
Abstract
Background:
Men who have sex with men (MSM), a high-risk group for HIV/AIDS, face various health issues. However, research is scarce on MSM in India, and available studies generally focus on the mental health of HIV-infected MSM rather than their overall health. Therefore, this study aimed to assess the quality of life (QOL) among MSM.
Materials and Methods:
This observational cross-sectional study was done in Sagar, Madhya Pradesh, involving 100 MSM individuals. Participants were recruited from a non-governmental organization that works toward the welfare of MSM individuals. Socio-demographic data were collected using a semi-structured questionnaire, while QOL was measured using the Hindi version of the WHOQOL-BREF questionnaire. Quantitative variables were summarized using mean and standard deviation, and qualitative variables were summarized using frequency and percentage. The differences between mean QOL scores were analyzed using t-test/analysis of variance, and Pearson’s correlation coefficient was used to assess the correlation between domains.
Results:
Most participants were 21-40 years of age, with a mean age of 34.8 (±8.1) years. Most participants resided in urban areas and identified as Hindu (92%). The scores of WHOQOL-BREF ranged from 0 to 100, with higher scores indicating better QOL. The mean scores for general QOL and general health among participants were 42 ± 20.4 and 67.5 ± 24.7, respectively. Among the four domains of WHOQOL-BREF, social relationship domain had the highest mean QOL score (72.7 ± 11.5), while the psychological domain exhibited the lowest score (57.2 ± 11.7). The mean scores for the physical and environmental domains were 70.9 ± 8.7 and 59.6 ± 10.7, respectively.
Conclusions:
The findings underscore the importance of addressing various health aspects beyond HIV/AIDS in this population to improve their overall well-being and life satisfaction.
Introduction
For thousands of years, men who have sex with men (MSM) have existed in India. This is evidenced by temple sculptures depicting homosexuality at Konark and Khajuraho (950-1050 AD) and different treatises dating back to ancient times. 1 There is no government or public data regarding the total population of MSM in India. However, according to the Joint United Nations Programme on HIV/AIDS data, population size estimates of MSM were 238,200 for India in 2016. 2 Although the sexual minority group of MSM is regarded as a high-risk group for HIV/AIDS, MSM faces several other health issues. These problems range from intimate partner violence, mental health issues, substance abuse, body dysmorphia, reproduction, and fertility to other sexually transmitted infections.3,4 Study findings have indicated that stigma significantly fosters negative self-perceptions, diminished self-confidence, depression, increased sexual risk behavior, and reduced utilization of HIV prevention services within the sexual minority community. In the context of India, studies have shown that mental health issues are prevalent among MSM, including depression, anxiety, and suicidal thoughts. Consequently, it has been recommended that healthcare professionals screen MSM for psychological and mental health disorders while offering support to help them cope with the stigma associated with their sexual orientation.1,5,6
Quality of life (QOL) is recognized as a reliable indicator of overall health. QOL reaffirms the World Health Organization’s (WHO) commitment to promoting a holistic approach to health and healthcare. WHO defines QOL as individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It is a broad notion influenced by a person’s physical health, psychological condition, level of independence, social ties, personal views, and relationship to critical characteristics of their environment in a complex way. In healthcare, QOL assessment has a variety of applications. It is more comprehensive and congruent with the WHO’s notion of health because it measures functioning and well-being rather than diseases and disorders. It can be used to guide appropriate management techniques as well as one of the outcome indicators for comparing them, such as drug trials. Beyond symptoms and signs, QOL assessment focuses on components of a patient’s life. As a result, healthcare workers are more likely to notice and address the direct and indirect consequences of sickness and treatment on people. QOL is also helpful in policy analysis, such as programme evaluation and budget allocation. 7
Previous research on QOL in the MSM community has found that examining MSM QOL can provide insight into their physical, psychological, cognitive, and social functioning based on their health assessments.8,9 There are very few studies done in India among MSM; moreover, those studies mainly observed the mental health status among HIV-infected MSM but not the overall health. Therefore, the present study aimed to assess the QOL among MSM.
Materials and Methods
Study Design, Subjects, and Setting
This observational cross-sectional study was conducted in Sagar, Madhya Pradesh, India, among MSM.
Sample Size and Sampling
The sample size was calculated by the formula: n = (Z 2 σ 2 )/d 2 and where Z = 2.58 (at 99% confidence), σ = 17.09, σ is the standard deviation (SD) of psychological health among MSM, which was 17.09 from a previous study, 10 and d = 5% (absolute precision). This gives a value of 77.8, adding 20% for non-response/missing data, and rounding off leads to the final sample size of 100. Non-probability sampling was done for this study purpose.
Selection of Study Sample
Participants were recruited from the registered individuals in the “Tumul Social Fundamental Development Society,” a non-governmental organization of Sagar, Madhya Pradesh, working toward the welfare of MSM in Sagar.
Inclusion Criteria and Exclusion Criteria
MSM individuals registered in the Tumul Social Fundamental Development Society were included, while HIV-seropositive MSM individuals, those with chronic disease, and those unwilling to participate were excluded.
Study Tool
A semi-structured questionnaire was used to collect data which had two parts. The first part included basic socio-demographic information about participants. It included age, occupation, educational status, marital status, and residence (urban/rural). While in the second part, data regarding QOL were collected using the Hindi version of the WHOQOL-BREF questionnaire, 11 which is a validated scale (five-point Likert scale). The Hindi version of the WHOQOL-BREF has demonstrated both reliability and validity in measuring QOL.12,13 Several studies have assessed the QOL of MSM using the WHOQOL-BREF tool.14,15 The WHOQOL-BREF includes 24 items in four domains—physical health, psychological health, social relationships, and environment—and two items on overall QOL and general health. The 26 items are scored from 1 to 5, and the scores are transformed into 0 to 100, with higher scores indicating better QOL.
Statistical Analysis
Data from all participants were imported to IBM Statistical Package for Social Sciences (SPSS) software (IBM Corp., released 2019. IBM SPSS Statistics for Windows, Version 26.0, Armonk, NY: IBM Corp.) for analysis. There were no missing data. Quantitative variables were described using mean and SD, and qualitative variables were summarized using frequency and percentage. Normality assumptions were checked, and the difference between mean scores of QOL was tested by t-test/analysis of variance (ANOVA). Pearson’s correlation coefficient was used to determine the level of agreement between the domains of WHOQOL-BREF. A P value of less than 0.05 was considered significant.
Results
Basic Characteristics
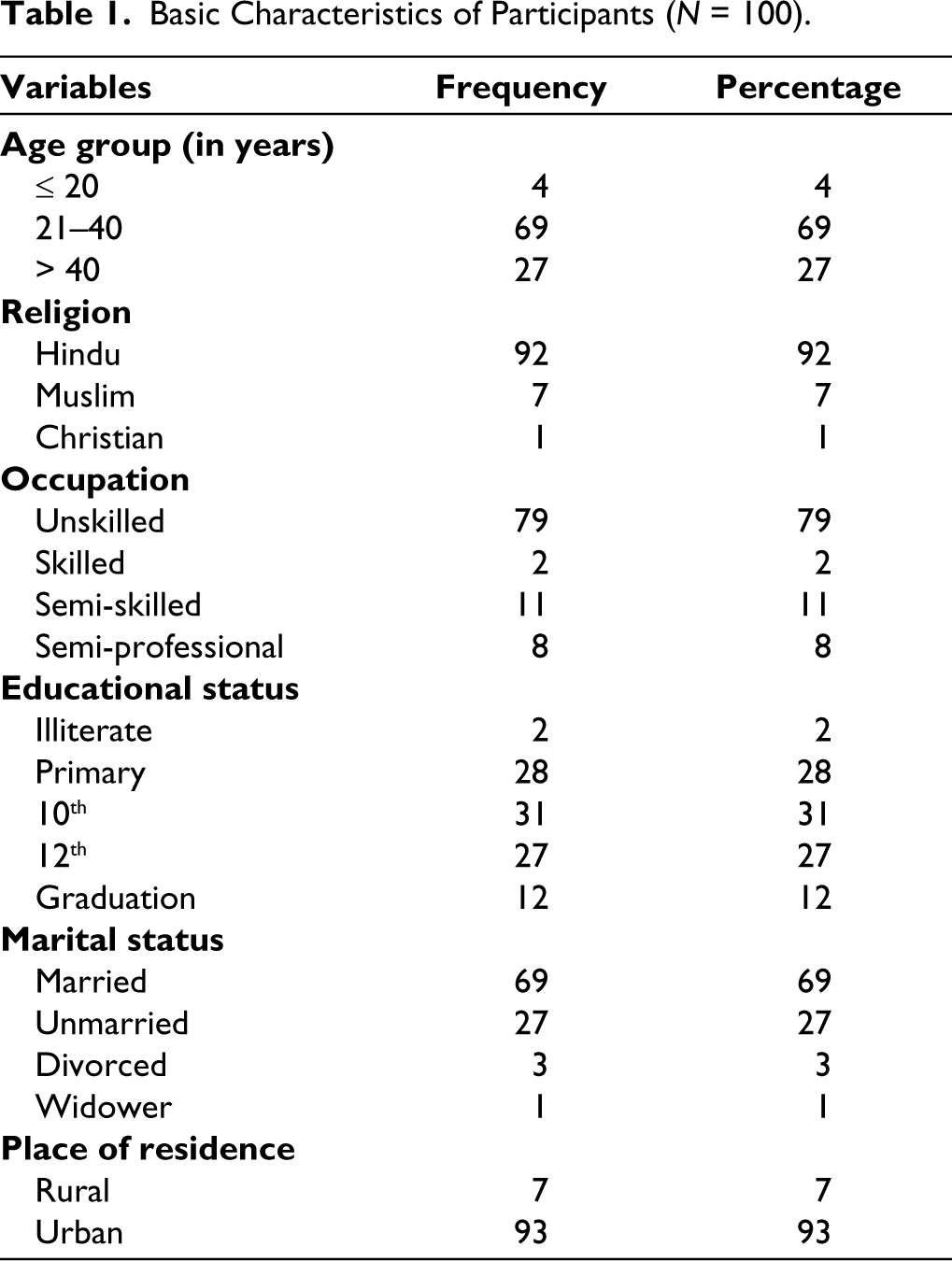
Out of 100 participants, the majority belonged to the age group of 21–40 years, with a mean age of 34.8 (±8.1) years. Table 1 describes other basic characteristics of participants.
Basic Characteristics of Participants (N = 100).
Quality of Life
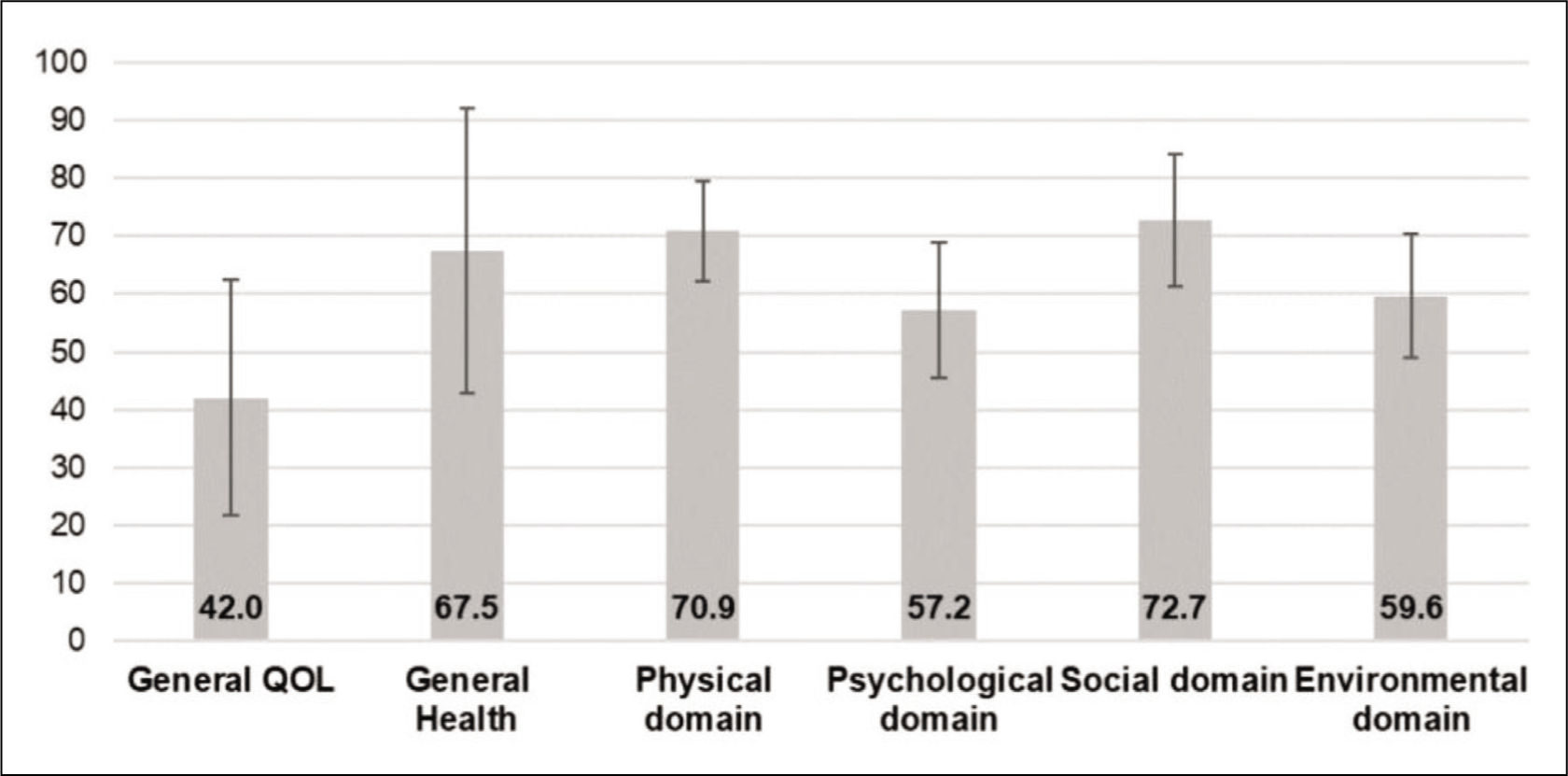
The mean score of general QOL among participants was 42.0 ± 20.4 on a 0-100 scale. Of the four domains, the social relationship domain had the highest mean score of QOL (72.7 ± 11.5), and the psychological domain demonstrated the lowest score (57.2 ± 11.7) (Figure 1).
Quality of Life of MSM.
Domain Score Across Different Variables
The differences in the mean score of all four domains, along with the general QOL and general health across different socio-demographic variables, are displayed in Table 2. The differences in the mean score of general health and physical domain across the age group were significant, and the rest scores were insignificant. No significant differences in mean scores of all the domains across the religion were seen. The differences in mean scores of all the domains across the occupational status of the participants, except for general QOL, were not statistically significant. However, the differences in mean scores of general health, psychological domain, and environmental domain across the educational status of the participants were statistically significant. Significant differences between marital status and general health, psychological, and environmental domains were seen.
Comparison of Domain Score According to Different Variable.
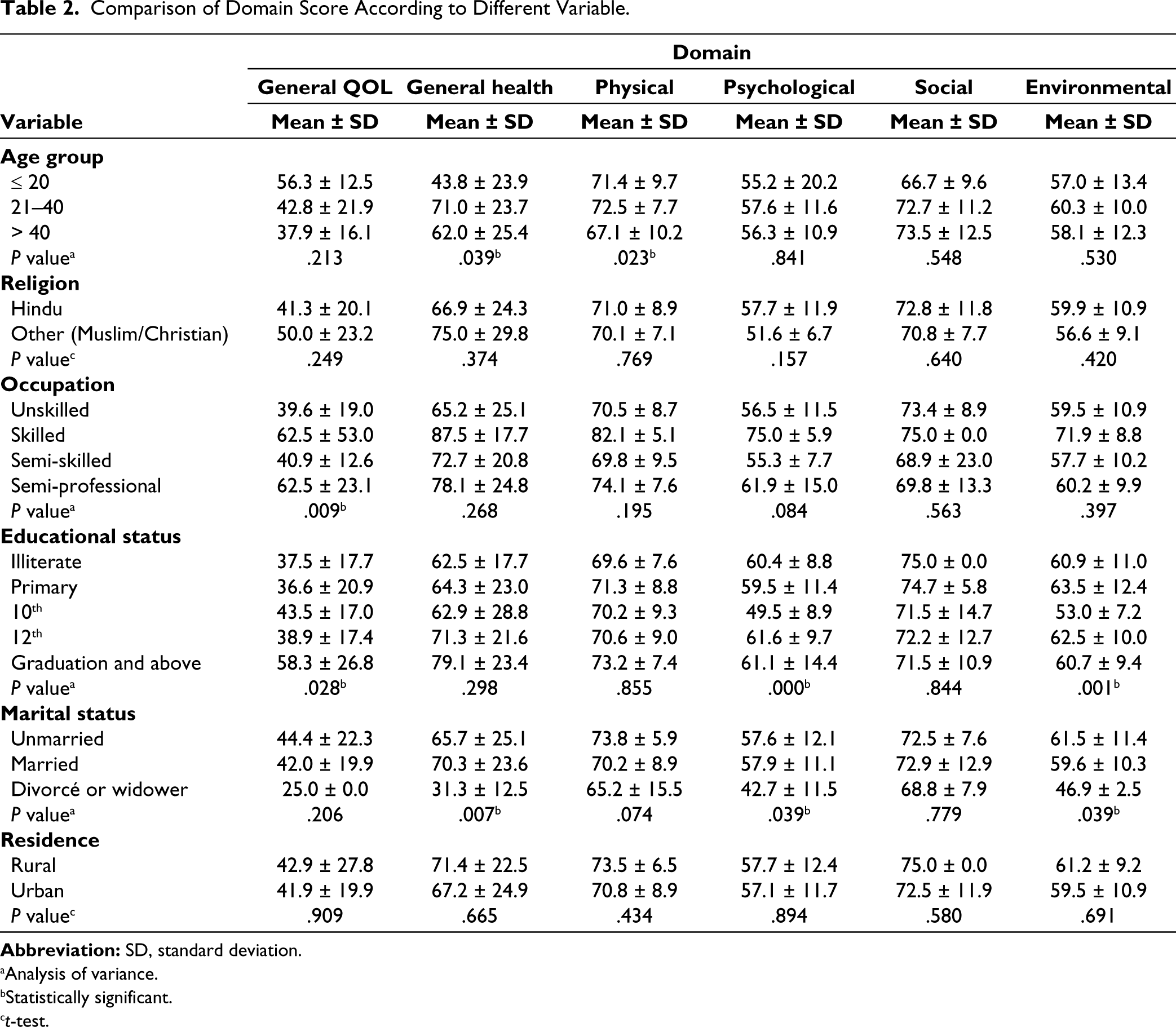
aAnalysis of variance.
bStatistically significant.
ct-test.
Correlation
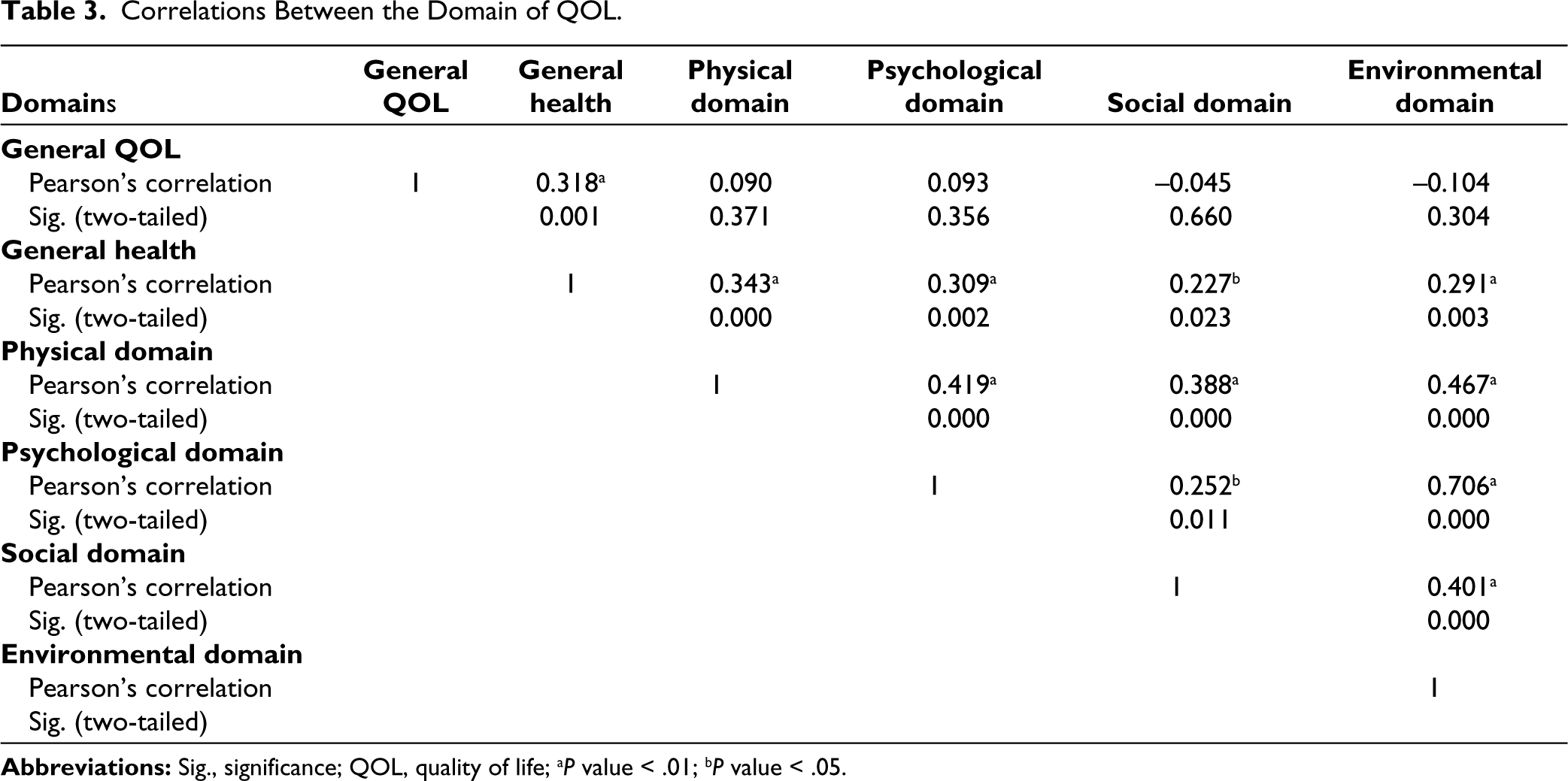
As observed, there were positive correlations between all four domains of WHOQOL-BREF, and they were statistically significant (Table 3). General QOL and general health were positively correlated and statistically significant. General QOL was positively correlated with the physical and psychological domain, and negatively correlated with the social and environmental domain; however, those correlations were not statistically significant. A positive correlation was seen between general health and scores obtained from all four domains, and those correlations were found to be statistically significant too.
Correlations Between the Domain of QOL.
Discussion
Our study aimed to assess the QOL among MSM. The results provide a snapshot of QOL among MSM in India, and how the QOL domains (physical health, psychological health, social relationships, and environment) were associated with a variety of adjustable determinants of health. Results showed that among our study participants, the highest score, reflecting better QOL, was obtained in the social relationship domain, while the lowest score, indicating poor QOL, was obtained in the psychological domains. No study evaluated the QOL of MSM from India in the current literature using WHOQOL-BREF. However, a study from United States assessed the QOL of MSM and found the lowest mean score in the social relationship domain, contrary to our study result. 16 Contrary to what Liu et al. reported that we found no association between different socio-demographic characteristics and social domain. 16 However, a similar finding regarding the correlation between the social relation domain and general health, physical, psychological, and environmental domains was reported. The possible difference in the score of the social domain can be attributed to cultural and geographical comparability. As the social relationship domain includes personal relationships, social support, and sexual activity, it could be possible that most of the men among our study participants were married to the opposite gender, may be without revealing their MSM status, and this did not impact the social relationship as they lived like any other men. However, our data did not collect information on whether they revealed their MSM status to their partner, family members, or friends. Also, we did not collect data on detailed sexual orientations, that is, homosexual or bisexual.
The results of our study showed that the psychological domain had the lowest score among the four domains of QOL, indicating poor QOL in psychological aspects. This finding highlights the importance of addressing psychological well-being. However, contrary to our result, Zhu et al. and Ramadhani et al. reported the lowest score in the environment domain.10,17 The study also found a significant correlation between the psychological domain and other domains, including general health, physical well-being, social relationships, and the environment. This connection between the psychological and other domains highlights the complex interplay between different aspects of well-being. This supports previous studies showing that psychological well-being is closely linked to overall health and other aspects of life.10,16 In addition, the relationship between psychological well-being and educational level among participants was found to be significant. Evidence suggests that individuals with lower levels of education experience greater stress levels and poorer mental QOL scores than those with higher levels of education.9,18,19 The psychological domain encompasses a range of factors such as emotions, self-esteem, body image, and appearance, and it is not surprising that the prevalence of psychological issues is high among MSM due to the stigma and discrimination they face. Addressing these psychological issues is crucial for improving the overall QOL of MSM.
The score of general QOL was the lowest, if we consider the general QOL, general health, and four domains (physical domain, psychological domain, social relationship domain, and environmental domain). Consistent with prior research, the occupation and education levels of the participants were significantly linked to their overall QOL.16,17 Additionally, age was a significant factor in determining the general health and physical QOL, which aligns with findings from previous studies.18,20 Environmental health was also significantly associated with participants’ educational and marital status; however, these relationships varied across studies.16,18,20 These findings highlight the complex interplay between various demographic factors and QOL outcomes. Understanding these associations can inform the development of targeted interventions and policies to improve the QOL for individuals across different backgrounds and life stages.
Based on the study findings, the care provider should be focused on the psychological issues of MSM individuals to improve their QOL. In addition, research should be undertaken to identify the underlying causes of the poor QOL across the psychological domain, preferably through qualitative or mixed-method research. Comparing the QOL between heterosexual men and MSM would give more insight. Finally, a multicentric study on the QOL of MSM is recommended to overcome the issue of the generalizability of our results.
To our knowledge, this is the first study to examine the QOL among MSM in India. However, there are certain limitations to this study that must be acknowledged. First, it was conducted at a single center using nonprobability sampling techniques, which may limit the generalizability of the findings to other MSM populations in India. Additionally, certain essential variables such as socioeconomic status, sexual orientation, and duration since last sexual intercourse were not recorded, which may have implications for the interpretation of the results. It is essential to recognize these limitations to interpret the study’s findings accurately and guide future research. Future studies with larger and more diverse samples, as well as more comprehensive data collection, can provide a more robust understanding of the QOL experiences among MSM individuals in India.
Conclusion
Psychological health is a crucial component of QOL and was found to be poor among MSM in this study. This finding underscores the necessity of addressing a broader range of health issues beyond HIV/AIDS, incorporating strategies to improve psychological health, and consequently, enhancing overall well-being and life satisfaction in this high-risk population.
Footnotes
Acknowledgements
The authors would like to thank the study participants for their time and involvement in this study. A special thanks to Mr. Hasan Khan, project manager, Targeted Intervention Program (MSM), Sagar, and other volunteers of Tumul Social Fundamental Development Society, Sagar, for helping in conducting the survey. Finally, we would like to thank the Madhya Pradesh State AIDS Control Society (MPSACS), Bhopal, India, for approving the use of registered data for recruitment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Ethical Committee of Bundelkhand Medical College, Sagar (IECBMC/2021/50) and from the Research and Development Division of Madhya Pradesh State AIDS Control Society (R&D/2021/361).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from all participants before data collection.