
Abstract
Aims:
The purpose of this analysis was to identify bivariate correlates of history of prior incarceration, and self-reported risky sexual practices among a sample of adolescent male detainees.
Methods:
The current analyses included 139 male adolescent offenders enrolled in an AOD/HIV prevention intervention conducted in a juvenile detention facility in a major Southeastern city in the USA. Significance tests were conducted using univariate logistic regressions to examine the independent associations of prior arrest history, and self-reported risky behaviors prior to this recent incarceration.
Results:
Adolescents who identified as having a prior arrest history were more likely to report they had willingly had sex with a prostitute (OR = 2.78, 95% CI = 1.29–5.95), used alcohol or other drugs to get a desired effect (OR = 3.39, 95% CI = 1.18–9.68), had tattoos (OR = 4.18, 95% CI = 1.78–9.78) and were addicted to AODs (OR = 2.51, 95% CI = 0.77–8.16).
Conclusion:
Findings suggest that risk practices that increase risk for STIs among adolescent male offenders, maybe a function of incarceration history.
Sexually transmitted infections (STIs), including HIV, are considered one of the most significant health threats to adolescents.1-6 Although rates of HIV/STIs diagnoses are not uniform among adolescents, what is known is that African Americans and incarcerated populations are disproportionately affected by the epidemics of HIV and STIs; particularly those residing in urban areas in the Southeastern U.S.7-13
Given that HIV/STI-associated risk, practices are common among this population, understanding the relationship between risky sexual behaviors and alcohol and other drug use (AOD) is of paramount importance. 11 Much of the literature supports this observation with other populations, including men who have sex with men (MSM), intravenous drug users (IDUs), young heterosexual women, and inmates.14-17 Although the majority of HIV-infected persons in the US, are either MSM and/or IDUs, 8 data note that the proportion of infected persons who are young adolescents is rapidly increasing.8,9 Adolescent juvenile detainees are a subset of this population that is uniquely at risk through both AOD use and risky sexual practices.18,19
Several perspectives have been proffered to explain why adolescent offenders are at greater risk for STI’s including HIV.20-22 Among adolescents, for instance, epidemiological studies have consistently shown that those who engage in delinquent activities are particularly at risk for HIV. 20 Studies have also revealed that adolescent detainees had less knowledge about HIV and lower efficacy in preventing the spread and contraction of STIs including HIV. 18 Moreover, it is documented that behavioral risk factors such as multiple partners, injection drug use, and unprotected intercourse are also prevalent among adolescent detainees, as well as being sexually active prior to being booked and having a history of multiple sexual partners.3,20,23-26 As a consequence, these multitude of factors contribute to tendencies for risky sex among adolescent detainees that increase their risk of STIs.
Adolescent detainees are considered to be at a higher risk for HIV for several reasons including (a) early age at first intercourse; (b) less frequent use of condoms during sex; (c) less HIV-related knowledge; (d) lower perceived susceptibility to HIV infection; (e) less self-efficacy to engage in preventive behavior; (f) higher levels of psychopathology; (g) different patterns of HIV risk factors; and (h) more permissive attitudes toward sex.11,27,28
Unfortunately, one factor missing from the examination of risk for STIs among juvenile adolescents, male or female, is the extent to which prior incarceration or one’s incarceration history affects prevalence of risk behaviors and practices. Given the aforementioned factors confronting adolescents involved in the correctional system, the purpose of this analysis was to identify bivariate correlates of incarceration history and risky sexually practices among a sample of juvenile adolescent offenders
Methods
Data were collected from youth participants over a 15-month period of time. Detained youth were recruited and enrolled in the study, from Youth Development Campuses (YDCs), by trained research staff. The YDCs housed youth who were sentenced to serve no more than two years. Prior to this investigation, IRB approval was obtained from all affiliated agencies (Georgia Department of Juvenile Justice and Emory University Institutional Review Boards). Both participant assent and parental consent were required for participation in the study. Once the consent process was completed, participants were administered a questionnaire by trained interviewers in a private location within the YDC. Each participant was provided with a unique identifier that was used on all surveys collected from the participants. All data collected during the course of the project was stored in a secured file cabinet and data were later entered on a secured computer. This analysis was conducted using baseline data.
Sample
Participants in this study included 139 male adolescent offenders enrolled in an AOD/HIV prevention intervention conducted in a juvenile detention facility. To be eligible for the study, youth had to be scheduled for release from the YDC facility within 90 days. Participants were excluded from the study only if they refused to provide informed assent and/or their parents (or legal guardians) refused to provide written consent for participation. No participants suffered from severe cognitive or psychiatric impairments (e.g., psychosis) that would have compromised their ability to complete the assessment. All adolescents were fluent in spoken English.
Instrumentation
Demographics: Participants reported their age, race, and years of formal education, length of incarceration, and prior arrest, among a number of demographic variables. Incarceration History was specifically measured using a single dichotomous item selected from the survey instrument that asked participants “Have you ever been locked up before this time?”
Risky behaviors were assessed with 14 self-report dichotomous items that asked about participants’ activities prior to their current incarceration. Example items include “Have you ever willingly had vaginal sex?” “Have you ever willingly had five or more alcoholic drinks in a day?” and “Have you ever had sex with a prostitute?” A more detailed description of these items and the survey instrument have been published multiple times previously.10,11
Instrument Validation
Existing measurements were used in order to increase instrument validity when possible. When existing measures were not available items were adapted or developed for the purposes of this study. All substance use variables were measured using an adaptation of the Centers for Disease Control’s (CDC) Youth Risk Behavior Surveillance (YRBS) questionnaire and additional problem behaviors were obtained using a scale based on the Seattle Survey Instrument (Hindelang et al., 1981). These have demonstrated to be very reliable and valid measurement instruments historically.30,31
Analysis
Associations between dichotomous correlates were assessed by contingency table analyses. Due to the retrospective nature of the study, risk ratios were computed to provide an estimate of relative risk for adolescents who were repeat offenders versus first time offenders. This status was determined by a participant’s response to the item: “Have you ever been locked up before this time?” This was a dichotomous yes or no response item. It should be noted that participants were informed what the item meant prior to the survey administration. Thus, the use of univariate logistic regressions to examine the independent associations of these variables, is presented in the form of adjusted odds ratios (ORs) with 95% confidence intervals (CIs).
Results
The mean age of study participants was 15.52 years (SD = 1.03) and they reported spending an average of 47.5 days incarcerated prior to survey administration. Participants reported their age of first drinking alcohol and using marijuana as being 12.9 (SD = 2.61) and 12.3 (SD = 2.3) years of age, respectively. Overall, participants reported having 2.29 (SD = 2.68) tattoos and that they first willingly had vaginal sex at age 12.7 (SD = 2.06) years of age. More than two-thirds (60.4%) reported being incarcerated before the time of data collection.
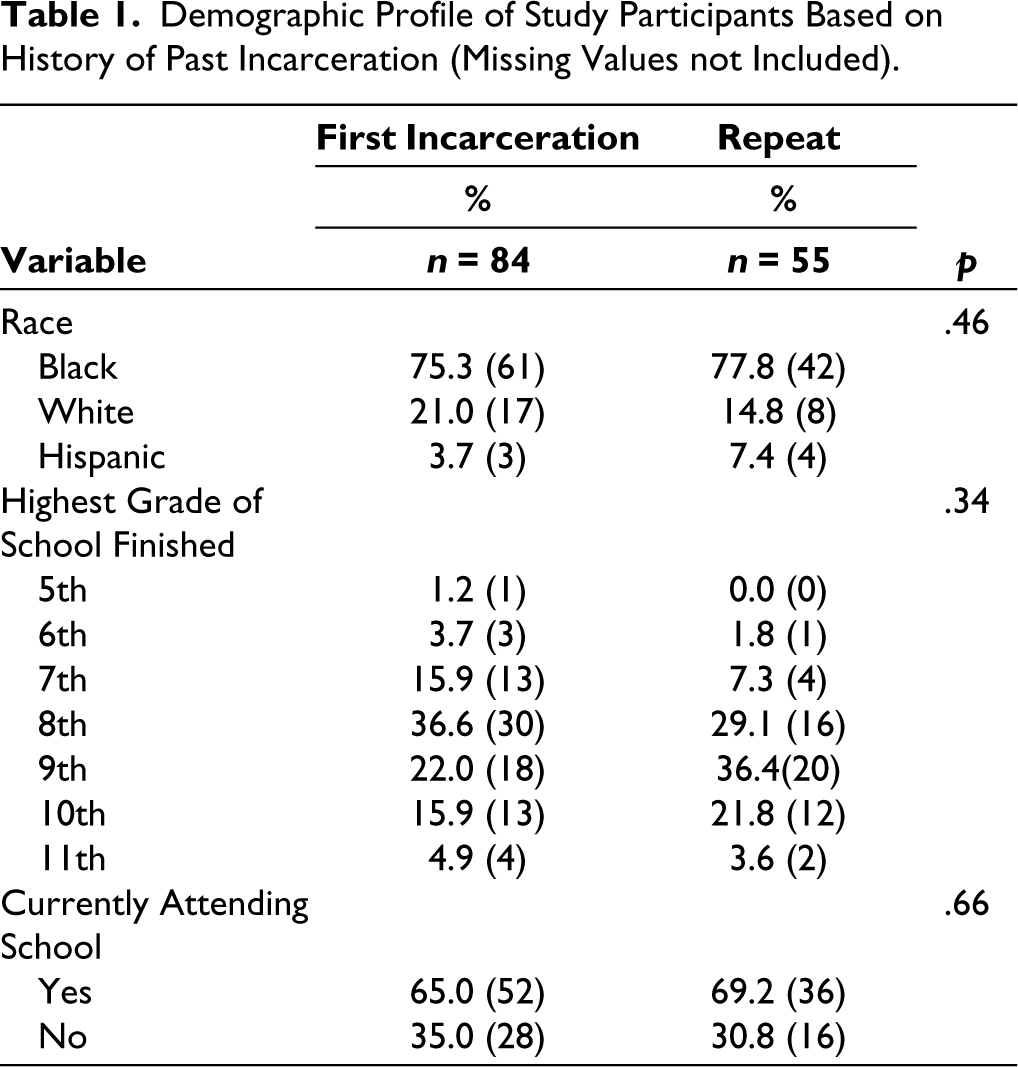
The majority of study participants self-reported Black/African American (76.8%) with whites and Hispanics comprising 18.5% and 5.1% accordingly. With respect to education, the majority of the sample respondents had attended school up until 8th grade (34%) followed by 9th grade (28%). Only 2.3% indicated attending school up to grades 10 and 11. Regarding sexual behavior, on average, males reported age of first having vaginal sex at 12.8 years (SD = 1.77) and oral sex at 14.1 (n = 284, SD = 1.67) years. Given participants were not of age to provide for themselves economically, no information was collected from parents related to their socioeconomic status although they lived in communities where over 70% received some form of federal government assistance.
Adolescent males who reported being incarcerated previously had a mean age of 15.2 (SD = 1.2), were 12.8 (SD = 2.34) years of age when they had their first drink of alcohol, 11.9 (SD = 2.19) years of age when they smoked marijuana, had 2.34 (SD = 1.97) tattoos and were 12.7 (SD = 1.51) years of age when they are first willing had vaginal sex.
Adolescent males who reported this was the first time they had been incarcerated had a mean age of 15.7 (SD = 0.96), were 13.3 (SD = 2.46) years of age when they had their first drink of alcohol, 12.4 (SD = 3.25) years of age when the smoked marijuana, had 1.73 (SD = 2.37) tattoos and were 12.7 (SD = 2.69) years of age when they are first willing had vaginal sex. Based on Chi-square analysis, there were no statistically significant differences between both groups of participants in terms of ethnicity and education as detailed in Table 1.
Demographic Profile of Study Participants Based on History of Past Incarceration (Missing Values not Included).
Bivariate associations between the groups assessed prior arrest history correlates and self-reported STI risk behaviors (e.g., yes vs. never) as well as corresponding prevalence ratios and their 95% confidence intervals are presented in Table 2. Table 2 also serves a descriptive purpose by showing the proportions of those who reported having been arrested previously, and those who did not, with respect to their agreement or disagreement with selected correlates. Of note, eight of the 14 correlates indicated that prior arrest was a potential risk factor. Associations were based on remarkably similar proportions (i.e., the difference between groups was extremely small).
Bivariate Logistic Regression of Prior Arrest History and STI Risk Behaviors Reported by Male Juvenile Offenders.
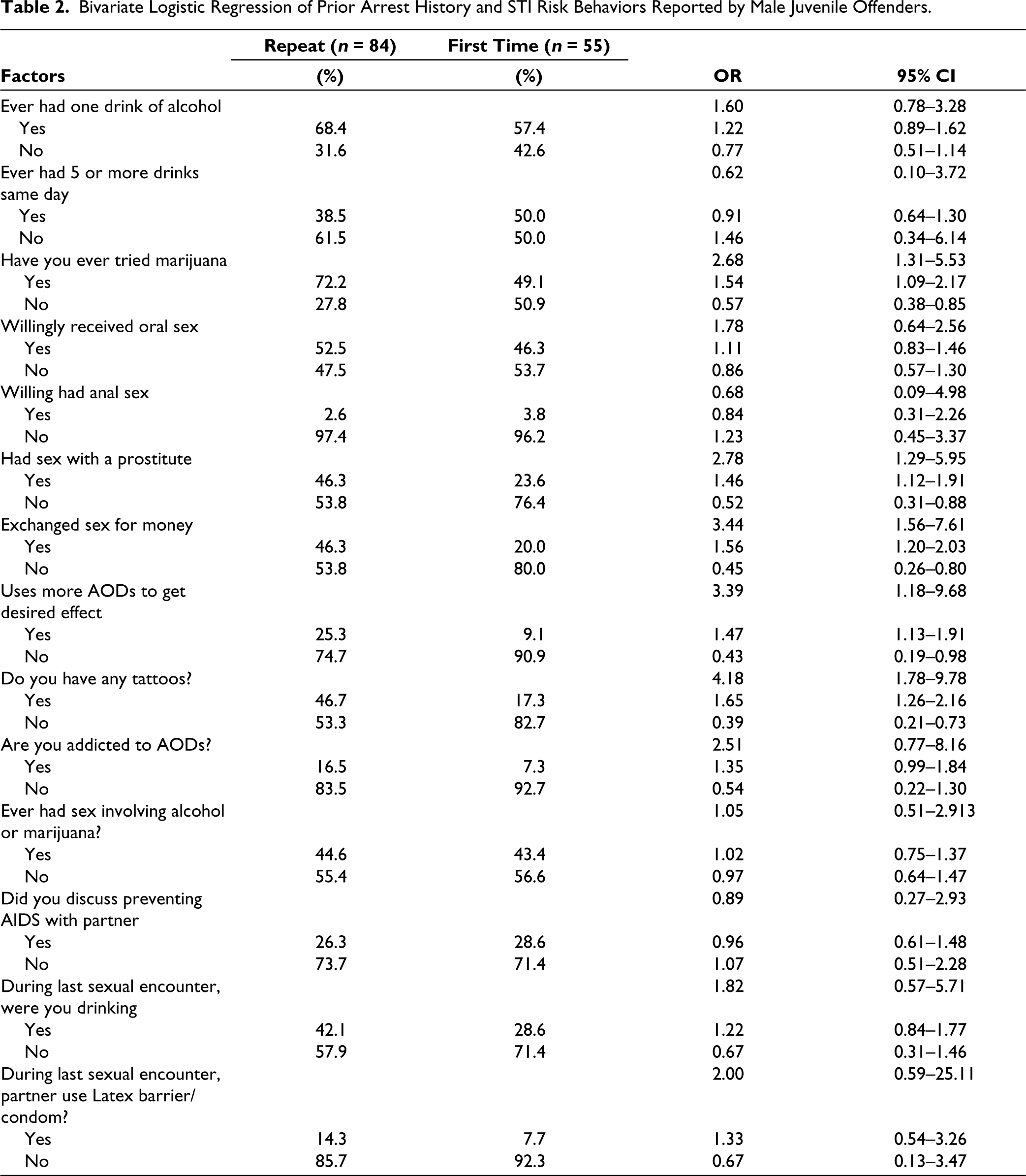
Male juveniles who reported having been arrested previously were more likely to indicate that they drank alcohol (OR = 1.60, 95% CI = .78–3.28) and tried marijuana (OR = 2.68, 95% CI = 1.31–5.53) before the current incarceration, than those who had not been previously arrested. In addition, they were more likely to have reported willingly receiving oral sex (OR = 1.78, 95% CI = .64-2.56) and willingly having sex with a prostitute (OR = 2.78, 95% CI = 1.29–5.95). Moreover, they reported exchanging sex for money (OR = 3.44, 95% CI = 1.56–7.61), using more AODs to achieve a desired effect (OR = 3.39, 95% CI = 1.18–9.68), having more tattoos (OR = 4.18, 95% CI = 1.78–9.78) and being addicted to AODs (OR = 2.51, 95% CI = 0.77–8.16). Strangely, they were two times more likely to have reported using a condom during their last sexual experience prior to current incarceration (OR = 2.00, 95% CI = 0.59–25.11).
Discussion
Results of this study indicate distinctive differences between youth with and without a history of prior incarceration with respect to substance use problem behaviors. AOD-involved risk behaviors other appear to drive the behavior of adolescent included in this investigation. In this sample of male adolescent offenders, more than two-thirds reported a history of being arrested previously. Since there is limited looking at prior arrest history among a sample of male adolescent offenders and the targeted STI risk behaviors included in this investigation, it is difficult to corroborate findings with other studies examining this same population. Although indistinguishable in terms of criminal activity and abuse and dependency of most substances, study participants were more likely to perceive they were addicted to AOD use. This is an important observation given that substance abuse is demonstrated to be associated with increased hyper-sexuality and subsequently a heightened risk of contracting a STI. 32 In addition, this study noted an association between juvenile arrest history with marijuana use, AOD use, having sex with prostitutes, and exchanging sex for money, which has been observed in other studies.32-34
Although the findings indicate that the magnitude of the associations observed are substantial, it is the consistent pattern of associations observed across these different outcomes that the consistent pattern of associations observed across these different outcomes is particularly concerning. Research in the field of male adolescent offender STI risk behaviors may provide a useful framework for understanding the association between adolescent belief orientations within the context of correctional settings. Consequently, those who have experience within correctional settings may perceive themselves as limited in their vulnerability to contracting and spreading an STI, which in turn may reduce the likelihood of practicing safer sex. 35
In addition, their own experience of abuse may shape their beliefs regarding what is an STI risk. Having an STI may be considered normative and adversely result in the development of perceptions about safer sex and healthy relationships that may increase personal risk—all of which have implications for clinical and public health practice. Public health educators serving adolescents, in particular, male adolescents with a prior history of incarceration may need to provide a comprehensive risk assessment that includes screening to develop and or implement counseling and education, including resources on pregnancy, STIs, and HIV prevention.
The self-reported differences in condom use, observed among participants, are important given the high prevalence of STIs including HIV, among this population, particularly in the Southern U.S.20,22,36 There may be practices and/or beliefs by adolescent offenders, males especially, that manifest themselves in some form or self-efficacious belief or practice that requires additional and detailed investigation. Still, these findings add to the collective empirical database indicating that more behavioral interventions for juveniles in correctional settings should be employed for this high-risk population.
Although our findings are unique and clearly add to the current corpus of research, this study is not without limitations. First, the findings may not be applicable to male adolescent offenders in other regions of the country or globe, as well as to adolescents in general with different sociodemographic characteristics or risk profiles (e.g., injecting drug users). Moreover, the reliance on a methodology that involves the use of self-reported outcome measures (i.e., sexual behaviors and substance use) may bring about concerns pertaining to reliability of our findings and results. Prospective Investigations are desirable to differentiate the course of youth behaviors in relation to infectious disease since, findings herein may not generalize to youth populations with less severe AOD use and without judicial involvement. Although a multitude of studies have supported validity and reliability of self-reported sexual behavior,37,38 none examined juvenile detainees who were predominantly African Americans.
Based on the findings of this study, several approaches may be used to inform clinical practices for intervention design and implementation. First, since this population is culturally diverse; practitioners may want to consider employing culturally sensitive approaches that target problem behavior risks associated with sexual risk-taking and substance use. Thus, behavioral interventions may need to be employed to accommodate the age of adolescent male offenders, given that older juvenile offenders than younger ones may require more effort. Consequently, these may need to target improving decision-making and communication skills associated with both substance use and sexual behavior with their peer groups. This is essential because many of our sample respondents reported being sexually active prior to incarceration. This suggests that delaying the commencement of sexual activity, and inspiring abstinence among youth who have previously been sexually active is not an efficacious practice.
Clinicians working in juvenile correctional facilities may also want to consider offering SRTI and substance use reduction programs specific for youth who have not been incarcerated previously separately from those with a history of prior incarceration, since higher-risk youths may necessitate more rigorous services.
Conclusion
In the absence of a vaccine, there is a clear and distinct need to develop new and innovative intervention research to optimize intervention effectiveness for vulnerable populations to reduce their risk for HIV infection.3,39-42 This is a particularly salient need given a majority of adolescent offenders are a vulnerable subgroup of adolescents. The value of such programs is buttressed and magnified by the needed public health benefit of averting the growing issue of STIs and their spread among correctional populations and the communities to which these individuals eventually return.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
IRB approval was obtained from the following organizations: Emory University Human Research Protection Program and the Institutional Review Board of the Georgia Department of Corrections as study was determined to have met all ethical standards of approval.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institutes on Alcohol Abuse and Alcoholism Grant #RO1 AA015018.
Informed Consent
Written informed consent for program participation was obtained from parents or guardians to request permission for subject participation.