
Abstract
Objectives:
There is a significant gap in evidence regarding the health-seeking behaviour of short-distance drivers (SDDs) traveling less than 800 km in a single direction within India, resulting in an absence of healthcare programmes or interventions specifically designed for this group. This exploratory qualitative assessment was conducted to understand the experiences and perceptions of SDDs regarding health services available for human immunodeficiency virus (HIV).
Methods:
In-depth interviews were conducted in 2022 with 86 primary and 118 secondary participants from nine states in India. The interviews were conducted in five different languages. Two separate interview guides were developed: one for primary participants (including drivers) and another for secondary participants (such as government officials, programme officials and nongovernment organisation [NGO] representatives). Purposive sampling was employed to select secondary participants, while primary participants were identified through snowball sampling. Data analysis was carried out using thematic analysis, identifying key themes and patterns from the transcripts. ATLAS.ti (version 8) software was used for data analysis.
Results:
The SDDs did not have knowledge of any HIV prevention or care services accounting for their working environment and hours. The results showed that financial problems, poor management of healthcare services, lack of knowledge regarding the available services and quality of care at public healthcare facilities were major barriers to accessing care for HIV/AIDS. The perceived risk of infection did not translate into seeking testing for HIV. Stigma emerged as an important factor that deterred testing as well as treatment for HIV/AIDS. The secondary participants mentioned that the targeted interventions had limited engagement with short-distance drivers due to a lack of specific focus on this group.
Conclusion:
This study highlights the need for tailored HIV prevention and care programmes for SDDs, who face unique barriers such as financial constraints, stigma and limited healthcare access. It emphasises the importance of integrating this group into national strategies to improve awareness, reduce stigma and promote regular testing.
Introduction
The HIV (human immunodeficiency virus) is a chronic viral infection that attacks and weakens the immune system of the host, and when left untreated leads to the acquired immunodeficiency syndrome (AIDS). An estimated 38.4 million (33.9-43.8 million) people worldwide were living with HIV (PLHIV) and 650,000 (510,000-860,000) of those individuals died from the virus in 2021. 1 The Joint United Nations Program on HIV/AIDS (UNAIDS) has set an ambitious target code named 90-90-90, which aims to ensure that 90% of all PLHIV are diagnosed, 90% of all people diagnosed will receive sustained antiretroviral therapy (ART) and 90% of those on therapy will have viral suppression by 2020. These treatment targets have been revised to 95-95-95 for 2030. 2 India has the third-highest absolute burden of HIV in the world with an estimated 2.3 million PLHIV in 2021—of which 63 thousand were newly infected—and 42,000 annual fatalities linked to the virus. Additionally, only 77% of PLHIV were aware of their diagnosis and 65% of PLHIV were started on ART. 3
The spread of HIV is usually heightened by the transmission of the virus among populations with high-risk behaviour. These include workers in the transport sector whose occupation, difficult work environment and poor economic and living conditions make them vulnerable to an increased risk of acquiring HIV infections. 4 Transport drivers are known to be the ‘bridge’ for the spread of HIV or sexually transmitted infection (STI) to the general population through their sexual interaction with the core group (high-risk sex workers). The pattern of transmission from transport drivers to their wives and other sex workers has been observed in India.5,6 Against this background, the National AIDS Control Organisation (NACO) provides prevention, testing and treatment services for truck drivers through targeted-intervention (TI) projects. Despite the provision of dedicated healthcare services, studies in India have documented poor accessibility of these services for long-distance truck drivers. 7 Even though HIV prevention interventions have been focused on truckers in India since 1996, a study in the state of Andhra Pradesh found that truckers on an average made only 2.2 contacts annually with these programmes. 8
While traditionally research from the 1990s in several low- and middle-income countries (LMICs) identified truck drivers as the at-risk bridge population in the transport sector,9-11 the rapid urban expansion and growth in India, with penetration of technology, have transformed the mobility landscape over the years. Research in Nigeria found that commercial taxi and bus drivers are at high risk of HIV infection and transmission, and that immediate interventions are needed to prevent HIV transmission among drivers and their partners. 12 A study in Ethiopia found considerable risky sexual behaviour among taxi drivers and their assistants. 13 Another study in Brazil found that short haul truck drivers (travel less than 50 km) were vulnerable to the sexual transmission of HIV/AIDS primarily due to inconsistent use of condoms. 14 A study in India found that helpers, cleaners, rickshaw, taxi and bus drivers who visited sex workers had similar high-risk sexual behaviours and prevalence of HIV and other STIs as compared to truck drivers. 15 The short-distance drivers, such as taxi and auto-rickshaw drivers, are continuously mobile through the day and night. They may also exhibit high-risk behaviour since they ferry female sex workers and their clients, and therefore, visit red light areas of the city. 16
The high prevalence of HIV in high-risk groups or important populations is one of the current drivers of the HIV epidemic that threatens to undermine the success narrative. In India, taxi and auto drivers have incorrect knowledge of the treatment options available for HIV/AIDS. 17 While there have been studies indicating high-risk sexual behaviour among short-distance drivers, it is not clear how this sub-population perceives the support rendered to them with regard to HIV and AIDS prevention and treatment strategies. To our knowledge, the study participants, short-distance drivers (less than 800 km), have not been the target of HIV prevention programmes or government-led TIs in the study settings as well as in India. This exploratory qualitative study examined participant experiences and perceptions on the existing HIV interventions and services with the goal of identifying and prioritising barriers and improving programme performance.
Methods
Study Setting
This exploratory qualitative study was conducted in 11 cities in nine states strategically chosen in consultation with the State AIDS Control Society (SACS) and District AIDS Prevention and Control Unit (DAPCU) officials (Table 1). These cities, representing various regions, were hubs of transportation activity, ensuring a diverse representation of drivers and their health-seeking behaviour.
Study Sites.
Study Population
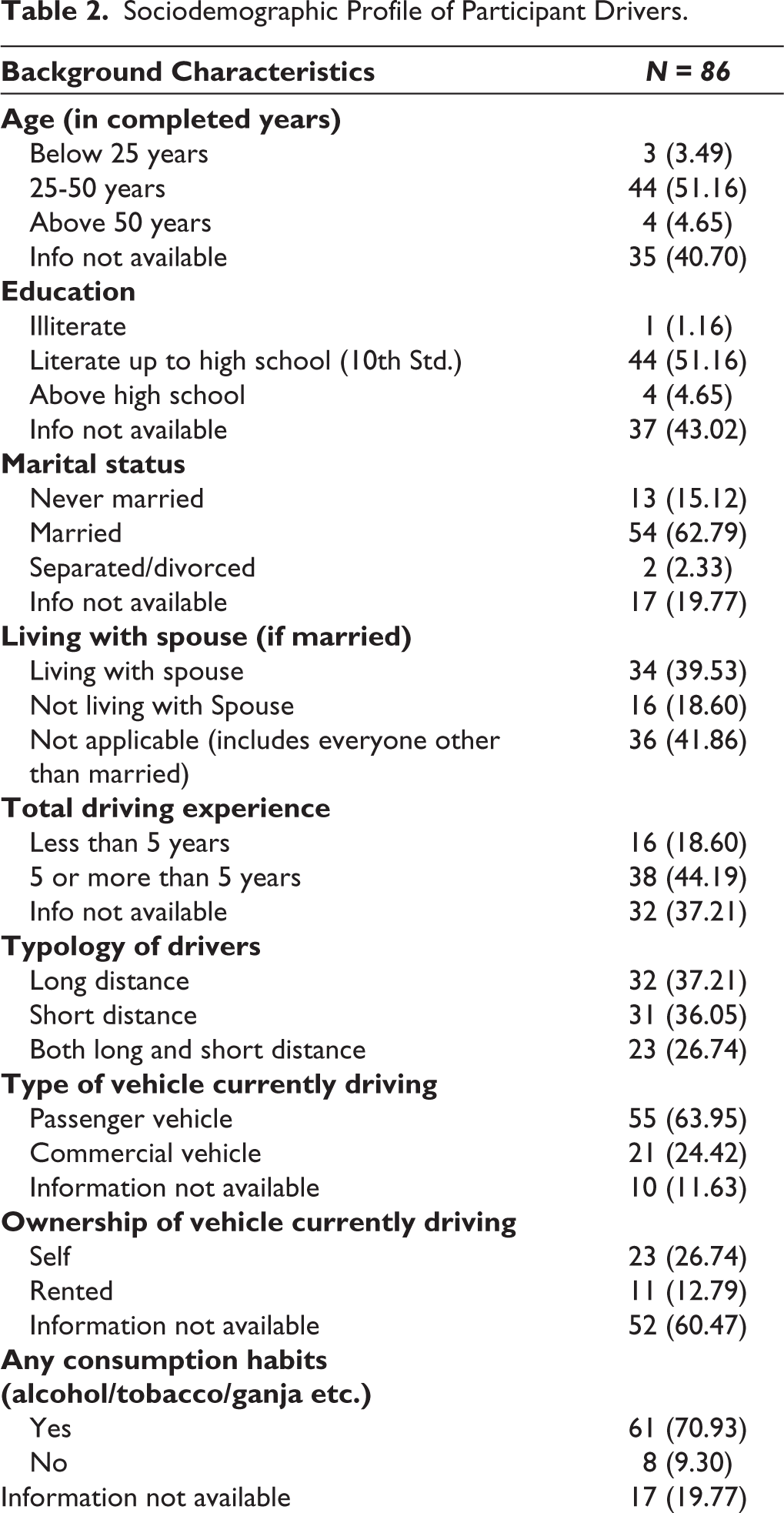
The study participants included primary (this study interested to understanding primary participants risky sexual behaviour) and secondary participants (secondary participants have idea about primary participants risky sexual behaviour). Primary participants were transportation sector workers (cart pullers, e-rickshaw pullers, tractor drivers, mini truck drivers, bus drivers, toto drivers, ola/uber drivers, delivery drivers, pedal rickshaw driver, auto driver and allied population which includes helper, cleaner and operators) (Table 2), while the secondary participants included government officials: SACS Project Director/Deputy Director/Joint Director Targeted Intervention (TI)/Assistant Director TI, Program officer/Monitoring & Evaluation Officer, Technical support unit, nongovernment organisation (NGOs) TIs/ICTC councillors. We used purposive sampling technique for selection of secondary respondents and snowball sampling to select the primary study participants.
Sociodemographic Profile of Participant Drivers.
Data Collection
In-depth interviews were conducted with 204 study participants in various regional languages by post-graduate level field investigators from social science backgrounds (MSW) from October 2022 to December 2022. The field investigators were trained by the authors and had been involved in conducting qualitative research studies. Separate interview guides were developed for interviewing primary and secondary participants. Short-distance drivers who stopped at their respective city junctions were approached individually and invited to participate in the study. After explaining the purpose of the study, those who provided consent for the interview were taken to a separate area to maintain privacy and confidentiality, and assured that their identity and information given would be kept confidential. The topics covered in the interview guides included access to and utilisation of healthcare services for HIV/AIDS, knowledge, attitudes and practices of drivers and helpers. The guides were first prepared in English and were then translated into regional languages (Hindi, Telugu, Tamil, Punjabi, Marathi) as were to be conducted across different states of India where natives spoke different languages. The interviews were recorded and audiotaped after the consent of the participants, and some field notes were also made by the members of the data collection teams. Each interview with the participants lasted for around 45-90 minutes approximately. The audiotaped interviews were transcribed verbatim first into the local language and then translated to English. Transcripts were read several times before developing a coding system. Next, all transcripts were coded using the code-book definitions. A thematic analysis of the transcripts was carried out to analyse the data and find themes or patterns. Two researchers (SL, AK) were involved in coding of the data. ATLAS.ti (version 8) software was used for data analysis.
Ethical Considerations
The study received ethical approval from the Ethics Committee of the National AIDS Control Organisation. Ethical issues were discussed comprehensively with all persons involved in the study. The entire research team was sensitised to ethical issues and given suitable training prior to the commencement of the study. The data collectors were trained on the importance of voluntary choice and participation and sensitised to issues of privacy and confidentiality. Each participant was informed about the nature and scope of the study and given any additional information sought by them. Every participant was requested to provide their written consent before the data collection was begun. Illiterate participants put their thumb impressions on the consent form. The information collected was kept confidential in the custody of the principle investigators (PIs) and site research officer. On completion of the study, all documents pertaining to the study, including consent forms, filled survey instruments, transcripts and translated documents, were couriered to Tata Institute of Social Sciences for the preservation for three years from completion.
Results
Availability of HIV/AIDS Interventions for Short-distance Drivers
In the secondary respondents’ interviews, participants were asked about the availability of HIV TIs for short-distance drivers. The majority of respondents indicated that the HIV interventions were present for long-distance drivers and short-distance drivers had very low contact with such TIs.
Based upon the definition of NACO mainly we are targeting the long-distance truckers only those who are loading and unloading, mainly in the harbours, ports and those who are frequently using the highway for transit, there will be given the top preference. (DD SACS, TN)
The participants reported that they did not consider short-distance drivers as an important sub-population in their interventions. Many experiences of drivers also reflected the focus of TIs on long-distance truck drivers.
If a short-distance driver comes, he will be served but our focus is on our long-distance drivers. (NGO official, MP)
I saw another camp which was set up in the middle of the truck drivers there were many truck drivers who were showing whatever problem they were telling. I was getting down so I saw a little but I did not hear what’s going on there. (Auto driver, Rajasthan)
Some of the drivers indicated that while they were aware of occasional HIV camps held for the general public, they did not have contact with HIV/AIDS interventions and activities held specially for drivers.
I have heard that the government gives free condoms and there are free checkups but I have never been there. (Auto driver, Punjab)
(HIV prevention camp) It is there in government hospital, medical college and bus-stand. I have seen these camps but not attended (Taxi driver, TN)
Health-seeking Behaviour of Short-distance Drivers
The short-distance drivers described visiting unqualified medical practitioners as the first point of seeking care.
First, we go to small doctors(quack). If nothing happens, we go to a qualified doctor and to other doctors when referred to. (Rickshaw driver, West Bengal)
Drivers preferred obtaining general medicines from pharmacies and resorted to check-ups with doctors only in case of significant health problems.
General illness is pharmacy, if heavy fever than we go to doctors. (Taxi driver, Assam)
These people think that if there is a slight infection, they just don’t go anywhere and just in case something happens, they go to the local doctor and get themselves treated, nothing more than that. (App-based driver, MP)
For services specific to HIV and AIDS, the majority of drivers sought care in government hospitals. Very few drivers were in contact with outreach services in the community or AIDS-specific TIs.
I have been to a government hospital many times and get my self-tested. (Truck Driver, Maharashtra)
The drivers recognised the benefits of getting services at camps specially set-up for them. However, they also mentioned the reluctance to visit such camps for testing and treatment.
In the camp that the investigation is done quickly. We don’t need to go to the hospital every time. The facility is also good in the camp but people don’t like to go to a camp. (Taxi driver, MP)
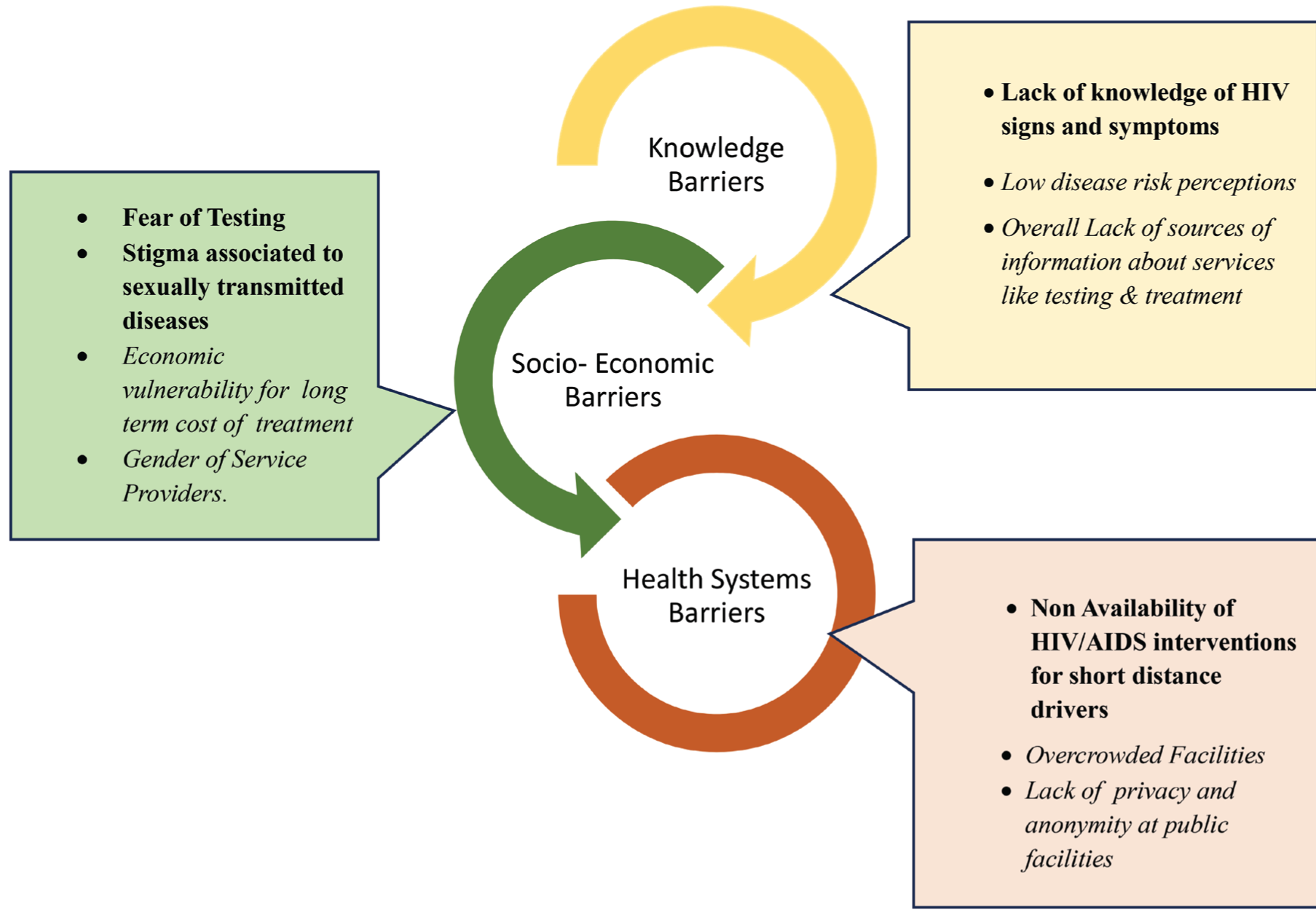
The results from the study is summarised as barriers to accessing HIV services for short-distance drivers in India fall into three domains: knowledge barriers, including lack of awareness and misconceptions about services; socio-economic barriers, such as stigma, fear, economic vulnerability and lack of privacy; and health system barriers, including the absence of targeted interventions and overcrowded facilities. These interconnected barriers highlight the need for tailored strategies to enhance access to HIV services for this population (Figure 1)
Access Barriers to HIV Related Health Services amongst Short Distance Drivers.
Barriers to Testing
Lack of Knowledge of HIV Testing Facilities
The short-distance drivers did not have comprehensive knowledge about the HIV infection. The drivers were aware of services being provided at government hospitals for all. Many reported being unaware of voluntary testing and counselling camps which were set up specially for drivers.
It is done in government hospital and it happens somewhere else, I don’t know the information. (E-rickshaw driver, New Delhi)
Some drivers who were aware of HIV/AIDS camps reported observing a decline in the number of such camps in recent years.
Previously, we had had AIDS camps at Khalpara. But now the numbers have dropped rapidly. (Toto driver, WB)
I just know about the eye treatment and other camps only. I don’t know about the other camps. I have not seen the (HIV/AIDS) camps for a long time. (Tempo matador driver, WB)
Fear of Testing
Due to anticipated stigma, the majority of short-distance drivers preferred to avoid getting tested. The lack of knowledge about the various ways in which the spread of HIV/AIDS can occur contributed to attitudes fearful of testing for AIDS. For example, drivers associated a positive test result with an established behaviour pattern of visiting sex workers as illustrated in the following quote.
No, I did not get any test done. I am scared that someone may come to know that I visit a sex worker. (Rickshaw driver, Punjab)
What If we are found positive, then what will everyone say, what will the family members say. (City bus driver, MP)
The fear of consequences of a positive HIV test deterred the drivers from getting themselves tested.
There is no point in holding a medical camp because we are afraid that if we come to know, then it is better that we die anyway. There is a kind of fear inside if I come to know. if I get married tomorrow, then my wife will get it, my children will get it, because of me two lives are getting ruined. (Rapido bike driver, Maharashtra)
Inadequate or Incorrect Perceptions
Many participant drivers were unaware of the services and emphasised the absence of measures to address these knowledge gaps.
They don’t have any idea whom to contact or sometimes they feel shy to inform. (App-based driver, Rajasthan)
Low self-perception of HIV risk, despite drivers being involved in high-risk sexual relationships, was a key reason for their unwillingness to undergo HIV testing.
No, I never got it (testing) done. I mostly have sex without condom nothing happened to me, I am standing in front of you healthy. (Auto driver, Punjab)
The drivers were of the opinion that testing was not a requirement for them and was needed only when severe or persistent symptoms of AIDS became evident.
When the person starts drying up, he gets the test done, then he will know and he will get the treatment. (JCB driver, Punjab)
I have tested once, and got negative result. So, I get more confidence and since then I have not faced any sex-related issues. (Toto driver, WB)
Barriers that Impact Utilisation of Healthcare Services
Lack of Knowledge of Services
The short-distance drivers did not receive any support, including information from the government. The drivers mentioned having limited avenues to gain knowledge regarding prevention and treatment for HIV. They mentioned a decline in the HIV/AIDS activities over the years.
Nobody is giving us any information, only we on our interest learning few things from others that’s all. Especially for drivers no one is giving any information regarding anything. I haven’t seen any awareness programs for drivers, once upon a time in the year of 1999, 2000 there was some programs but now nowhere its happening. Those times when HIV started there was few programs conducted in the form of dramas and TV as well but now no one talk about it, even govt or any other people are not talking about it. At least for 1-2 months no one has come, not even for year we get any awareness program. (Taxi driver, Karnataka)
Economic Vulnerability
The limited availability of free ART medications for short-distance drivers emerged from the interviews. This led to financial problems for accessing treatment and care for HIV/AIDS.
They do not give all medicines. I had to buy as per prescriptions. But as we are poor, this is really very tough for us to buy such costly medicines. (Sumo driver, WB)
Stigma
HIV/AIDS-related stigma was rampant among short-distance drivers in the settings where the study was conducted. The fear of stigmatising and discriminating attitudes of others towards the person diagnosed with HIV as well as family members discouraged them from seeking treatment. Dissatisfaction with the public healthcare system also emerged during the interviews. The following excerpts indicate these findings
HIV patients fear seeking health services because they worry that disclosing their status could lead to social stigma, including being treated poorly by society, neighbors, or even their own family members. This fear works to the advantage of government workers, who believe that HIV patients will not openly request the services or benefits available to them. (Taxi driver, Karnataka) The reason for this is people don’t have money, don’t have right information, don’t know whom to show, other than this some people feel ashamed that what people will think that he goes to have sex with another woman. And this may also be the reason that he is not comfortable talking about this disease openly with the doctor and family members. (E-Rickshaw driver, Punjab) There is a lack of time, there is a feeling of fear, the world is busy, they are shy, so they do not go, there are many problems, and no one wants to discuss the sexually transmitted disease when it takes a big form. (Bus driver, MP) If you talk about me, I will die but will not tell anything to anyone. (Bus conductor, Punjab)
Drivers preferred attending general healthcare camps rather than those specifically for AIDS due to the stigma associated with the disease.
When they come to know whose camp has been set up, if AIDS was set up, then there will be no people in the name of AIDS ready to go, but they go when the eyes check-up camp is been set there, they do not go to the camp after hearing the name of AIDS. (App-based driver, MP)
Management of Healthcare Services
Concerns about privacy were noted from the participants. Drivers felt that sufficient privacy was not maintained at government facilities. The organisation of healthcare services for HIV did not account for the stigma associated with the disease, leading to hesitancy in accessing these services.
There is a separate department of HIV in the government hospital. There is a line of HIV people. So many people come there for cold, fever, minor treatment, then they see people with HIV/AIDS, then they will tell the people of the locality. (App-based driver, Maharashtra)
There is only one government hospital in my area Shatabdi where medicines for HIV are available. There it is written in big letters ART, I will sit under there to get the medicine. People will see that you are sitting here taking medicines, do you have HIV? They will tell more people in my area so sitting with me will stop. (Rapido driver, Maharashtra)
No matter how much someone says, there is no such thing as privacy in a government hospital, it is a very useless situation. (App-based driver, MP)
Gender of Healthcare Providers
The dominance of males in the driving profession coupled with misconceptions regarding the process of testing or availing treatment for HIV/AIDS makes it difficult for male drivers to access services from female physicians or female health workers. This indicates the need to include education of drivers regarding the testing and treatment procedure as a part of interventions in order to reduce gender as a barrier to testing.
The HIV test team comes inside this parking lot. Doctor are ladies and the ones who sit at the counter are also ladies. But the driver man here does not like to go to that doctor woman because of shame. There are many illiterate people in the driving line, very few educated people. They believe that they will remove the clothes, hold the penis in the hand, get the test done. Many people know that they have HIV, but how can they tell in front of the ladies. (Travels driver, Maharashtra)
Quality of Care
The shortage of healthcare personnel for treatment in government hospitals led to challenges in accessing care from these facilities. This also resulted in many seeking care from private healthcare facilities.
Govt hospitals are good but there will be doctor for 100 patients likewise there will be only 1 nurse for 50 patients but in private there will be one nurse for every 5–10 patients so they treat well. (Taxi driver, Karnataka)
They give no supply in govt. nothing is there, what we want we don’t get, emergency and costly medicine are not available in medical college and govt. hospital, there is nothing. (E rickshaw driver, Assam)
The participants described how the service providers treated them as a negative reason to avail treatment. They reported unacceptable or hostile behaviour when visiting government healthcare facilities.
Doctors don’t talk properly, it seems like we have taken a loan from them, they don’t behave well. (Mini truck driver, New Delhi)
Overcrowded Healthcare Facilities
Drivers led very busy lives with strict schedules operating according to their employers. In such cases, long waiting hours to avail healthcare services make it difficult for them to visit government facilities. Long waiting times impacted drivers’ livelihoods and served as barriers to utilising healthcare services.
I am a driver and our work should be done quickly that’s why I prefer to go private. (Rickshaw puller, Delhi)
Mostly there is a long queue and there you have to be in a queue to get the treatment done. If your number does not come, then one has to go again the next day. (City bus driver, MP)
Discussion
To the best of our knowledge, this qualitative study is one of the first few studies among short-distance drivers in nine states of India that explored challenges around seeking healthcare for HIV/AIDS. The participant short-distance drivers did not have knowledge of any HIV prevention or care services that were available for them taking their working environment and hours into consideration. The results showed that financial problems, poor management of healthcare services, lack of knowledge regarding the available services, quality of care at public healthcare facilities were major barriers to accessing care for HIV/AIDS. The drivers in this study despite engaging in risky sexual activities did not feel the need to be tested regularly. The perceived risk of infection also did not translate into seeking testing for HIV. Stigma emerged as an important factor that deterred testing as well as treatment for HIV/AIDS.
Studies in LMICs including India suggest that local transportation workers such as short-distance drivers are engaged in high-risk sexual behaviour.13,16,18 The studies suggest that these drivers need more attention in relation to control and prevention of the spread of HIV and AIDS. In our study, the low visibility of current programmes for HIV was highlighted. Some drivers were aware of the existing HIV prevention and treatment strategies in the form of medical camps. However, all such camps were aimed at the general public or directed at long-distance truck drivers and they were not recipients of such services. A study with short-distance drivers in South Africa also found that minibus taxi drivers were aware of the HIV prevention strategies aimed at the general public and that their work as taxi drivers made it difficult for them to participate. 19 Similar to the findings of a study in Ethiopia, 13 in this study, the official authorities working for the control of spread of HIV/AIDS had limited information on short-distance drivers and hence, failed to consider this sub-population as a high-risk group for national interventions.
Our study showed that the short-distance drivers are primary beneficiaries of HIV/AIDS treatment services at government hospitals and they have very less knowledge of HIV and TIs or outreach activities. In a study in Uganda, people accessing care for HIV/AIDS at health facilities reported a need for more outreach and home-based services in their treatment. 20 Although HIV services are available free of cost at government hospitals in India, they were not easily accessible to the drivers. The schedules and work hours of the participant drivers made it difficult for them to avail services at government hospitals. They described problems such as long queues and prolonged waiting time at these facilities that impacted their employment and livelihoods. These health systems level barriers have also been identified in previous studies as challenges for accessing HIV care. 21 In a recent study in 2019 conducted in Pune district, Maharashtra, the loss of privacy and breach of confidentiality when visiting government hospitals for HIV testing had been reported as concerns by truck drivers. These drivers preferred testing at Khushi clinics-dedicated clinics at trans-shipment locations or along the highway to reduce the spread of HIV and other STIs in truck drivers. 22 No such initiatives were available for short-distance drivers, further hampering their access to HIV care services.
In our study, many drivers avoided testing because they perceived getting tested as an acknowledgement of engaging with sex workers. It has been found that individuals who undergo HIV testing are stigmatised, because they are considered guilty of ‘immoral’ behaviours. 21
Regular testing has been strongly advised for high-risk groups that engage in risky sexual activities. Early testing of HIV can help individuals who test positive to take action to receive care, support and treatment in advance of symptoms showing up, which can significantly extend life and avert health issues in the long-term. 23 Studies have also shown that infected persons who are aware of their positive HIV status decrease behaviours associated with transmission of the disease. 24 A systematic review on sexual behaviour change following HIV testing services found positive modifications in behaviour immediately following an HIV positive test. 25 Furthermore, such behaviour changes in the early stages after diagnosis can lower the risk of transmission to HIV-uninfected partners. 25
The fear of being stigmatised and subjected to discrimination because of using HIV testing services or being HIV positive was evident from the findings of this study. Many studies with truck drivers as well as taxi drivers have reported fear or stigma impacting the uptake of HIV testing and treatment services.19,22,26 The fear of rejection by society and even by close family members has been documented earlier. 27 The fear of consequences of a positive HIV test, such as transmitting the disease to family and children was noted as a deterrent to undergoing the test. Educating short-distance drivers regarding the modes of transmission and advances in HIV treatment regimens that can suppress viral load and enable them to live healthy fulfilling lives is important. 28
The short-distance drivers recognised the targeted HIV testing camps as a service for key stigmatised populations and hence, themselves avoided accessing services at these camps. It has been suggested that HIV testing must be available together with tests for respiratory viruses, blood-borne infections and other STIs. This will significantly lessen the stigma associated with getting tested for HIV and enhance the care of other illnesses. 29 A study in the district of Pune in Maharashtra, India with truck drivers and young men and women found high acceptability and willingness to undergo HIV oral self-test. 22 Further research into feasibility and acceptability of using such self-testing kits for short-distance drivers is warranted. The drivers reported common sentiments such as I am standing in front of you healthy indicating how they rationalised or minimised their perceived risk of infection and the presence of individual level barriers. 21 Misconceptions related to the manner in which diagnosis and treatment of HIV is done were also prevalent among short-distance drivers.
One of the most important ways to lessen the effects of HIV and AIDS is to tailor interventions to the requirements of key populations. 30 Programmes tailored to truck drivers showed positive changes in risk behaviours, knowledge and attitudes. 31 Interventions should therefore focus on individual, social and health system barriers to ensure access to HIV prevention and treatment services to short-distance drivers.
Our study addressed a gap in evidence by providing information about a key population’s challenges while accessing care for HIV. An important strength of our study is that we were able to collect data from nine states representing diverse regions across the country; hence our data is rich in scope and context. However, this study has few limitations. Our reliance on self-reported data might lead to some ‘socially acceptable’ responses, such as those regarding accessing testing, that may have been overreported. The use of snowball sampling technique could have also been a limitation as it might have resulted in underrepresentation of participants outside the social networks of the current study participants or from other parts or outside of the districts, leading to an incomplete overview of the barriers to accessing HIV testing and care among the short-distance drivers. Therefore, the findings of this study must be interpreted with caution.
The findings of this study show a need for HIV prevention and care interventions for short-distance drivers. The different individual, social and health systems barriers to accessing testing and treatment for HIV were identified. Our findings provide information for policy makers to address the healthcare needs of short-distance drivers. We recommend future research to understand the behaviour change communication and information education and communication (IEC) activities best suited to the needs and working environments of short-distance drivers.
Conclusion
This study underscores the critical need for customised HIV prevention and care programmes for short-distance drivers, a group facing unique obstacles in accessing healthcare. Challenges such as financial constraints, stigma, misconceptions and systemic issues like inaccessible healthcare services and limited outreach efforts significantly impede their ability to seek timely testing and treatment. Although many participants engaged in high-risk sexual behaviour, they exhibited limited awareness of available HIV services and often did not perceive the necessity for regular testing. These findings highlight the urgency of developing inclusive interventions that address barriers at the individual, social and health system levels, while promoting behaviour change through education and stigma reduction. The study points to the importance of integrating short-distance drivers into national HIV prevention and care strategies to ensure their needs are met.
Strengths and Limitations
A major strength of this study is its inclusion of diverse types of short-distance commercial drivers from nine states, offering detailed and context-rich insights into their healthcare challenges. This broad representation enhances the study’s relevance and provides a nuanced understanding of the barriers faced by this underrepresented group. Furthermore, the research fills a critical gap by focusing on the unique experiences and needs of short-distance drivers, a population often overlooked in HIV prevention and care initiatives.
However, there are limitations to consider. The reliance on self-reported data may have resulted in response biases, with participants potentially overstating socially desirable behaviours, such as seeking testing. Additionally, the snowball sampling method may have limited the inclusion of individuals outside the immediate networks of the participants, potentially restricting the scope of perspectives captured. Despite these limitations, the findings provide valuable insights that can inform future interventions.
Footnotes
Author’s Contribution
Conceptualization: PD. Methodology: PD, SL. Software: SL, AK. Validation: PD. Formal analysis: SL, AK. Investigation: PD. Resources: PD, CD, SR, BSK, SB, VV, SP. Data curation: SL, AK. Writing – Original Draft: SL, PD. Writing – Review & Editing: PD, AK, CD, SR, BSK, SB, VV, SP. Supervision: PD. Project administration: PD, CD, SR, BSK, SB, VV, SP.
Data Availability Statement
The datasets generated during and/or analysed during the current study are not publicly available due to ethical restrictions regarding data protection issues and the study-specific consent text and procedure, but anonymised data are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the National AIDS Control Organisation (NACO) Ethics Committee (Ref: T-11020/15/2021-NACO (R & E); dated 22 February 2022). Any protocol changes, participant consent alterations, or tool modifications were scrutinised and documented before implementation to prevent participant risk exposure. Ethical considerations were extensively discussed with all involved, sensitising the research team and data collectors to voluntary participation, privacy, and confidentiality. Rigorous ethical standards were maintained throughout. Regular progress reports were submitted to the NACO, detailing enrolment, discontinuations, study completions, alterations, and unexpected issues. Poststudy, all related documents were sent for preservation, with data sets, transcripts, and translations to be forwarded to NACO.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through grants from the National AIDS Control Organisation.
Informed Consent
Only adults aged 18 and above joined voluntarily, informed about the study’s scope, after providing written consent. Culturally sensitive, language-adapted tablet-based data collection allowed withdrawal rights. Participants received detailed information, accommodating illiteracy with thumb impressions, and interviews lasted 45–60 min.