
Abstract
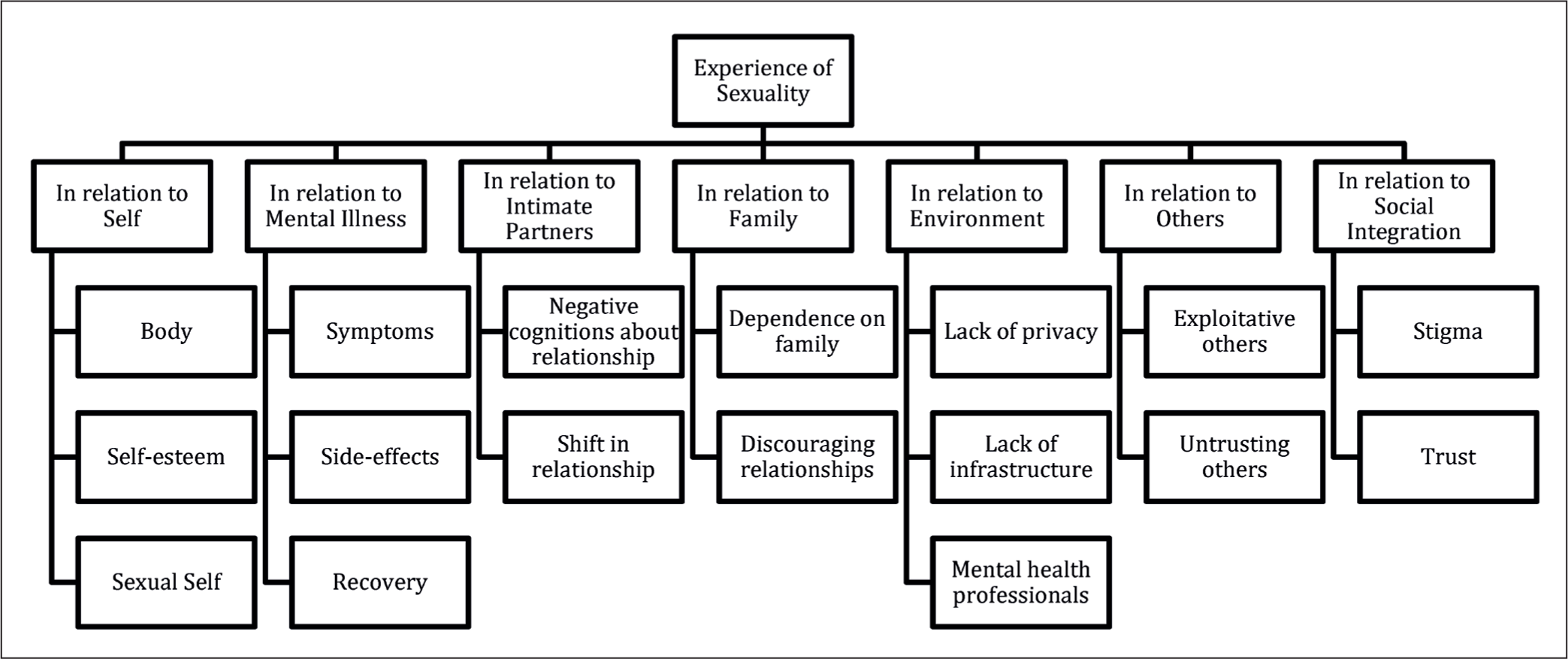
Mental illness has an impact on the experience of intimacy and sexuality by causing impairments in various domains of personal and interpersonal function. An in-depth exploration of the subject reveals various psychological and sociocultural factors impacting sexual functioning in persons with mental illness. This review attempts to synthesise available qualitative studies to generate interpretive themes that describe the narrative experiences of intimacy and sexuality in this population. Major and Savin-Baden’s metasynthesis method for qualitative research was used, with the modified PCO (Person, Context, Outcome) framework guiding the search strategy. A total of nine studies were obtained from a search of the electronic databases PubMed, ProQuest and Web of Science. ATLAS.ti software was used to code the primary and secondary data to generate 83 descriptive themes and 17 composite themes, which were further synthesised to create seven interpretive themes. These were About self (body, self-esteem and sexual self), mental illness (symptoms, side effects and recovery), intimate partners (negative cognitions about intimate relationships and shift in the relationship), family (dependence on family and discouraging relationships); environment (lack of privacy, lack of infrastructure and mental health professionals); others (exploitative others and untrusting others) and social integration (stigma and trust). The review establishes how the effects of mental illness pervade the experience of intimacy and sexuality by impacting their sense of self, body image, and the ability to initiate and nurture intimacy and conduct themselves in society as respectable and independent individuals. It highlights how treatment protocols and settings must incorporate the patients’ intimacy needs for holistic recovery and social integration.
Introduction
‘Sexuality, a central aspect of being human, encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy, and reproduction. It is influenced by biological, psychological, social, economic, political, cultural, legal, historical, religious and spiritual factors’. 1 Its definitions are closely tied to the sociocultural climate of the times 2 and can reflect how deeply acquainted society is with its core needs. Sexual health cannot be defined, understood, or made operational without a broad consideration of sexuality, which underlies essential behaviours and outcomes related to sexual health. With the growth and evolution of our understanding of human sexuality, its significance is being gradually acknowledged among clinicians, researchers and the general public. However, there are many grey areas when it comes to the experience of sexuality in vulnerable groups. Though we have come a long way from restricting and punishing sexual behaviour to accepting it as a fundamental human right, 1 much needs to be done to address sexual health in vulnerable groups, such as the differently abled, those suffering from chronic illnesses, those with mental health concerns, etc. The risk of developing sexual dysfunction is higher in those with depression, anxiety, and other severe mental disorders. 3 The prevalence of sexual dysfunction in the psychiatric population is estimated to be around 45%. 4 It was as high as 70% in an Indian study comprising women with severe mental illness. 5 Despite the prevalence of sexual difficulties in this population, how it manifests and shapes the sexuality of persons with mental illness needs more research attention. Few studies have focused on an in-depth exploration of the subject, while fewer have attempted to synthesise the available qualitative evidence.6,7 Synthesis makes it possible to delineate the shared aspects of sexuality within the lived experience of various mental illnesses. It contributes to addressing the concerns at the grassroots level. Therefore, the objective of the current review is to explore qualitative research on the subjective and narrative experiences of sexuality in persons with mental illness and synthesise the findings so that the specific needs and challenges faced by this population can be understood and adequate measures can be taken to integrate sexual health into their treatment.
Design
Major and Savin-Baden’s metasynthesis 8 method for qualitative research was used to search for, extract, synthesise, and interpret evidence. The modified PCO (Person, Context, Outcome) framework was used to formulate the search strategy.
Inclusion and Exclusion Criteria:
The review included qualitative (including phenomenological, grounded theory, and ethnographic) studies published in the English language, conducted between 2000 and 2022, on male or female cis-gender individuals with a clinical diagnosis of any mental illness as per the ICD or DSM classification. It excluded studies that examined marital problems and discord as the primary aim and those conducted on the LGBTQ+ population and those with diagnoses of neurodevelopmental and neurodegenerative illnesses.
Procedure
Search Strategy
The electronic databases PubMed, ProQuest, and Web of Science were searched using the search terms.
Common mental disorders OR Severe mental disorders OR Psychiatric illness OR Mental Illness AND Intimate relationships OR Sexual AND Relationships OR Functioning OR Need OR Expression OR Experience OR Perspective OR View OR Stigma OR Obstacles OR Difficulties OR Intimacy OR Perception OR Concerns AND Female OR Women OR Men OR Male OR Persons OR People OR Individuals AND qualitative.
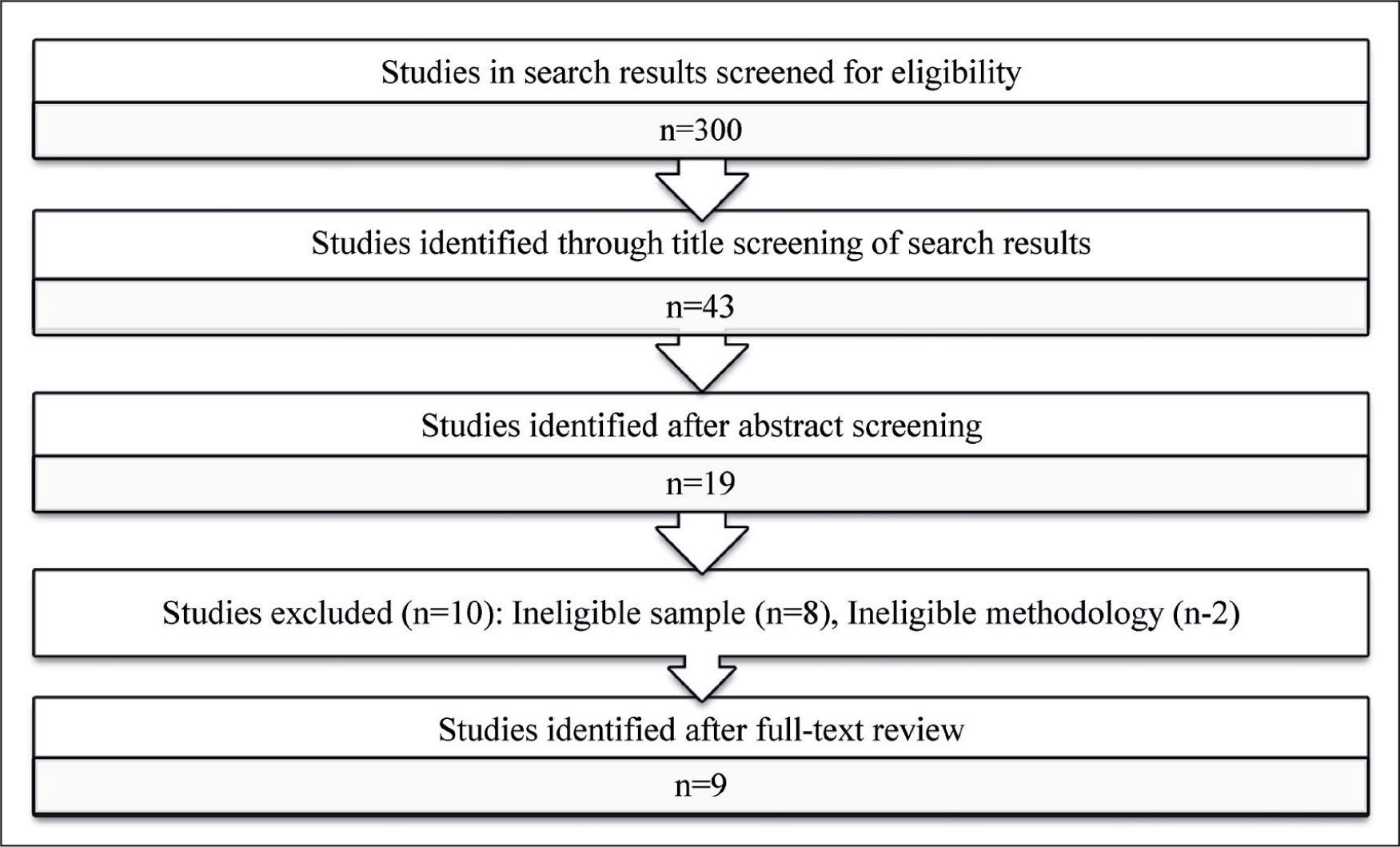
Titles and abstracts of the first 300 studies in the search results of each database were assessed for eligibility. The eligible studies were uploaded to Zotero software, and duplicates were removed. The full texts of the final list of studies were individually reviewed again to ensure eligibility. The studies were then appraised for congruity in the research goals, methodology, data collection techniques, and analysis to ensure soundness of quality. 8 Figure 1 summarises the reviewing process.
Article Screening and Selection.
Data Extraction
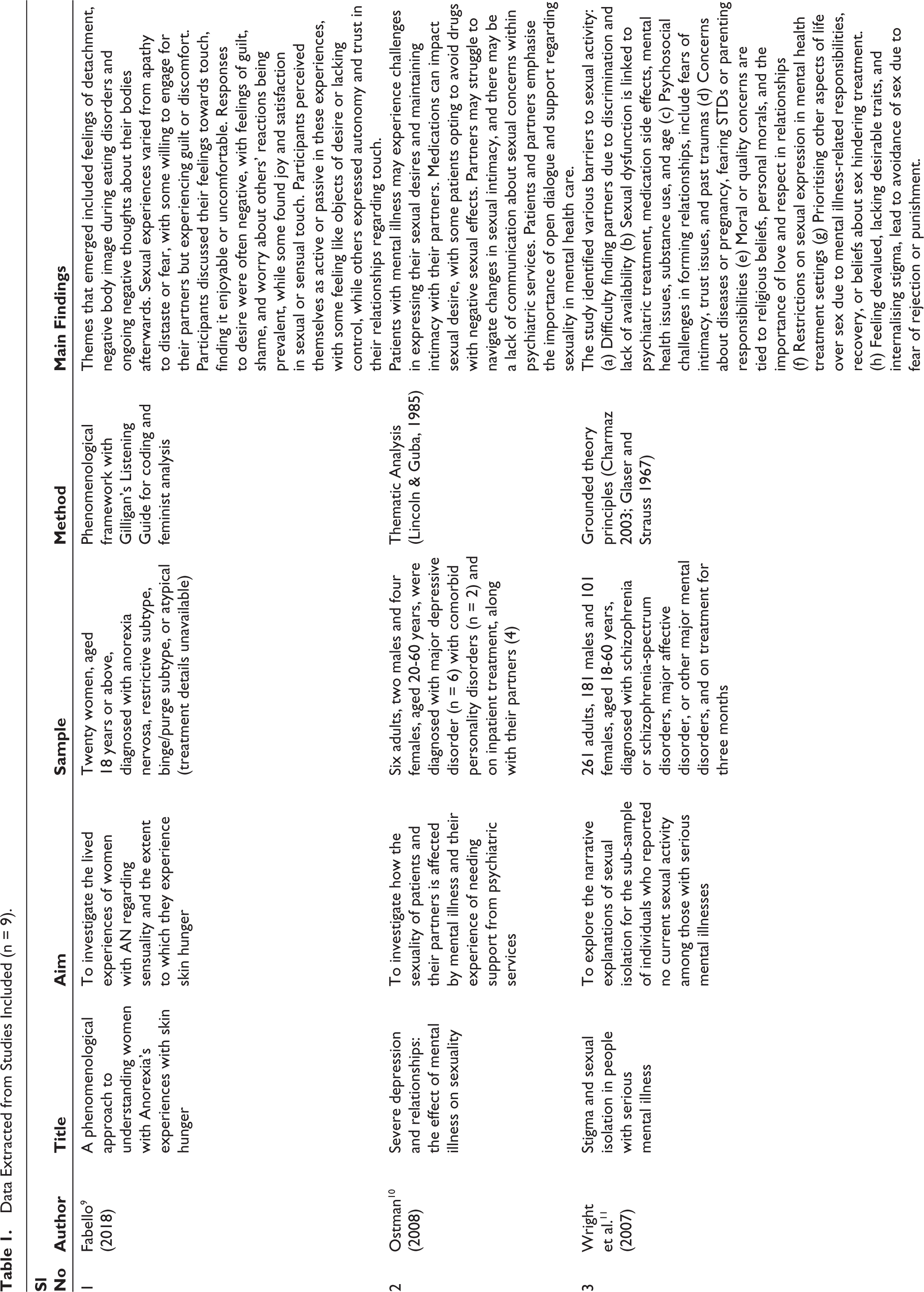
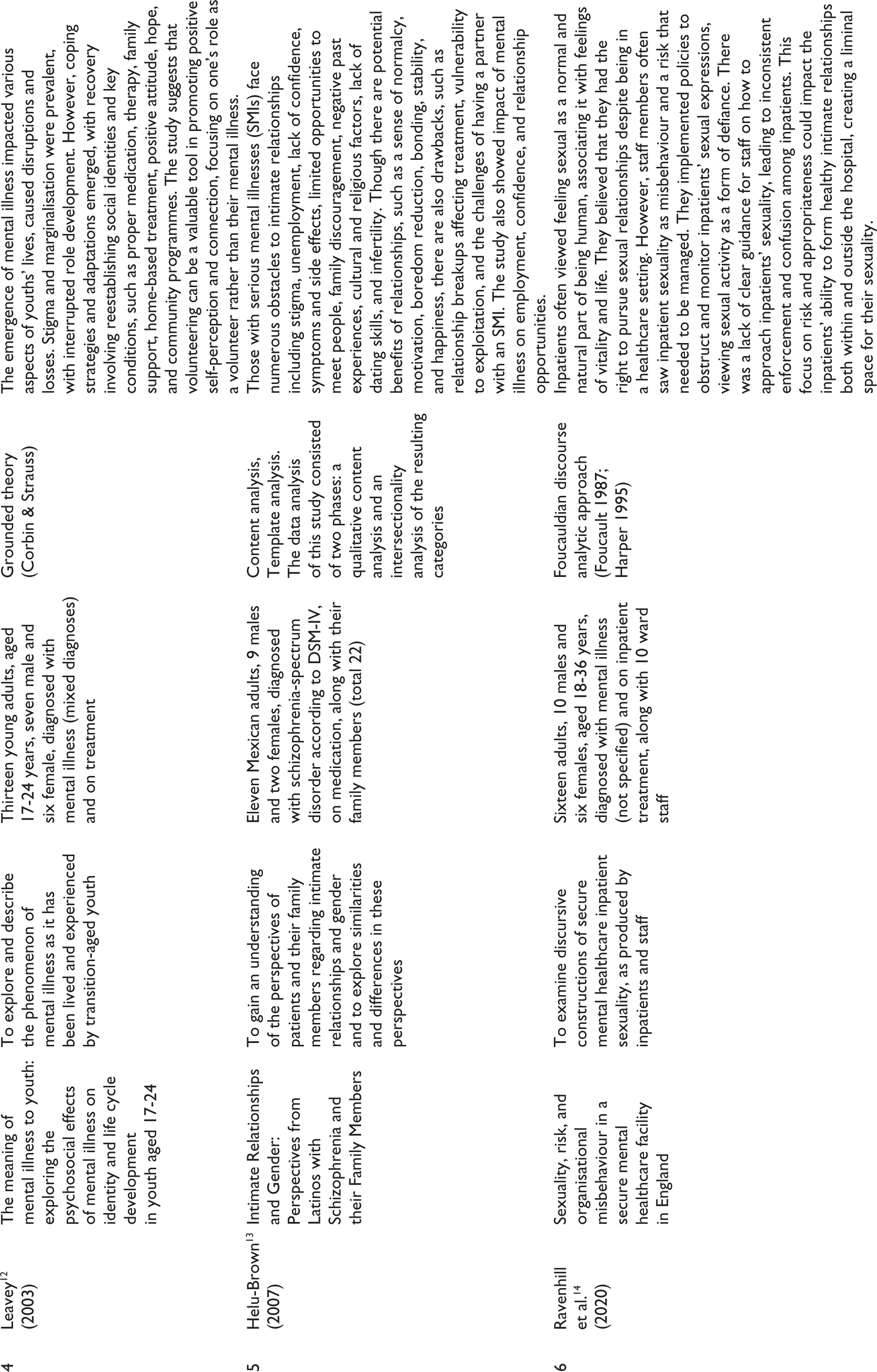
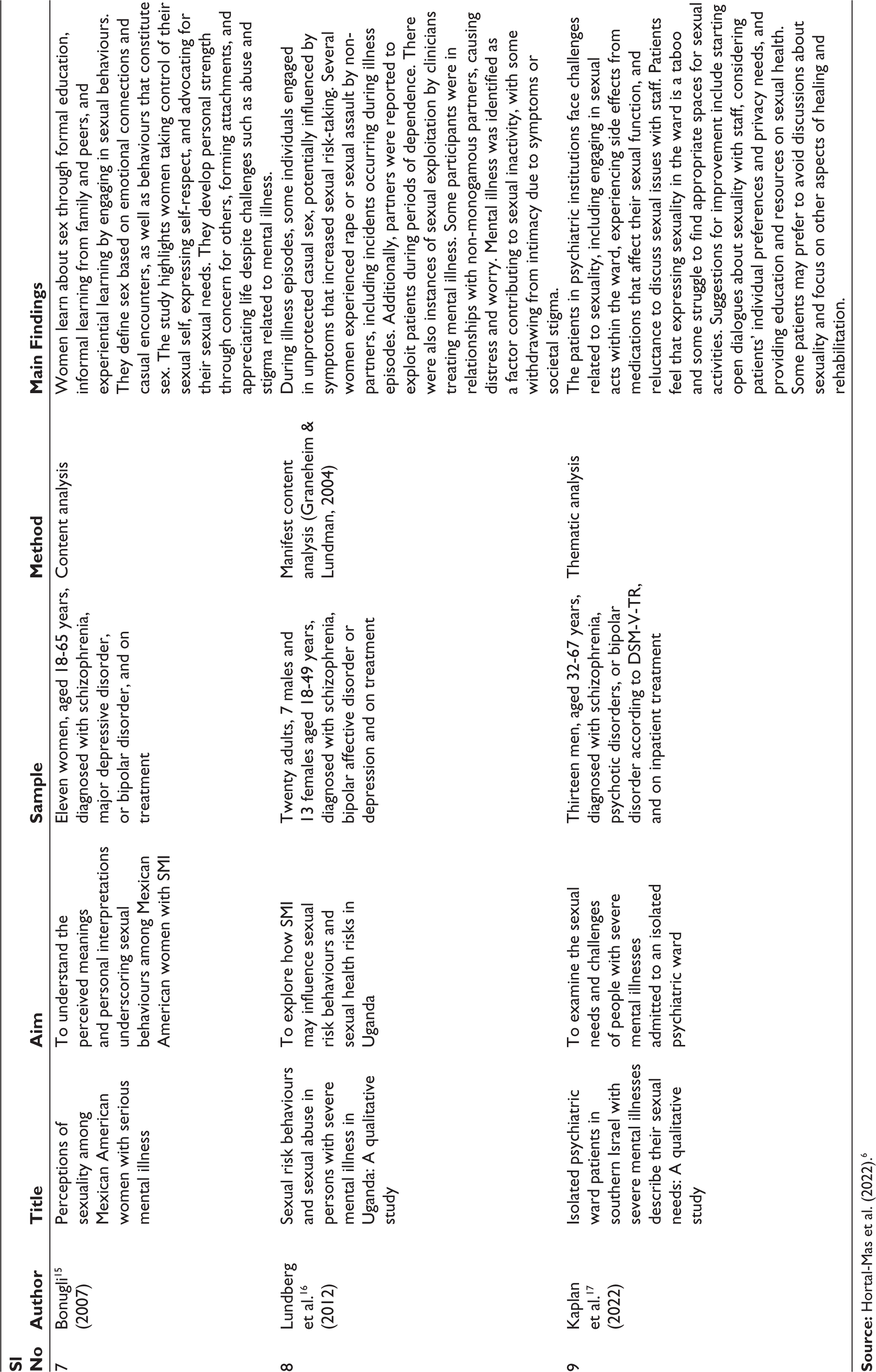
Primary data (the verbatim included in the study as evidence for each theme) and secondary data (the findings of the study) were entered into MS Excel (2019) with additional information such as year of publication, study objective, sample characteristics, procedure, and method of analysis. Table 1 summarises the extracted data.
Data Extracted from Studies Included (n = 9).
Synthesis
Line-by-line coding of the primary and secondary data using ATLAS.ti software gave 216 preliminary codes. The data under each code was reviewed and similar codes across studies were grouped into 83 descriptive themes. These themes were reviewed for their similarities and differences and categorised to give composite themes. Each reviewer checked the emergent themes against the data and made necessary modifications. They revisited and analysed the patterns and connections between the first- and second-order themes. This iterative process was repeated until seven interpretive themes emerged, that could sufficiently describe and explain the primary and secondary data. Figure 2 summarises the results of the metasynthesis.
Interpretive and Composite Themes Obtained from the Metasynthesis.
Results
The metasynthesis included nine qualitative studies, of which four were from the United States, one from the United Kingdom, one from Canada, one from Sweden, one from Israel and one from Uganda. The following were the themes that emerged from the thematic synthesis:
In relation to self: several Studies describe how the experience of sexuality is intimately related to the person’s self-concept, body perception and self-esteem in the context of their mental illness. The following sub-themes emerged in this category:
Body: Having a mental illness influences how an individual relates to their physical self. Studies show that persons with mental illness may experience discomfort with sensory stimuli, especially touch. Many report having no awareness about how their bodies interact with the environment, generally and during sexual or intimate experiences.
9
A disconnection with the body, experiencing it as separate from themselves, is common. Some studies emphasise how their bodies are perceived to be at war with them by not cooperating
9
or fitting a certain ‘ideal’,
10
thus leading to feelings of discomfort or even disgust. This was related to prominent themes of a negative body image—one that was undesirable, unattractive and lacking in physical attributes that were commonly desirable.
11
These feelings persist well into the recovery phase of their illness, thus making intimacy a challenge.
9
Self-esteem: During an active phase of mental illness, studies reveal experiences of disruption in all domains of life. This disruption leads to changes in the patient’s self-concept, with many grappling with the reality of being mentally ill and what it means to their identity.
12
In addition to feeling undesirable physically, the experience of mental illness and the social isolation associated with it leads to decreased self-confidence in their interpersonal and professional domains. The lack of employment poses difficulties as financial stability and child-rearing responsibilities are significant factors that potential partners would consider.
13
There are also beliefs that they have become less popular and desirable in their peer groups compared to their premorbid selves.
12
Throughout the illness, its treatment and recovery, patients struggle with significant changes in their self-concept, poor self-esteem and a sense of being devalued in their own families, peer groups and society at large. Sexual self: Studies show a strong association between sexual feelings and feelings of normalcy and health. Sexual needs are acknowledged as a normal part of the human experience, and many advocate for their sexual rights.
14
This can be seen in the open expression of sexual health concerns to health care providers, pursuing sexual needs in settings that unfairly prohibit them and prioritising sexual pleasure despite being told not to.
15
Intimacy and the comfort of touch from trusted others are expressed as one of the most healing aspects of relationships. The need to trust the partner entirely and feel a sense of control in intimate encounters is a common theme.
9
This is an extension of the degree of sexual exploitation that persons with mental illness are vulnerable to.
16
Making appropriate choices that honour one’s sexuality and self-respect is deemed an invaluable skill that preserves and promotes mental health.
15
On the other hand, there are also themes of feeling ambivalence towards touch, intimacy and sex.
10
Some studies reveal how persons with mental illness feel a sense of disgust towards sexual contact and feelings of confusion regarding the validity of such an experience in a normatively sexual society.
9
In relation to mental illness: The experience of mental illness impacts sexual health in various ways. The following are the different aspects that emerged from the studies. Symptoms: The symptoms of mental illness have a direct bearing on a person’s emotional state, perception and behaviour.
3
It has a profound impact on the way they interact with people and their confidence.
11
These difficulties in social interactions, in turn, pose a challenge in finding intimate partners.
16
The episodes of illness also increase tendencies to engage in substance use and risky sexual acts, furthering dysfunctional patterns of interpersonal behaviours.
16
Another aspect that gets affected during the illness is the body image, which takes an adverse turn as a result of distorted perception and cognition,
9
which are a common part of mental illness. Side-effects: Almost all studies discuss the effects of psychiatric medications on sexual functioning. While some drugs do not have any impact, others commonly cause sexual side effects, especially in areas of sexual desire and arousal.
10
In males, the effects include erectile dysfunction, premature ejaculation, a diminished sense of masculinity, etc.,
17
while in females, there is a lack of interest in engaging in sex due to the various mental and physical effects of mental illness and treatment.
11
The sexual side effects have been severe enough for patients to discontinue medications.10,17 Recovery: Several studies emphasised the patients’ focus on their recovery process and inner healing,
10
while also trying to establish themselves in terms of employment.
11
Amidst this process, many find it challenging to pursue sexual intimacy and believe serious relationships to be better reserved for when they are in a better place mentally and financially. However, various factors aid in the recovery process. While medications give a sense of stability, patients also worry about how dependent they are on them.
12
Sharing intimacy with a partner has been commonly reported as a healing experience in times of emotional turmoil.
9
Understanding the partner’s needs and responding to them with intimacy and sexual expression helps the person build their repertoire of relationship skills.
15
Such learning supports the development of attachment with people, giving them a sense of normalcy and satisfaction with their lives.
13
Seeking and establishing social relations and taking part in social initiatives bring back a sense of community while helping decrease the sense of dependence on family. Such a gradual process of reestablishing intimacy and social identity helps solidify the recovery process.
12
In relation to intimate partners: The need for intimacy and connection was expressed as a very important one in the recovery from mental illness, as described above. The other important aspects of this theme include:
Negative cognitions about intimate relationships: There are several fears and apprehensions that persons with mental illness have regarding intimate relationships. A common negative belief is that love is reserved for those who meet certain criteria like physical attractiveness,
10
a good salary and social status.
11
It is challenging to move beyond the constraints imposed by mental illness and risk being vulnerable to possible rejection.11,13 Illness episodes may be experienced by them as an interrupted reality,
9
after which the person is left confused about how to behave ‘normally’ in close encounters.
14
There are also fears of disclosing the mental illness to potential partners due to the stigma associated with the label.10,13 Other apprehensions were those surrounding the possible risk of acquiring STDs, getting pregnant, etc., along with moral concerns about engaging in premarital sex.
11
Shift in relationship: A common theme seen across studies is the change in how intimate relationships are perceived after the onset of mental illness. In addition to the fears and apprehensions mentioned above, patients describe finding sex and intimacy to be meaningless.11,12 There is also hopelessness rising from challenges of finding a partner.
10
For those who are partnered, the patients may notice a shift in the relationship as the partner inhibits their sexual expression either to accommodate the varying moods and needs of the patient or as a natural reaction to the patient’s symptoms, like suicidality or dysphoria.
10
On the other hand, there may also be ways in which the partner may contribute to the patient’s symptoms with their own personality disturbances or dysfunctional behaviours.
13
Another prominent theme that emerged was the shift in how patients dealt with the expectation of sex in the relationship. Many report consenting to sexual intimacy in order to fulfil their duties, failing which they end up feeling guilty. They often do not enjoy sexual contact and may even ask their partner to stop as they are not able to go on.
9
In relation to family: Family members play a significant role in the treatment and recovery of people with mental illness. They also impact how these individuals engage interpersonally and reintegrate into society, as described by these themes:
Dependence on family: Many studies reveal patients’ difficulties in becoming fully independent. Most are at least financially dependent on their families, if not for housing and emotional support.
12
This is mainly due to factors surrounding decreased employability due to the presence of or history of mental illness, in addition to the cognitive decline accompanying several mental illnesses.
12
These factors make it further challenging to establish oneself independently and seek or maintain intimate relationships. Discouraging relationships: Family members often actively discourage patients from seeking long-term relationships due to fears of it worsening their symptoms.
13
They also express a lack of trust in the patient’s ability to make appropriate decisions,
12
thus augmenting the patients’ poor self-esteem and beliefs of inadequacy. In relation to environment: The treatment settings are revealed to be sexually restrictive and encroaching on the sexual rights of the inpatients, as illustrated in the following themes:
Lack of privacy: The ward staff are directed to monitor patients throughout the day and night closely. Any sexual aids, such as vibrators, condoms, etc., are to be used only with permission and by those with these privileges.10,14 The lack of a private space is an outcome of poor infrastructure at the hospital
17
and an extension of the mandated monitoring that patients undergo. These aspects make pursuing sexual needs uncomfortable and difficult. Lack of infrastructure: The treatment settings commonly have an open design, with monitoring and easy intervention built into it. Even though these are of prime importance to prevent harm to the patients, such a design makes it impossible for patients to meet their sexual needs during the entire course of treatment. Many hospitals also do not have provisions in place for conjugal visits, thus denying the patients’ basic rights to sexual intimacy.
17
Mental health professionals: The MHP’s role in providing a safe environment for patient recovery cannot be overstated. Studies show that the hospital protocol mandates the ward staff and doctors to discourage patients’ sexual activity and punish any partnered sexual act within the hospital walls.10,14,17 Even though such prohibitions are in place to prevent sexual exploitation and misdemeanour, they stifle patients’ very human needs
14
and make them something to be ashamed of.
10
MHPs also discourage discussions about sexual topics or sharing sexual concerns, as these are not supposedly the patients’ primary concerns.
10
In relation to others: There are poignant accounts, in the narrative experiences of patients, of occasions in which another person’s actions or words have impacted their sense of self and agency. The themes in this category include:
Exploitative others: Studies reveal how persons with mental illness are vulnerable to sexual exploitation by partners,
16
family members10,15 and strangers.
15
Several incidents of rape reported by patients across studies that occurred after the onset of mental illness indicate how the perpetrators view them as easy targets due to their illness.
16
There are also common experiences of the victim being blamed or disbelieved when they raise a complaint against the perpetrator,
15
thus strengthening the notion that they would be helpless in defending themselves or getting justice. Several accounts of intimate partners also exploiting them sexually due to their financial dependence on them
16
point toward a deeper problem of structural discrimination that keeps the mentally ill in a position of disadvantage in intimate relationships. Untrusting others: An important theme that emerged across studies was how others perceived persons with mental illness as incapable of making appropriate decisions. This included experiences of their family not allowing them to make independent decisions or asking for their opinions, therapists not listening to what they want and instead making treatment goals for them,
12
hospitals monitoring and controlling them in all matters,14,15 and not being taken seriously at the workplace.
12
These experiences take away the person’s trust in their own decision-making ability and propel a vicious cycle of dependency. In relation to social integration: A primary underlying reason why the experience of mental illness makes it challenging to seek intimate relationships and have a satisfying sex life is the difficulty in the social integration of a person with mental illness. Stigma: After receiving a clinical diagnosis, their identity changes to that of someone with a mental illness.
12
This label comes attached with a declining social standing,12,13 poor employment prospects and decreased desirability.
12
It leads to avoidance of social engagement, which suspends the development of social identity in the young.
12
The stigma makes it shameful to disclose the illness to potential partners and friends.
10
Trust: Another emerging theme is the difficulty of trusting people because of previous experiences of violation of personal boundaries and exploitation.11-13 This perpetuates a state of feeling devalued in society and being unable to venture beyond the limitations of mental illness because the world cannot be trusted to not harm them.
11
Discussion
An individual’s experience of sexuality is closely tied to biological, psychological, and sociocultural factors, among others. 1 Therefore; it is no surprise that persons suffering from mental illness also experience difficulties in sexual functioning. However, the nature and depth of these difficulties and how they contribute to their mental health concerns are often neglected from exploration through research. The current evidence synthesis was an attempt to understand and synthesise findings from different studies to give an overall perspective on the experience of sexuality in persons with mental illness. It must be highlighted that seven of the nine studies were from Western countries and hence may reflect the experiences within the sociocultural context of Western societies. It also indicates the dearth of studies on the subject in other parts of the world.
The first theme that emerged describes how the self relates to sexuality in the context of mental illness. Three interconnected aspects that could be seen were the Body, Self-esteem, and the Sexual Self. Having a mental illness significantly influences a person’s relationship with their physical self, manifested as discomfort with touch and disconnection with the body and its responses to the environment. 9 Some perceive their bodies as being at war with them, either by not cooperating or not fitting societal ideals.9,10 This association contributes to a negative body image characterised by feelings of being unattractive and lacking commonly desirable physical attributes. 11 In extension it has a critical impact on self-esteem, which also plays an important role in a person’s interpersonal relationships.18-20 The lack of financial stability and a decreased involvement in family decision-making as a consequence of mental illness contribute to poor self-esteem. There are also beliefs of being perceived differently by their families and peers after being diagnosed with mental illness, 12 creating a sense of decline in their social standing. Together, these impact the person’s confidence in pursuing intimate relationships. 20 However, studies highlight how the comfort of touch and intimacy are expressed by persons with mental illness as contributing to their healing. 9 Sexual needs are associated with feelings of normalcy and aliveness, and many advocate for their sexual rights in restrictive treatment settings. 14 Another aspect that emerged is the need for absolute trust in the partner and control in intimate encounters, 9 which can be seen as a result of personal and collective experiences of sexual exploitation that persons with mental illness are exposed to.16,21 In contrast, there are studies which emphasise the discomfort with sexual contact that persons with mental illness experience- ranging from ambivalence and confusion 10 to feelings of disgust and aversion. 9
The second theme describes how mental illness directly impacts the sexual experience of the individual in terms of the manifested symptoms, the various side effects of treatment and the recovery process. The symptoms of mental illness impact the way a person interacts in interpersonal contexts by its influence on their emotional state, perception and behaviour. 3 In addition to negative self-beliefs and body image, the illness episodes increase the risk of dysfunctional interpersonal behaviours, such as sexual risk-taking. 16 Several studies discuss the sexual side-effects of medications10,11,17,22 and how often patients have to choose between their sexual needs and psychiatric treatment.10,11 However, medications are crucial in restoring the patient’s sense of stability. During the recovery from mental illness, several studies reveal how persons tend to prioritise this sense of stability and getting back on their feet before pursuing intimate relationships,10,11 though partners contribute to their healing in various ways. The experience of intimacy helps during emotional turmoil, 15 and sexual expression and the development of a deeper attachment with the partner restores a sense of normalcy and satisfaction in their lives. 13 Such a gradual process of reestablishing intimacy and social identity helps solidify the recovery process. 12
Intimate partners play an important role in the experience of sexuality of persons with mental illness. 20 However, as discussed above, several factors related to the self and mental illness inhibit the seeking of intimacy. This results in several negative cognitions regarding intimate relationships, such as apprehensions of not being good enough in terms of physical attractiveness and social and financial status. 11 There are also prominent themes of fear of rejection and subsequent avoidance of socialisation and intimacy.12,13 Patients also experience confusion about how to behave in close encounters with people due to an interruption in their daily social activities owing to mental illness. 14 Disclosing about the illness to potential partners is another grey area that makes it even more challenging to navigate due to the stigma associated with the label.10,13,22 Other concerns like the risk of STDs, pregnancy, etc, also prevent active engagement in sexual relationships. Another consistent aspect across several studies is a shift in the relationship after the illness’s onset. This could be regarding the perception of relationships as meaningless or its pursuit hopeless.10-12 It could also be related to partner behaviours in response to patients’ illness episodes, such as inhibiting sexual expression during their recovery.10,22 On the other hand, many patients experience feelings of discomfort with or decreased interest in sexual contact but feel burdened by the pressure to fulfil their duties and give consent to prevent feelings of guilt. 9 Partners with personality disturbances or dysfunctional behavioural patterns of their own might worsen the patient’s symptoms, 13 which may lead to their distancing from the relationship. These factors together make the experience of intimacy and sexuality challenging for persons with mental illness.
The role of the family in the treatment and recovery of mental illness cannot be overstated. It provides the scaffolding for patients to engage interpersonally and participate meaningfully in society. This also means that, in several ways, the experience of intimate relationships is also contingent on family support. The dependence of patients on their families for emotional and financial support prevents their individuation. Studies show an active discouragement of patients by their families from seeking long-term relationships due to a lack of trust in their decision-making abilities or fears of their symptoms worsening.12,13 These factors result in perpetuating a cycle of dependence on family, poor self-esteem, and decreased confidence in their ability to make decisions, preventing the patient from engaging in intimate relationships.
The next theme that emerged describes the impact of the environment on the experience of sexuality in persons with mental illness. Studies consistently show that treatment settings are sexually restrictive and designed for the easy monitoring of patients throughout the day. 20 The lack of infrastructure prevents provisions for conjugal visits and private sexual activities.10,14 The need for obtaining permission for sexual aids, along with the close monitoring and punishment of partnered sex by ward staff, ensures that sexual activity is rarely ventured into. There is also active discouragement of discussion about sexual topics, and sharing of sexual concerns is not welcomed. The policies of some hospitals seem to point towards an invalidation of the sexual needs of persons with mental illness. 17
There are poignant accounts by patients in several studies of being exploited and treated with mistrust by others. Sexual exploitation by partners, family members and strangers points towards a more profound vulnerability in this population due to their illness and the blaming and shaming that they often go through in the aftermath. 21 This perpetuates the notion that they are easy targets for exploitation. 16 Such previous negative experiences contribute to currently held beliefs and attitudes towards intimacy and sexuality, placing them in a disadvantaged position in the relationship. Alongside the exploitation is the aspect of others who do not trust the patients’ decision-making abilities. This includes family members, therapists, hospitals, and workplaces that communicate an attitude of mistrust concerning their ability to think and make appropriate choices, to know what is best for them, and to have the skill set to take on responsibilities. Exploitation and mistrust prevent patients from moving beyond the limits of their illness and acquiring complete recovery.
The last theme that emerged was about social integration. The stigma associated with the label of being mentally ill impacts the person’s self-concept12,22 and has an extended influence on their employability, desirability, 20 and social status. Another aspect that comes with the experience of mental illness is vulnerability to exploitation and subsequent difficulty of patients to trust people.11-13,21 Previous negative experiences make it difficult for them to trust the world not to be rejecting, hurtful or exploitative. These factors prevent social integration and make seeking and engaging in intimate relationships challenging.
Conclusion
In conclusion, the evidence synthesis sheds light on the intricate relationship between mental illness and sexuality, unravelling a complex tapestry of interconnected themes. Mental illness affects every domain that is relevant to an intimate relationship. Starting from the effects on psychological aspects such as cognitive functioning, a positive self-concept and body image, it deprives the individual of the skill sets required to initiate and nurture intimacy and conduct themselves in society as respectable and independent individuals. It leaves them confused and disoriented about themselves, their needs and rights. Despite the several benefits of an intimate relationship in the recovery of the individual, the negative attitudes of the family, peers and society hold them back from exploring themselves beyond their mental illness. As the label of mental illness shapes their identity in several ways, the treatment should, in essence, enable recovery from the limits imposed on their identity, too. This will remain a distant dream as long as treatment settings continue to neglect the necessity of integrating intimacy needs into therapeutic goals and recovery.
Footnotes
Limitations of the Study
The study has included only nine studies in the synthesis. A more comprehensive search could give more relevant studies. The studies were also not subjected to stringent quality assessment because fewer numbers were obtained. The severity and duration of mental illness, gender and cultural aspects may influence the sexuality and intimacy expression.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.