categorized as intimacy-related were opinions (67%), and the rest (33%) were completely true. This means that none of the intimacy-related answers were identified as being even partially false. This is the only domain of the Circles of Sexuality Model 29 for which this happened, indicating a unique quality of intimacy as it relates to sexual health knowledge. It would seem that either (a) college students are incredibly well-versed in the science related to intimacy, or (b) intimacy does not lend itself well to objectively verifiable facts at all. Given college students’ history of poor sexual health knowledge,28,58 odds favor the latter hypothesis. Intimacy is a multifaceted concept that is as idiosyncratic as it is complex31,60 and may be difficult to scientifically quantify for that reason. It is the most intangible of the circles, occurring entirely on the emotional and intrapersonal level. As such, it seems incredibly difficult to say that any stated “fact” about intimacy is verifiably false. As an extension of this, it is no wonder that 67% of intimacy statements were opinions, the highest such rate by 50%. Intimacy, the present study would suggest, seems to be the most endogenous of all domains of sexuality, as defined by Dailey. 29 Sex educators may want to note this as they prepare for and deliver their lessons. It may be a fool’s errand to teach people what intimacy is or is not; it is perhaps better to invite people to explore and articulate what their level and type of intimacy needs are. 61
Dubious Truth of Sexual Identity
It seems hopeful that nearly 75% of answers related to sexual identity were true, and that these answers recognized the growing science around the biopsychosocial components of sexual identity.62,63 However, this promising result could be due to either a biased sample and/or participants succumbing to demand characteristics and providing answers that, although true, they did not personally believe. In either case, nonetheless, it does suggest that verifiable truths related to sexual identity are easily recalled by college students. This could be the result of increasing visibility and conversation about sexual identities, particularly among young adults, including on social media platforms like Tumblr 64 and TikTok. 65 White et al. 66 found that 35% of high school students in their sample identified as a sexual or gender minority. The proportion of the population that engages in nonheterosexual sexual behavior may be even higher than the proportion that identifies as a sexual or gender minority.67,68 With a relatively high number of sexual and gender minority young adults gaining increasing visibility and accessing wider social networks, the results of the present study are hopefully further evidence of a natural progression toward an attitude of inclusivity among college students. At the very least, it suggests that college students are familiar with inclusive language, even if they only feign endorsement. This familiarity can be leveraged by sex educators. Already, sex educators are on the front lines of combating homophobia and stigma by teaching and reinforcing inclusive language, and it seems to be sticking. Continued efforts in this venture may prove fruitful in creating—even at worst pseudo-genuine—culture and climate where such language is normalized and typical, ultimately overpowering language of hate, discrimination, and exclusion.
Limitations
The present analysis should only be read in proper context with respect to its limitations. First, the sample was drawn from only one college in the coastal Southeast. Though the study specifically sought to understand the “sex knowledge” of college students, a less homogeneous sample would have been ideal. Future research can easily address this limitation. Relatedly, the sample was primarily White. Future research should address this by meeting the growing call for a more concerted, sex-positive, and non-stigmatizing inquiry into the sex and pleasure of Black and other communities of color. 69 The sample size was also on the lower side, but the number of overall answers (n = 96) was still sizable enough to achieve the aim of the study. Finally, the operationalizations of the Circles of Sexuality are often inconsistent in the literature. This inconsistency does increase the chance of imprecision when using them as the coding source. Nonetheless, the present study achieved its aim of investigating the self-derived sex knowledge of college students.
Implications for Sex Therapists
Florida is the only state that statutorily protects the title “sex therapist.” As such, there may be a unique opportunity for Florida sex therapists to serve as providers of medically accurate, non-stigmatizing sexual health information. College students consistently experience sexual issues and report that sex therapists and counselors are the most likely helping professionals from whom they would seek help for these issues, second only to physicians.70-73 As such, the present study yields several considerations for sex therapists and other mental health professions working with college students. Sex therapists often utilize the PLISSIT model 74 to approach the treatment of sexual challenges presented by clients. Although Limited Information from the PLISSIT model was initially encouraged to be “limited,” the findings of this study suggest a potential need to assist clients with more comprehensive sex education by integrating factual sexual knowledge in tandem with exploring how the client came to understand themselves as sexual beings in relation to their knowledge and opinions of specific sexual interactions, sexual health, and interpersonal relationships. Upon exploring the sexual narrative of the client, sex therapists might be more apt to identify any potential thinking errors surrounding what is fact or not, and what is consensual or not, when it comes to the client’s sexual story and how they navigate sexual discourse and interactions with others. Additionally, sex therapists can call attention to and provide education regarding the role of opinion in sexual decision-making, sexual scripts, and sexual behavior. Therapists can give clients the Permission to state and explore their opinions on sexual issues and then provide evidence-based Limited Information to help contextualize the client’s opinions. Finally, sex therapists can reinforce for clients the deeply personal and idiosyncratic experience of intimacy, helping to normalize clients’ subjective experiences of unmet needs, isolation, and confusion around intimacy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the University of North Florida Institutional Review Board (1717665-1) on March 1, 2021.
Informed Consent
The participant has consented to the submission of the article to the journal.