
Abstract
This study explores primary carer’s experiences concerning the emerging sexuality of adolescents with intellectual and developmental disabilities (IDD) in different cultural and social contexts. Potential studies were collected from four databases: PubMed, Scopus, Science Direct, and Web of Science. Eighteen studies were met the inclusion criteria and published in the year between 2010 and 2022. Four themes were synthesized: Parental perceptions of sexuality, experience of confusion and dilemma, individual needs and uniqueness of the child, and primary carer’s needs. This study highlighted the need for equipping primary caregivers with knowledge and skills to manage and educate the child about sexuality and sexual health.
Keywords
Introduction
Adolescents with intellectual and developmental disabilities (IDD) have similar sexual and reproductive needs as their typically developed peers yet face impassable barriers in fulfilling their needs. 1 Historically, individuals with IDD were treated as asexual beings. In the past few decades, the sexual health and sexual needs of individuals with IDD have received increased recognition, and the significance has been highlighted internationally.2,3
Studies pointed out that the challenges regarding sexuality and sexual health are more among adolescents with disabilities than those without disabilities, and adolescents with IDD are at higher risk of sexual abuse.4,5 The cognitive and other developmental issues associated with ID make adolescents with IDD more vulnerable. Poor situational perception, lack of problem-solving and decision-making capacity, and lack of other appropriate skills significantly affect the ability of adolescents with IDD to maintain their sexual health and well-being. 6
Compared with typically developing counterparts, children with IDD are more isolated from society and live much of their time under greater dependence on their parents or caregivers. 7 Parents are crucial in molding the attitude toward sexuality and puberty in adolescents regardless of their disability status. 8 The role of parents is more significant in children with IDD because of the continued dependency and vulnerability. 7 Lack of parental knowledge about sexuality may result in an increased risk of sexual exploitation and sexually transmitted diseases (STDs) of persons with IDD. 9
The study is a qualitative meta-synthesis of empirical studies from January 2010 to September 2022 that aims to lay out the global evidence on primary caregivers’ experience relating to the emerging sexuality of adolescents with IDD. The specific research objectives addressed in this study were: (a) primary caregivers’ concerns about the sexuality and sexual health of adolescents with IDD; (b) primary caregivers’ perceptions of the sexuality and sexual health of adolescents with IDD; (c) primary carer’s needs and support systems concerning the sexuality and sexual health of adolescent with IDD. In this study, we interchangeably used the terms parent, primary carer, and primary caregiver to indicate the person who provides maximum parenting time to the adolescent with IDD.
Methodology
Meta-synthesis is the systematic review and integration of qualitative study findings that follow a methodology for collecting, analyzing, and interpreting the results of various studies and, as a result, developing overarching interpretation by merging the interpretations of the empirical studies included in the synthesis.
10
To answer the formulated research objectives, four databases, including PubMed, Web of Science, Science Direct, and Scopus, were utilized for a systematic search during November 2022 and December 2022. Search in databases was performed using the following terms as text words: adolescents OR teenagers AND intellectual disability OR developmental disability OR mental retardation AND primary caregivers OR parents AND Sexuality OR sexual and reproductive health AND sexuality education AND puberty. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed to identify studies,
11
and the procedure is depicted in Figure 1. A good number (around 1185) of studies were placed, and then the following criteria were applied:
Published in a peer-reviewed journal and English. Used qualitative methodology. Published between the period of 2010 (January) to 2022 (September). Focuses on primary caregivers’ experience of the sexuality of adolescents with IDD. Studies including the primary caregivers of adolescents with ID within the age group of 10-20 years with IDD.
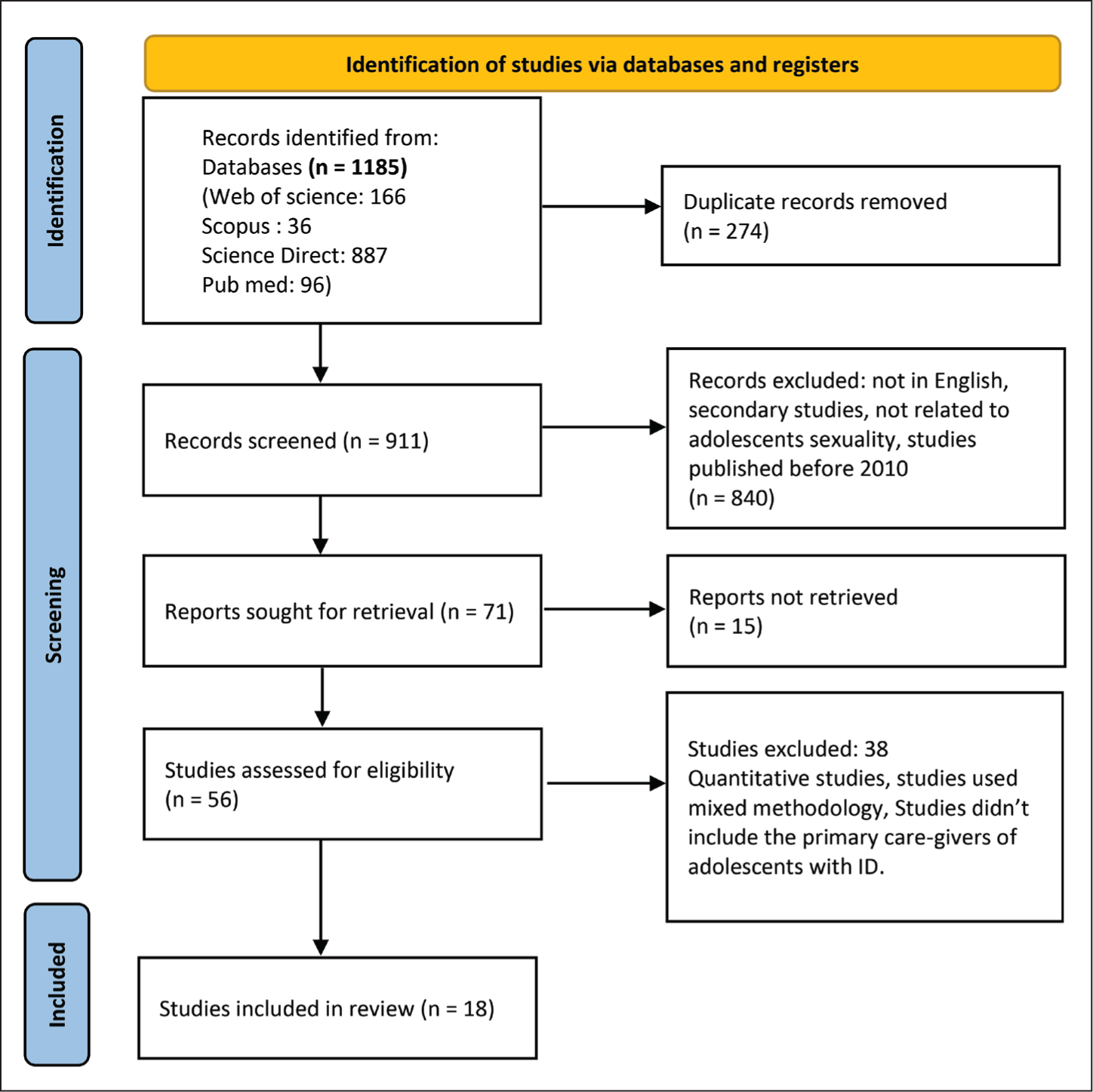
Several studies were excluded because of the conceptual nature of the articles, and a few were excluded due to the use of other methodologies (quantitative or mixed) and an inappropriate study population.
We selected the studies separately by screening the study titles, abstracts, and full texts when needed to decide whether they were eligible for meta-synthesis. The potential studies were read and re-read, and each article was analyzed based on methodology and quality appraisals. The Critical Appraisal Skills Programme (CASP) 12 guided the quality appraisal, and a detailed depiction is provided as supplementary material. The CASP 12 consists of ten questions that enable the evaluation of qualitative studies. The score assignment for each CASP question was adopted from the works of Rushbrooke. 13 Thus, each question was scored as zero, one, or two, indicating little or no information, moderate information, and fully addressed information. articles scored above ten were included in the review, and others were excluded. Finally, 18 studies were included in this study.
We used Thomas and Harden’s method of thematic synthesis to integrate the findings of various qualitative studies. The three stages followed were: “line-by-line” coding of text, “descriptive themes” development, and “analytical themes” generation. 14 The selected studies’ verbatim were entered and coded, and themes were generated using the qualitative analysis software QDA Minor.
Result
Among the 18 studies, 10 were from developed nations like the USA (n=4), UK (n=2), Canada (n=1), Ireland (n=1), Australia (n=1), and Scotland (n=1). Eight studies were identified from developing nations, including four from Turkey and one from India, Malaysia, Iran, and Israel. In eight studies, the participants were mothers. Nine studies included both mothers and fathers, and one study had parents, siblings, and close relatives who provided primary care to individuals with IDD. 15 Fourteen studies were focused on the primary caregivers of both boys and girls, three were focused only on girls,16-18 and one was focused on boys. 19 The sample size of the selected studies ranged from 5 to 27 primary caregivers. The most used data collection method was semi-structured interviews, and the commonly seen analysis was interpretative phenomenological analysis. More details are provided.
The following themes were synthesized:
Theme 1: Parental Perceptions of Sexuality
Many primary caregivers assumed that children with IDD were asexual and unable to lead a sex life,20-22 and some even opinioned, “I do not see any changes in terms of sexuality. I don’t think so.” 20 Some parents perceived that information about sexuality was irrelevant to their children, 23 and the ignorance was reflected in their words: “… It seems to me that she doesn’t have a sexual need.” 24 Many parents were oblivious to the sexual needs of girls and viewed they lacked sexual desires, unlike boys: “She is a girl; girls don’t feel things like boys.” 25 Parents used to compare their childhood with their child’s childhood and conclude that there is no sexual desire for children. 22
Religious, cultural, and family background influences the parental perception of sexuality. These backgrounds reinforce their belief that sexuality is something shameful: “My family taught me that sexuality is a shame and it should not be talked about.” 24 In the same way, parental embarrassment due to socio-cultural background was another problem that hardened the parent-child interaction regarding sexuality.15,26-28 For instance, “I treat everything as if it’s just a natural thing; because it embarrasses me, I can’t talk about it.” 27 Parents were unwilling to accept and respect the sexual needs and rights of adolescents with intellectual disabilities due to their socio-cultural background. 15,16,25
Caregivers felt that providing information about sexuality would create obsession and generalization among children and lead to habit formation.19,20,23,25 One parent stated, “I don’t want to teach him too much about it also, being a boy, he will keep doing this all day then.” 25 Similarly, caregivers feel that information about sexuality will harm their children and believe that communication will arouse sexual feelings in children and create curiosity among them:16,25 “It is better if we do not provide information to them because it might stimulate their sexual desire.” 16 Parents perceived that the expression of sexuality in children is scary sinful and something should be banned because it is morally inappropriate.21,26,29 “I always warned and forced him to leave that handling. You will not. I said shameful and sin.” 21 Parents suppress the expression of sexuality of their children due to their unawareness. “She wants to be in love and kiss and tries to attract the attention of handsome men, but we suppress her feelings and destroy her imagination…” 24
Studies revealed that parents shared that “I knew it (menstruation onset) would happen” 25 but were not prepared for the changes associated.17,20,25 For some parents, puberty onset was a hope for marriage because the child can carry and deliver the baby in the future. It was perceived that taking up socially valorized positions like husband or wife or parents would help to cure ID:16,25 “Maybe he will get cured after marriage. I have heard of cases where children are cured after marriage or after having relations (sexual relations) and children.” 25 On the other hand, some utterly rejected the possibility of marriage or finding a partner for their children. In such cases, parents equated the term sexuality with intimate relationships and felt that information about sexuality was unnecessary considering the incapability to lead a married life.20,22-26 The attitude was mirrored as, “Why talk about sex with him when it will most likely never happen.” 23 Fear of stigmatization and societal criticism severely impacted parents. 24
Theme 2: Experience of Confusion and Dilemma
Primary caregivers consistently experienced uncertainty and dilemmas about the emerging sexuality of their child with IDD. The significant concerns experienced by primary caregivers were related to the security and behavioral patterns of children with IDD. Safety becomes a prime issue due to the potential vulnerabilities and consequent risk of abuse.19,28 Children with IDD struggle with social skills, such as the inability to comprehend boundaries, communication of emotions, and convey safety threats.18,21-24,27,28,30 The susceptibility to sexual exploitation led to parental concerns, reflected in their words: “Someone is going to take advantage because they don’t fully understand sexuality like a child their age.” 23
Many studies reported that parents were unaware, uncertain, and inefficient in dealing with children in their pubertal changes and the resulting sexual behaviors. Parents also expressed the dilemma in resolving the queries raised by the child with IDD: “Once he asked his dad why it (penis) was standing the way it was, he didn’t know how to explain it to him.” 25
Similarly, primary caregivers were anxious about the behavioral issues associated with puberty among children with IDD. They shared: “…..when he started changing, my first thought was behavioral issues… How will we manage if he refuses to obey or gets angry? He is getting stronger, you see?.” 25 Also, witnessing sexual behaviors exhibited in public by children made parents annoyed, embarrassed, and angry:22,29 “She exhibits behaviors such as rubbing herself on the armchair. She even does this at school and when we go to somebody’s house… However, this annoys her father, we are embarrassed.” 29 Primary caregivers, especially mothers, face difficulties regarding the management of sexual behaviors of adolescents with an ID, stating: “He was trying to fulfill this need with me, as he could not distinguish the concept of mother. He wanted to caress my arms and legs.” 24
Parents were also concerned that others misinterpreted their adolescent’s nonsexual behaviors as sexual and pointed out scenarios like, “If you have a pattern on your shirt and he likes it, he is going to touch it, not because he wants to touch your breasts but because he wants to feel the shirt.” 23 Some of the parents were even confused about whether their child’s particular behaviors were sexual expressions or not. 26 The confusion was shared as “I don’t know if it’s sexual. I don’t know if her feelings are that way…” 26
The dilemma between “autonomy vs. protection” was one concern experienced by parents. Parents must educate and prepare their children for adulthood while ensuring their child’s safety and well-being. Hence, parents need to balance the appropriateness of information they communicate with their children regarding sexuality; “I think as a parent you want to back off a wee bit as well, but you don’t want anything to happen, so it’s getting the divide between, the balance between knowing when it’s appropriate to let go safely.” 26 Parents isolate and control their children from the social environment because of their fear of the inappropriate expression of sexual behaviors by children.16,21,24 Further, the personal traits of children with ID, like blind trust in strangers, create fear in primary caregivers and increased risk of abuse, compelling parents to limit socialization opportunities of the children within the home and school.24,31
It was a common observation that due to safety concerns, parents tend to deny the right of their children to express and experience their sexuality. 15 Some parents were confused about who would initiate the conversation about sexuality, and usually, they concluded that the responsibility lay on the child20,26 and responded, “It is not his interest. He did not ask.” 20 In terms of marriage or intimate relationships, the burden of care is also a common opinion that is reflected as; “They cannot marry because the person to marry will necessarily be Someone with disabilities. And I don’t think I have the power to add; plus, the burden on my responsibilities.” 24
Theme 3: Individual Need and Uniqueness of the Child
Every child is different, and their needs are also different based on their level of intellectual functioning, physical development, level of dependency, and learning strategies.18,30,32 Sexuality education should be individualized28,32 as “the particular combination with each child of their level of intellectual functioning and physical development and physical ability and the way they relate emotionally is all so different.” 30 Parents were receptive to the information and suggestions from experts regarding sexuality but were very cautious about applying this information. 32
The presence or absence of concomitant disability makes children unique and different. 25 For example, “My daughter does not speak. If something happens, she won’t even be able to call for help.” 25 Parents shared that the ability of each child to understand and respond to the events differs as well: “I think it’s about the child’s understanding…..how much she can understand.” 21
Children will be of different capacities in terms of grasping new skills. While some children were quick in learning, “she is quite rigid in what she learns. If you can teach her exactly what you do, in an exact situation, she will be able to do it”; 27 for some, it’s an arduous task: “These children have an intellectual disability and can forget everything very rapidly.” 29
Approach to sexuality and expression of sexual behaviors also varied within the familial, social, and cultural scenarios:20,32 “When he was in standard 5, I taught him not to play with girls. He could not touch any girls because it is prohibited in Islam.” 20
The experience and needs further differ in terms of the gender of adolescents. Girls with IDD experienced puberty with changes like menstruation, body hair development, and breast development, but the developmental changes and associated conflicts were quite different in boys.18,19 Within girls, the experience of menstruation varied with the occurrence of menstrual symptoms, the ability of the child to manage it, and the support system. For example, some decided, “We’re gonna have to get rid of that because that’s gonna be hard for her to deal with,” 17 while others shared: “She puts her pad on herself, she takes it off herself and puts it in the bin.” 18
The children are further unique regarding their circumstances and the socialization opportunities they are exposed to. Children with ID have limited opportunities to meet with people and explore relations, which additionally vary among the children depending on the parental approach as well as the capacity of the children.20,26,31
Theme 4: Primary Carer’s Needs
Primary carers need strong support to overcome the barriers related to the sexuality of their child with ID. Parents were confused about what, when, and how to communicate with the child about sexuality: “When do I need to speak with her? She is 13 years old,” 31 and “I am of the opposite sex. How will he approach me, and how should I behave towards him?” 29 Parents were hazy about seeking help and showed a desire for guidance on sexuality matters of their children with ID. 31 Some preferred “a little guidance” as they “do not know where to go or what to say,” 31 and some felt “it should be given with the expert.” 21 They needed professional support on matters related to the sexuality of their child due to the lack of knowledge, poor confidence, stigma, and feeling of incompetence.21,23 Parents were also up for a collaborative approach in which they actively participate in sexuality education along with the professionals.23,32 For example, “I just think that the parents have to be involved in the conversation…. We need to all be at the same table talking about how we are going to do this together.” 32
Parents could get information and guidance about sexuality from peer parents, special educators, social workers, and healthcare professionals,17,18,23 and “being able to talk to other families and parents” could also make a big difference, but for this robust “support systems are important.” 17 Parents experienced a lack of efficient, professional support in clearing the doubts regarding the sexuality of the child: “I feel like I never quite get a straight answer out of [school] or the doctors.” 18 Parents suggested that they needed information rather than medication for their children and said, “the doctor prescribes medication… It is more important to be informed about this issue.” 21 A smaller number of trained professionals is another problem faced by parents: “I want child psychiatrists to be involved, but unfortunately, their number is very low in our country.” 21 Lack of quality time with professionals is another issue. “…I went to a psychiatry clinic. The doctors told me that they did not have sufficient time for sexual education.” 22
It is essential to look through the kind of support each primary caregiver requires and the commonly reflected needs in the studies where assistance related to behavioral issues, hygienic practices, and safety concerns about Sexuality.21,22,29 The available resources were limited to the provision of skills on personal hygiene. According to the parents, “The resources you would get for younger children aren’t detailed enough,” 15 and they were unsatisfied with the information and assistance provided.15,18
Parents suggested developing and utilizing more technology-based resources for training and managing sexual health among children with ID:18,28 “I’m all about technology with these kids. I think it’s a wonderful resource for them.” 28
Many want their children to have a happy and safe life over a married life in the future. 19 “It doesn’t matter if he doesn’t marry or have children….I just want him to be more independent, happy, and safe, and that’s it.” 19 Yet, as a parent, they feel sad when they cannot satisfy their child’s wish. 24 Apart from home and school, Parents dreamt of an inclusive world where their children can access various opportunities and activities: “I want him to have as wide a range of activities, places he can go to, that he can access.” 19
Discussion
Primary caregivers experience confusion and dilemmas associated with the sexuality of their child with IDD during adolescence. Parental perceptions of child sexuality play a pivotal role in the sexual and reproductive health of adolescents with IDD. 5 This study result shows that parents considered their adolescents with IDD as asexual beings.20,21 A scoping review on barriers to sexuality education in the WHO European region identified that society constructed children with IDD as asexual. 33 Still, contrary to this, a study among adolescents with ID reflected that 85% of the adolescents with IDD reported a desire for a romantic relationship. 34
The narrative review on sexual abuse indicated that the prevalence of sexual violence among children with IDD was 15% and showed increased risks for sexual abuse. 35 Consequently, the main parental concern was associated with the safety of children with intellectual disabilities.18,21-24,27,28,30 Sexual behavior of children with IDD is another concern experienced by parents concerning sexuality.16,19,25,30 The quantitative study in Australia shared that children with autism exhibit inappropriate sexual behaviors, poorer social behaviors, and a lack of knowledge about public and private space behaviors. Parents experienced concerns over these behaviors. 36 For the primary caregivers, ensuring their child’s autonomy without compromising security was a significant challenge. The study among pediatricians also exposed the dilemma between autonomy and protection when trying to provide the sexual rights and safety of the individual with IDD. 37 Across the studies, primary caregiver experience fears related to the sexuality of their child with ID because of their poor knowledge and insufficiency. Due to insufficient knowledge about sexuality, parents were scared to open the box of sexual and reproductive education to their children with IDD. 38 Parental concerns over sexuality were closely related to parental self-efficacy and their preparedness to manage the emerging sexuality of their child with IDD. 39 Parents require support and assistance from health professionals, social workers, and special educators on sexuality.21,22,29,31 Various studies pointed out that parents’ involvement in care planning for these children will improve the quality of care and enhance the treatment outcomes.40,41 Hence, as a primary step toward sexuality education for children with IDD, it is critical to equip and empower parents regarding their knowledge, attitude, and practice on sexual and reproductive health.
Socialization opportunities for children with IDD were minimal26,31 due to parental concerns and societal stigma. The study in Africa identified different barriers affecting socialization opportunities, including social exclusion, absence of resources, and level of functioning. 42 Similarly, an Australian study found that adolescents with a disability experience higher bullying victimization. 43 The study in South Africa pointed out that contextual factors, such as socio-cultural background, interpersonal interactions, and structure of various institutions, impacted the implementation of sexuality education for adolescents with IDD. 44 Creating a safe environment for the inclusion of children with ID could eliminate the fear of parents and enhance social participation.
Children with IDD are different in terms of their functioning and support needs.18,30,32 Studies found that individualized support on sexuality is essential due to the diversity among children and families and suggested tailor-made interventions.45,46 Additionally, various studies argued about developing and implementing sexuality education curricula according to the cognitive and affective domain of children as supplementary to individualized education.47-49
Developing and using technologically advanced devices to assist children with IDD is another need of parents.18,28 A systematic mapping study on technology-enhanced and game-based learning shows that it benefits enhancing the cognitive, social, and motor skills of children with IDD, 50 and the impact of similar techniques on sexuality education has to be investigated in the future.
Future Directions for Research
First, there is a shortage of knowledge about the sexual and reproductive health scenario of adolescents with IDD from least developed nations. The main reasons for the underrepresentation of studies from developing countries or least developed nations due to lack of resources, poor amenities, and inadequate technical support and training. 51 Second, the reported studies should mainly focus on primary caregivers’ safety and behavioral concerns about their child with IDD. Apart from this, studies should focus on the strength perspectives like happiness, relationships, mutual understanding, and rights. Third, studies mainly focused on adolescent girls with IDD and issues like menstruation and safety problems and overlooked the sexuality concerns of boys with intellectual disabilities.
Similarly, studies should primarily focus on mothers than fathers. It’s also essential to study the different perspectives of healthcare experts, social workers, and special educators on the emerging sexuality of adolescents with IDD. Lastly, longitudinal research may give a more comprehensive approach and better picture of sexuality and sexual health over time.
Conclusion
This study highlighted the primary caregiver’s experience of the sexuality of their children with ID. Supporting adolescents with IDD in terms of sexuality is a complicated task that requires the vigilant address of experience of anxiety, dilemma, and practical questions. Contextual factors like support, attitudes, and perceptions of primary caregivers and society often control opportunities for persons with IDD to experience and express their sexuality. Prejudicial social attitudes regarding the sexuality of individuals with IDD create discriminatory practices. Shifting from deficit-based practices to a potential or strength-focused approach is essential.
Limitations of the Study
A limitation of this meta-synthesis is the inherent subjectivity in interpreting primary carers’ experiences regarding the emerging sexuality of adolescents with IDD. Since qualitative data from various studies are integrated, the interpretation of these experiences may vary among researchers, potentially influencing the understanding of how primary carers navigate and perceive the sexuality of adolescents with disabilities.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We would like to thank all the authors of the studies included in this meta-synthesis for their valuable contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and informed Consent
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.