
Abstract
Couvade syndrome occurs when expectant fathers experience psychological and somatic symptoms typical of pregnancy. Common somatic symptoms include gastrointestinal problems, toothache, heartburn, fatigue and back pain, while anxiety is the most commonly reported psychological symptom. Symptoms typically manifest during the first trimester of the partner’s pregnancy, decrease or disappear during the second trimester, increase during the third trimester, and usually resolve after delivery.
The aetiology of Couvade’s syndrome remains unclear, with psychoanalytic theories suggesting paternal anxiety and feelings of marginalisation. Hormonal changes, including increased cortisol, estradiol, prolactin and decreased testosterone levels during the third trimester, are also thought to be contributing factors. The prevalence varies widely, from 11% to 97%, depending on the population studied.
Despite its reported prevalence, research into Couvade’s syndrome is limited, especially studies involving closely related women with similar symptoms. The findings highlight the need for further research to better understand this phenomenon and its impact on family dynamics during pregnancy.
Introduction
False pregnancy is a condition in which a woman believes she is pregnant, despite the absence of physical symptoms and confirmation of the condition by medical tests.1-3 When a woman develops typical physical symptoms of pregnancy without the presence of a foetus, the condition is called pseudocyesis.1-3
In cases where a man who is expecting a child develops psychological (without believing he is pregnant, as this would be delusional) and physical symptoms typical of pregnancy, the condition is called sympathetic pregnancy or Couvade’s syndrome. 1 The first descriptions of this syndrome appeared in the medical literature in the 1950s and 1960s, referring to transient gastrointestinal symptoms in soldiers around the time of the suspected birth of their children.4,5
Couvade’s syndrome manifests in a variety of ways, with symptoms ranging from subtle, such as nausea or toothache, to more obvious, such as significant weight gain.6-8 These symptoms typically appear in the first trimester of the partner’s pregnancy, subside in the second trimester, reappear in the third trimester and disappear completely after the birth. 8 The syndrome appears to be common in all populations, often in more subtle forms.5,8 Despite its intriguing nature and the passage of time, the phenomenon remains poorly understood, with limited research and literature available.
Objective
The aim of this article is to discuss various aspects of Couvade’s syndrome based on the available literature, with particular emphasis on recent publications.
Materials and Methods
A search of the PubMed database was performed to identify scientific articles containing the terms ‘couvade syndrome’, ‘couvade’ or ‘sympathetic pregnancy’ in the title, abstract or keywords. This search yielded 63 articles, of which those published in English with free full-text access were included for further analysis.
Diagnostic Criteria, Symptomatology and Course of Couvade Syndrome
There are currently no official diagnostic criteria for Couvade syndrome. As a result, scientific studies rely on questionnaires developed by research teams studying the condition. It is important to note that the classification of Couvade syndrome remains controversial. Some researchers consider it to be a psychosomatic disorder, while others consider it to be a physiological response to hormonal changes in the partners of pregnant women.6,8
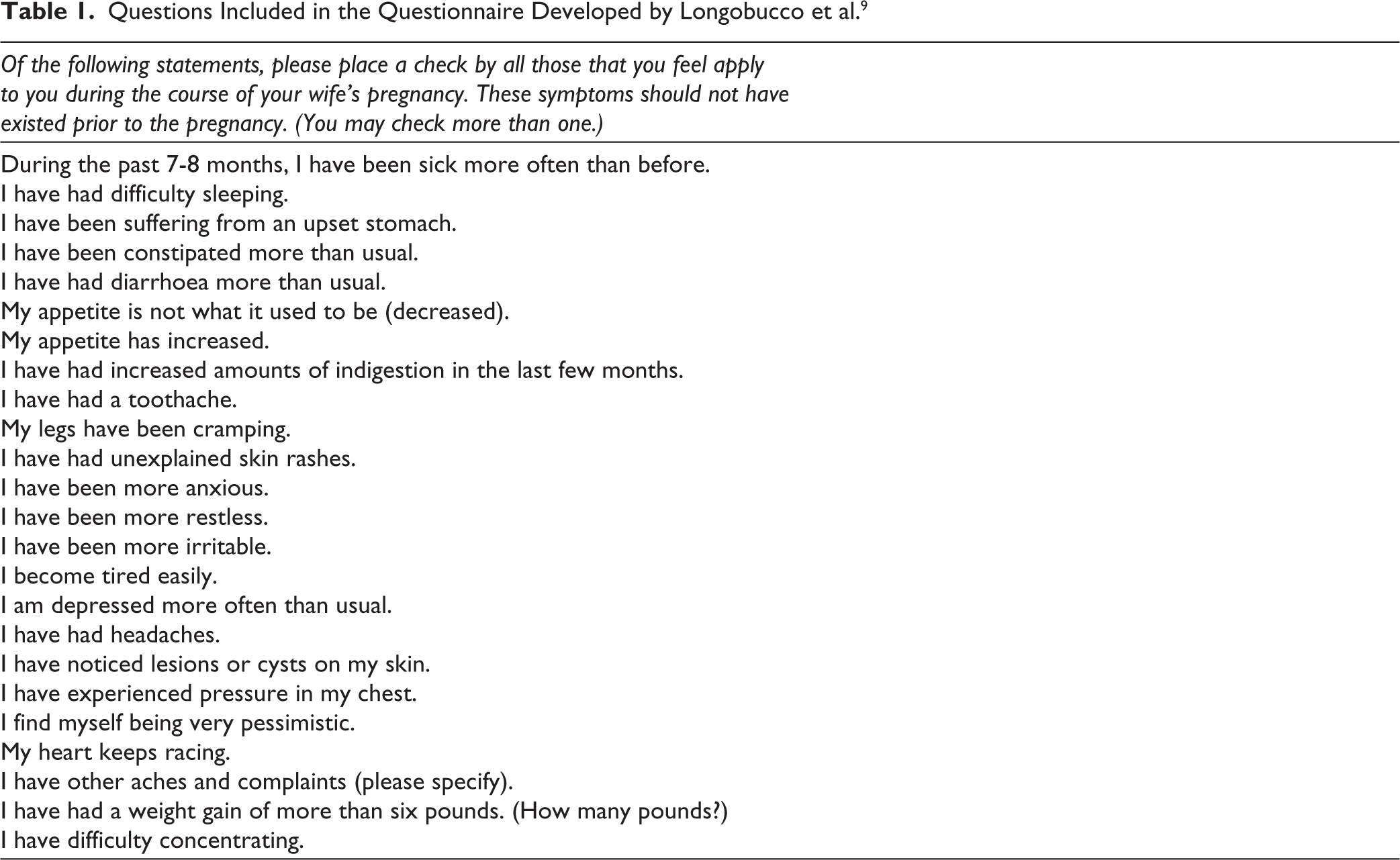
One of the first questionnaires dealing with this phenomenon was developed by Longobucco et al. 9 It consists of 24 questions relating to symptoms commonly associated with Couvade’s syndrome. The questions included in the questionnaire developed by these researchers are presented in Table 1. The presence of at least two symptoms is sufficient for diagnosis.
Questions Included in the Questionnaire Developed by Longobucco et al. 9
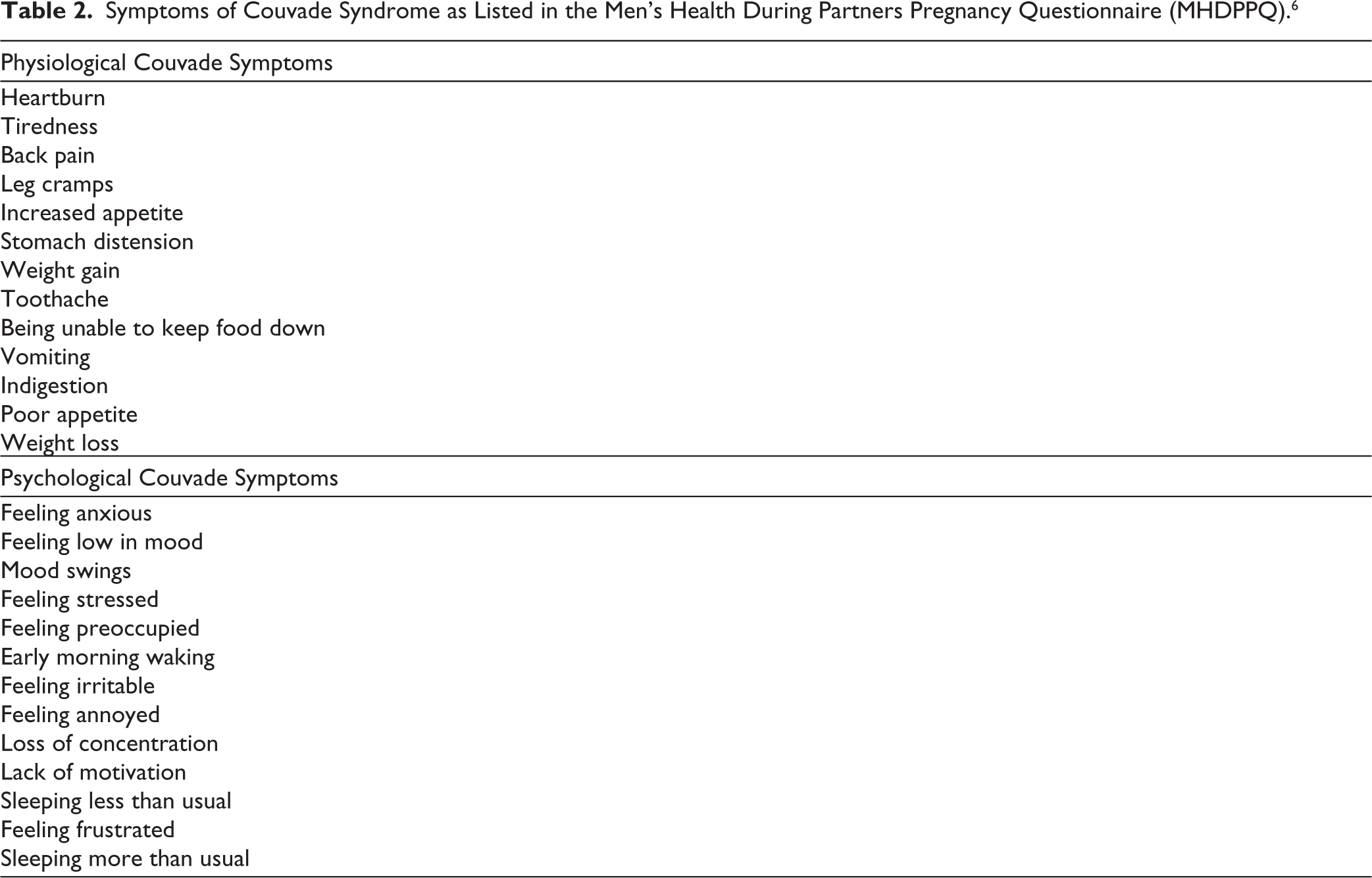
One of the more recent and commonly used tools in the study of Couvade’s syndrome is the Men’s Health During Partners Pregnancy Questionnaire (MHDPPQ), developed by Brennan. 10 Originally consisting of 35 questions, the questionnaire was refined during its validation process, resulting in the removal of 9 items. 10 The presence of at least 8 symptoms listed in this questionnaire within the last 3 months is sufficient to diagnose Couvade’s syndrome. 10 The questions included in the questionnaire developed by these researchers are presented in Table 2.
Symptoms of Couvade Syndrome as Listed in the Men’s Health During Partners Pregnancy Questionnaire (MHDPPQ). 6
It is noteworthy that although many of the questions in the cited diagnostic questionnaires overlap, they also differ in some respects. The MHDPPQ appears to be a superior diagnostic tool, due to the wider range of symptoms it covers and the validation carried out by its author.6,9,10 Although there are other questionnaires related to Couvade syndrome, the authors of this article do not consider it necessary to refer to them all in this discussion.
The aforementioned questionnaires provide a robust framework for describing the typical symptoms of Couvade syndrome.6,9-15 Consequently, this discussion will now focus on the prevalence of these symptoms.
According to the first studies on Couvade syndrome, 5 the most common symptoms were nausea, loss of appetite and dental pain. More recent studies have confirmed these findings, identifying gastrointestinal symptoms and dental pain as the most common somatic manifestations, while anxiety remains the most common psychological symptom. 8
However, Mrayan et al. 6 reported slightly different findings in a study of 449 married men whose partners were in at least the second trimester of pregnancy. Their findings provide additional insight into the variability and complexity of symptom prevalence in Couvade syndrome.
In this study, heartburn, fatigue and back pain were identified as the main somatic symptoms, while anxiety remained the predominant psychological symptom. Different results were found in studies of Polish and Finnish populations. In Poland, the most common somatic symptom was weight gain, accompanied by mood swings as the primary psychological symptom. Conversely, in Finland, the predominant somatic symptom was also weight gain, but nervousness was the predominant psychological problem. 15
Although the specific symptoms of Couvade’s syndrome vary, the course of the disease appears to be consistent between individuals.1,5,8 Symptoms typically appear during the first trimester of the partner’s pregnancy, subside or disappear during the second trimester, reappear with increased intensity during the third trimester, and finally resolve after or shortly after delivery.1,5,8
Interestingly, a case study by Thippaiah et al. 16 described symptoms characteristic of Couvade syndrome that recurred cyclically in a woman during each of her daughter’s pregnancies. Further evidence was provided by a review by Chase et al. 8 which suggested that Couvade syndrome may also develop in women who are emotionally attached to a pregnant woman or even to a man who is expecting a child. These observations challenge the traditional definition of Couvade’s syndrome as a phenomenon affecting only men awaiting fatherhood. 5
Suspected Aetiology of Couvade Syndrome
Early studies suggested that Couvade’s syndrome arises from a man’s anxiety about pregnancy, which contributes to the development of somatic symptoms.5,17 Currently, its occurrence is explained by a combination of psychoanalytic theories and hormonal changes in men whose partners are pregnant.5,8,17
Psychoanalytic theories attribute the syndrome to factors such as paternal anxiety, feelings of alienation during pregnancy, the man’s level of involvement in the pregnancy (which correlates with the incidence of Couvade’s syndrome), and the perception of the child as a rival for the partner’s attention.5,8,17,18
Research has identified significant hormonal changes in expectant fathers, particularly during the third trimester and just before delivery. These include increased levels of cortisol, oestradiol and prolactin, and decreased levels of testosterone.8,19 These changes are thought to prepare men to care for their offspring. Notably, men with more symptoms of Couvade’s syndrome also have more pronounced changes in prolactin and testosterone levels.8,19
Finally, certain cultural practices involve ritual behaviours associated with Couvade syndrome, in which expectant fathers deliberately imitate behaviours typical of pregnant women. 20
Prevalence of Couvade Syndrome
Early studies suggested that mild forms of Couvade’s syndrome are relatively common. 5 For example, a study by Curtis 21 reported that 22 out of 35 (63%) expectant fathers experienced transient gastrointestinal symptoms during their partner’s pregnancy. Another study of 327 married men expecting a child and a control group of 221 non-expectant men found that subtle symptoms of Couvade’s syndrome (e.g., nausea, toothache, loss of appetite) were more common in the expectant group (57%) than in the control group (46%). 5
It is currently believed that Couvade’s syndrome affects men of all racial and socio-economic groups. However, some studies suggest a higher prevalence in ethnic minorities and in men who are unmarried or have not planned a pregnancy.8,17 According to Brennan et al. the prevalence of the syndrome ranges from 11% to 97%, depending on the society studied. 17
Specific prevalence rates include approximately 60% in a Jordanian population, 6 72% in Polish men 14 and 61% in a Thai cohort. 22 In contrast, lower prevalence rates have been reported in Sweden (20%), the United Kingdom (25%), Australia (31%) and the United States (25%-52%).6,10,23
The considerable variation in prevalence between societies is likely to be due to cultural differences, such as the degree of male involvement in pregnancy, and to differences in the diagnostic criteria used in different studies. These factors significantly influence reported rates and highlight the need for standardised diagnostic approaches.
Summary
Couvade’s syndrome, also known as sympathetic pregnancy, describes the occurrence of psychological and somatic symptoms in expectant fathers during their partner’s pregnancy. The condition is often diagnosed using the MHDPPQ, which uses a minimum of eight symptoms experienced in the previous three months as diagnostic criteria. Symptoms are categorised as physiological (e.g., gastrointestinal problems, toothache, heartburn, fatigue and back pain) and psychological (e.g., anxiety).
The syndrome typically begins in the first trimester, subsides in the second trimester, reappears in the third trimester, and disappears after or shortly after childbirth. The aetiology of the condition may include paternal anxiety, perceived marginalisation during pregnancy, or hormonal changes, including increased levels of cortisol, estradiol and prolactin, and decreased levels of testosterone, particularly in the third trimester.
The prevalence of Couvade’s syndrome varies widely, from 11% to 97%, depending on the population studied. Despite its high prevalence, research into the syndrome remains scarce. In addition, there is limited research on similar symptoms in women closely related to pregnant individuals. This gap highlights the need for more comprehensive studies to better understand the condition and its implications.
Couvade syndrome has practical implications, particularly in terms of family dynamics and the role of the father during pregnancy. Affected fathers often show increased attentiveness to their partner’s needs and help to facilitate communication with medical professionals, particularly during labour. In some cases, however, the syndrome can lead to increased self-absorption and stress, which may affect their ability to provide empathic support to the mother. 14
Given its impact on both the individual and the family as a whole, incorporating screening for Couvade syndrome into antenatal and postnatal care could help identify fathers who may benefit from specialised support. Educating expectant fathers about the syndrome and its symptoms will enable them to better understand and manage their experience, ultimately fostering a stronger and more supportive family environment.
Footnotes
Author Contributions
All authors equally contributed to the conception and design of the study, literature search, its analysis, and the preparation of the first draft of the manuscript. K. W. reviewed the draft, made necessary corrections, and approved its final version for submission to the journal. All authors read and approved the final manuscript.
Consent to Participate
Not applicable.
Consent to Publish
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.