
Abstract
Sex is a biological need of human beings and the aspects of sexuality and sexual development are less discussed in people with intellectual disability (ID). Sex education training (SET) for persons with ID and their parents is pivotal in mitigating challenges and creating a safe and healthy space for expressing their sexual needs.
The aim was (a) to see the effects of SET in the enhancement of knowledge and skills about sexual health among adults with ID, (b) To see the effect of mothers as an observer during SET on their perception, attitude and practice on sexual health for their children with ID. The sample consisted of 11 mothers and their children who were above 18 years with ID. Awareness of sexual health education for parents of intellectually challenged children and family life and sexual health assessment tools were used. A qualitative/descriptive analysis was done. SET was started for the period of three months, two sessions in a week, each session lasting one and half hours. It was done in a playful manner on self and social awareness, safe/unsafe touch, relationships, personal safety rules and sexual harassment of women at workplace (POSH).
SET shows not only enhancement in the level of awareness, knowledge on sexual health but also improved communication skills and decision-making skills among adults with ID and their mothers. Mothers feel more confident and comfortable to have open discussions with their children on sexual health.
Introduction
Intellectual disability (ID) is characterized by a significant global delay in achieving milestones, associated with an arrest or slow rate of development compared to normal children. It leads to deficits in intellectual functioning and adaptive abilities. It is present since birth or early childhood and definitely manifests before the age of 18. 1 Its prevalence in India is approximately 1%–3.2% of the population. 2
The sexual development of a person is a natural process in the overall development. Sexuality is a fundamental need of the human being. It is an integral part of the personality of everyone: man, woman and child. It cannot be separated from other aspects of life. 3 Sexuality is a diverse and complex subject which needs to be understood through the lens of biopsychosocial development. It encompasses one’s actions/behaviors, thoughts, feelings and functioning as male and female.
Sex and sexual health are sensitive topics. Talking about sex is taboo in society and there is a lot of misunderstanding about sexuality. Moreover, knowledge and awareness among people are very limited.
Individuals with ID also undergo the same developmental stages and changes, that is, physical, emotional, and sexual. They experience puberty the same hormonal changes as their healthy peers. However, they are regarded as asexual, childish or inhuman. 4 It is believed that they are over-fond of sex, they could not control their sexuality 5 and unwanted sexualized behaviors may occur among these people as they do not know whether their sexually oriented behaviors are appropriate in terms of place, time and context.6,7 They have the same sexual needs and desires as healthy ones but the way of discovering and expressing sexual feelings might be different.
In addition, parents of individuals with special needs face numerous challenges on a day-to-day basis and they do not have either time or strength to initiate conversation on sexuality. They both are confused and find it difficult to have an open discussion with each other. They either hesitate or feel ashamed to talk. Parents generally forget that they are the primary sex educators to their children irrespective of their disabilities. Parents are fearful that giving this information will arouse their curiosity and lead to experimentation or they will not understand these sensitive issues because of an immature mind. The majority of parents do not know how to deal with such problems, and they have anxiety about how to educate their children on sexuality and sexual development.8-12 Therefore, parent education programs are needed to promote confidence and enhance knowledge on their roles in sexual health education of persons with special needs. Father can educate his daughter and a mother can educate her son. However, gender has no role in imparting sex education to their children with ID13,14; rather parents should feel free to share and listen to their children’s viewpoint in a non-judgmental way and must avoid unrealistic statements. These comments lead to poor self-esteem, low confidence and motivation to learn them and their views on sexuality depend on social acceptance, attitudes and opinions of family members.15,16
Families usually recognize that children with ID have the right to express the aspects of sexuality but in practice, parents’ over-protection of their children from social contact and access to sexual knowledge directly affects their sexual attitudes and behavior. They do not have access to adequate information about sexual behavior, which makes them vulnerable to sexual abuse.17,18 Therefore, parent education on sexuality is an important aspect in creating awareness in families and society. Families must acquire necessary skills so that sexual abuse can be prevented and improve sexual well-being in persons with special needs.19,20 The role of mothers in imparting sex education to their children is more significant than the fathers of children with ID. As mothers are more careful about contraception, readiness to learn about sex and decisions about intimate relationships.21,22
Furthermore, a systematic literature review on mothers’ perceptions of sex education for children with ID. 23 The findings showed that mothers want to provide appropriate sex education for their children, believing that school could be the best choice for providing sex education, and mothers have barriers to providing sexual education because of lack of confidence, resources and support, and poor knowledge about sexuality. Hence, the role and responsibility of the mothers as facilitators in providing sex education in the family is very crucial. Mothers’ concerns, challenges, perceptions and attitudes on sexual health must be addressed. As mothers are the primary teachers of their children, making them aware and educate would play a significant role in enhancing sexual health and well-being, reducing the vulnerability of sexual abuse and harassment of persons with ID. Moreover, it would be cost-effective and less of a financial burden on the families. There is a dearth of adequate and effective teaching materials on sex education for persons with ID and capacity-building training programs for mothers. Hence, the present study has been taken up for enhancing knowledge, awareness, adequate perception and skills on sexual health in persons with ID and their mothers.
Objectives
To see the effects of sex education training (SET) on enhancing knowledge and skills on sexual health among adults with ID.
To see the effect of mothers as an observer during SET on their perception, attitude and practice about sexual health for their children with ID.
Method and Materials
Sample
The study was carried out on 11 mothers and their children with mild to moderate levels of ID, above 18 years, who were attending employability training at the Center for the Differently Abled, Bangalore City, India. The mothers were confused, anxious, fearful about their children’s sexual health and well-being and facing challenges related to sexuality. Informed written consent was taken from the mothers and their children. The adults with ID had comorbidity of Down syndrome, learning difficulties, speech difficulties and an autism spectrum disorder.
Exclusion Criteria
Both mothers and their children who were having comorbidity of mental illness and mood disorder were excluded from the study.
All relevant ethical approvals regarding conducting the study were obtained from ethical committee.
Tools Used
Family Life and Sexual Health (FLASH) assessment 24 was used and customized as per the needs of the adults with ID. It has 42 items, focusing on private/non-private body parts, places and behavior, puberty, relationships, social-sexual boundaries, exploitation, gender identification, self-esteem, and communication in Part A and Part B has designed separately to assess the knowledge on sexual harassment of women at workplace and legal aspects (POSH ACT) as these trainees were getting training for open employment. The respondent was asked to tick mark/write in the box opposite the item statement of which he/she thinks suitable or correct answer. Qualitative and descriptive scoring methods were used. Two scores for appropriate answer/response, 1 score for right responses with cue or pointing and 0 score for wrong or no answer were given. Later, sum of the total scores was done which serves as a raw score and baseline for the SET. Later the percentage was calculated for interpretation of the scores. The minimum and maximum possible scores were 0–80 in Part A and 0–6 in Part B.
Awareness on Sexual Health Education (ASHE) for parents of intellectually challenged children. 25 It consists of 71 items referring to three dimensions, that is, knowledge, attitude and practice on sexual health and responses were given as “Strongly Agree, Agree, Uncertain, Disagree, and Strongly Disagree” with a five-point rating. The scoring was done as per the procedure mentioned in the manual. Results were interpreted based on percentage.
Design
Pretest-posttest assessment design was used.
Techniques Used
Psychoeducation, role play and group discussion, non-judgmental approach, open space to express feelings and thoughts, playful manner during SET.
Parents as an active observer throughout the SET.
Procedure
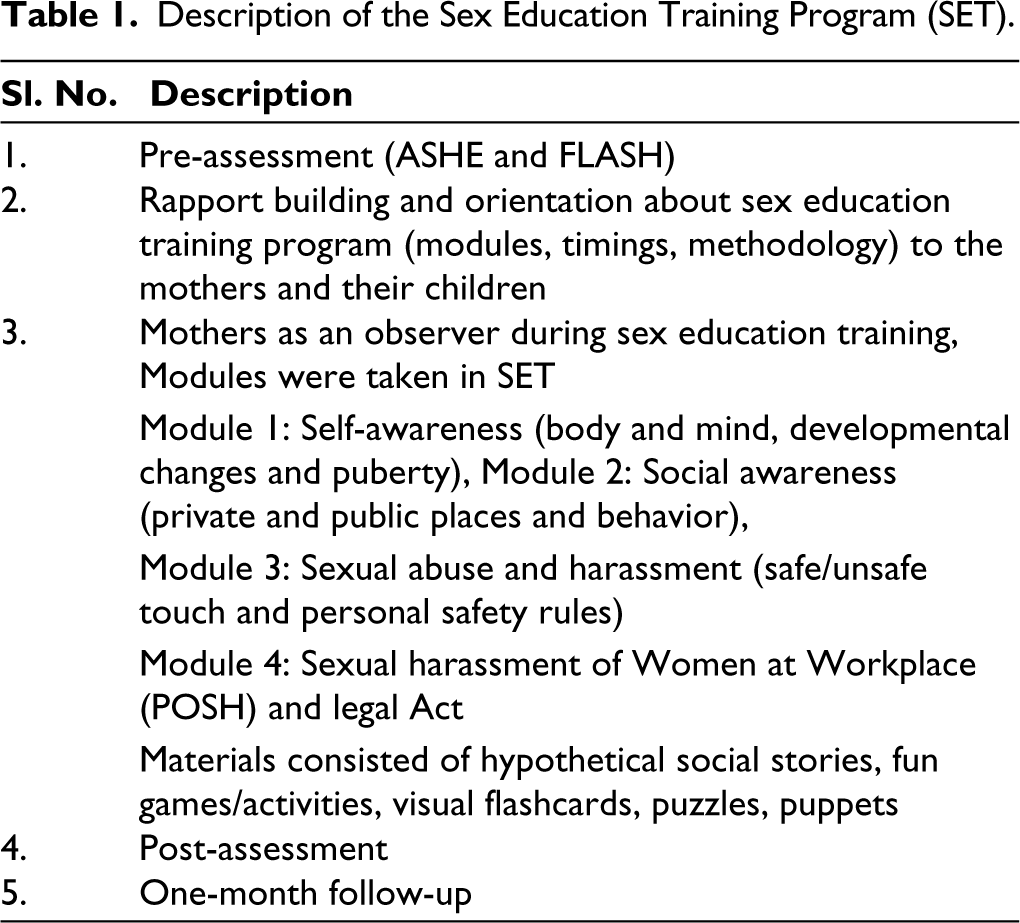
The assessment of ASHE and FLASH were done. Later, SET was started for the period of three months, two sessions in a week, each session lasting one and a half hours. These training sessions were conducted in small groups of five to six trainees (male and female together) in two batches and mothers were active observers throughout the sessions. The training program was conducted by the rehabilitation psychologist (registered with the Rehabilitation Council of India) who served as Facilitator. The description of the training modules and materials is given in Table 1.
Description of the Sex Education Training Program (SET).
Analysis
Descriptive and qualitative analysis were done.
Results and Discussion
The results are presented in Tables 2, 3, 4, and 5.
Results of Pre- and Post-assessment of FLASH.
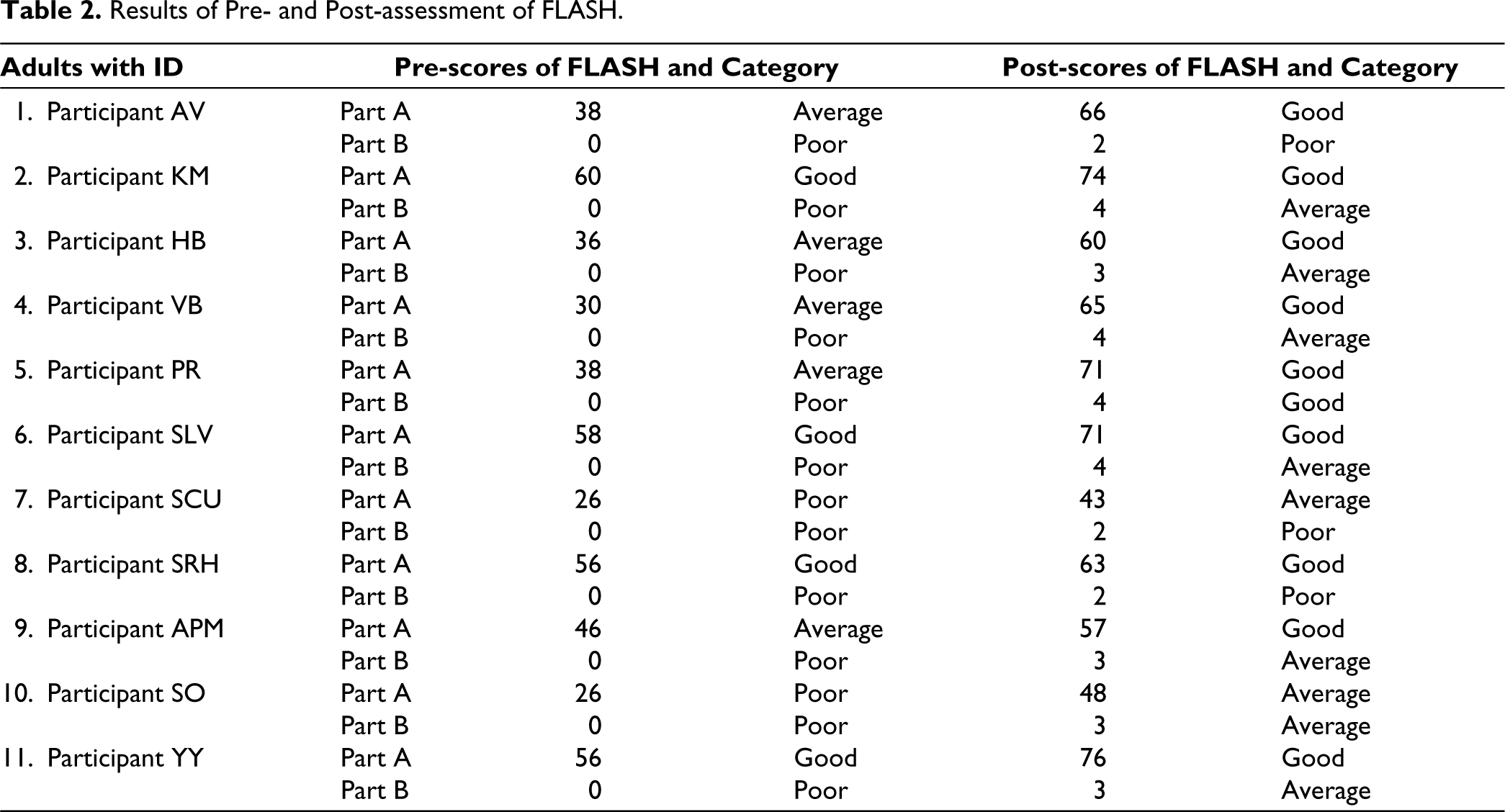
The results of Tables 2 and 3 showed drastic improvements in the knowledge of sexual health through SET among the adults with ID, that is, understanding public and private places and behavior, private body parts, safe/unsafe touch, puberty, developmental changes, gender identification, personal safety rules, sexual harassment of women at workplace and legal aspects. Area-wise qualitative analysis of Part B on FLASH revealed that these trainees were lacking knowledge of sexual abuse and harassment of women at workplace. SET enhanced not only the knowledge of POSH but also improved their behavioral skills, communication skills and decision-making skills.
Results on Qualitative Analysis of FLASH.
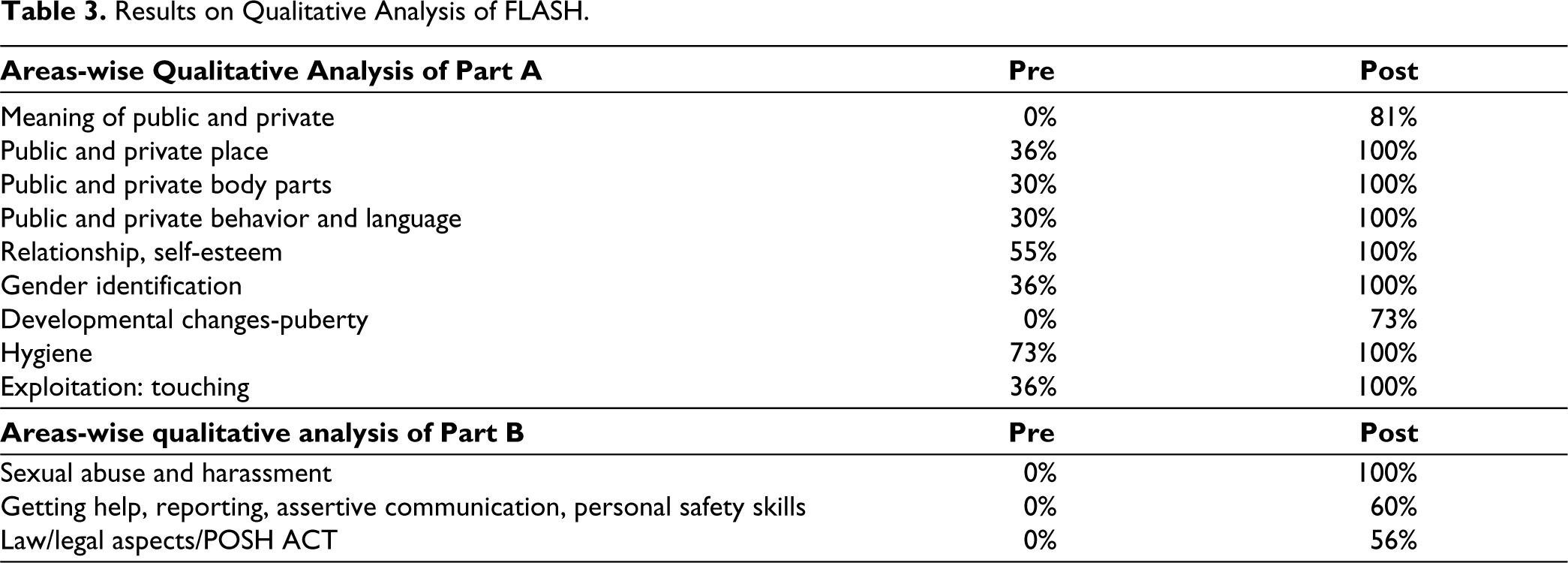
All participants shared that they like role plays on the various situation related to sexual harassment at workplace and POSH ACT because corrective feedback helped them to learn the skills in a better way.
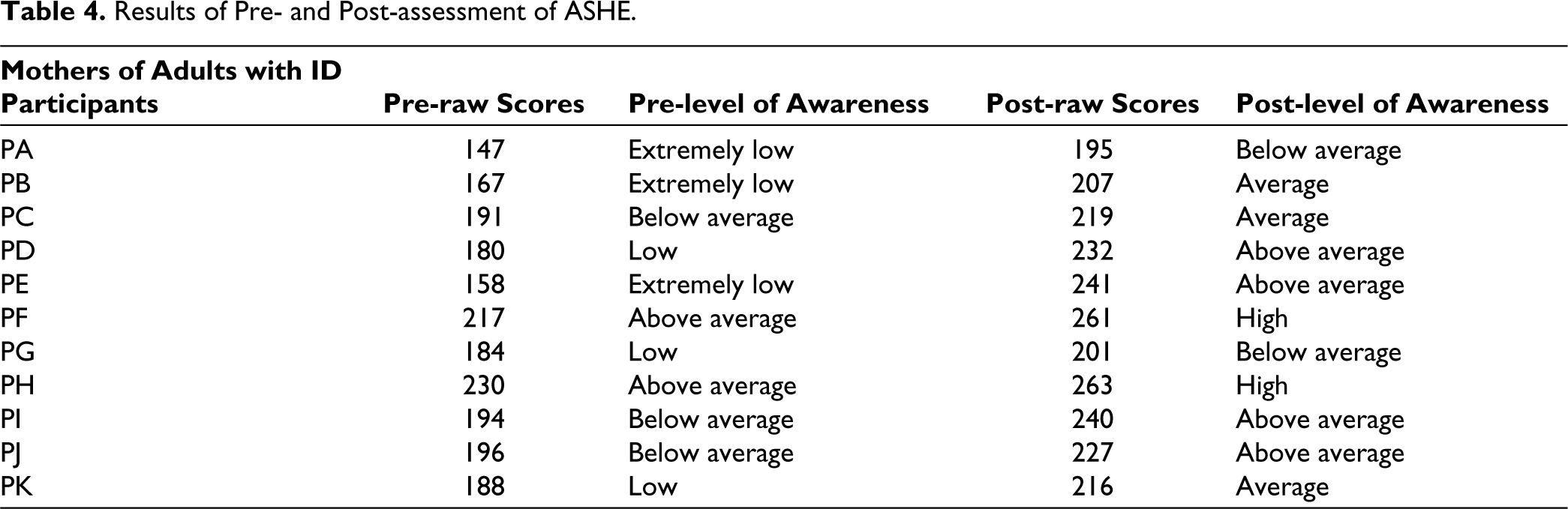
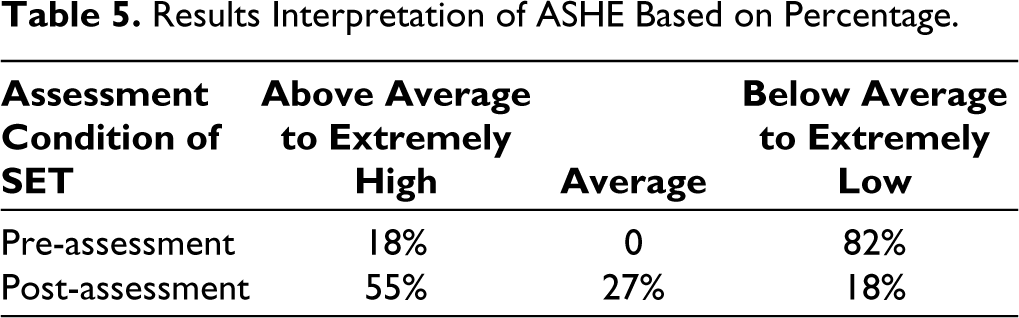
Tables 4 and 5 show results of pre- and post-assessment of ASHE indicating drastic changes in the perception, awareness, attitude, skills and knowledge of the mothers on sexual health and sex education. The present study found that mothers as an active observer are a very prominent factor in supporting adults with ID in understanding and experiencing sexuality and sex education. Moreover, their fears and worries about children’s sexual well-being have reduced. Fifty-five percent mothers enhanced their level of awareness (above average to extremely high levels of awareness) from the 18% mothers on pre-assessment, 27% mothers enhanced their level of awareness (average level of awareness). Eighty-two percent mothers who were having awareness below average to extremely low levels of awareness in pre-assessment, which was very high, came down to 18%. Mothers found themselves more aware, knowledgeable on the topic of sexual health education, physiological growth and development, sexual abuse, sexual feelings, sexual attitudes, sexual abuse, sex education as misleading topic, social behaviors and interaction, right to sexual health education, relationship, personal hygiene, difference between safe/unsafe touch, personal safety skills, sexual harassment of women at workplace (POSH ACT).
Results of Pre- and Post-assessment of ASHE.
Results Interpretation of ASHE Based on Percentage.
Now mothers find themselves more confident in handling sexual health education as they are equipped with teaching methodology (what to teach, when to teach and how to teach), with scientific information to their children with ID. Social Stories are effective strategy to teach appropriate social behaviour for woman with ID under sexual education program.26,27 It helps to encourage parents to support their sons or daughters in expressing sexuality safely in any way they choose. 28 Awareness of mothers has a major role in providing sex education to their children and this kind of extensive parents’ empowerment programs are needed.29,30 Parents’ active involvement must be ensured for its effective implementation 31 and their views on sex education are important predictors of parents’ implementation of SET. When their attitude toward sex education and sexual behavior is positive, they can talk more about sexual issues with their children 32 which would help them in enhancing sexual well-being.
In addition, the capacity of parents and children to perceive risk, lack of accurate sexual knowledge, personal beliefs and social and cultural values as important factors that influence communication between parents and their children for sexual issues, 33 school can provide more comprehensive information and avoid the embarrassment of mothers communicating with their children about sexual issues. 34
As SET consisted of role plays, flash cards, stories, puzzles and games in a fun way which made it unique and successful too. It helped in building capacity/skills of adults with ID and their mothers on sexual health and well-being. Moreover, it was a vehicle to bring positive changes in a mother’s knowledge, perception and attitude toward imparting sexual health education. It is very important for individuals with ID to have age-appropriate and comprehensive sexual health education. So that they can be equipped with facts on sexuality, able to manage and enjoy relationships, discriminate between safe and unsafe touch in any situation at home, social and workplace, able to report incidents of suspected sexual abuse and take the right steps in order to deal with these issues.
Feedback Shared by Mothers
“Earlier I had the impression of sex education is bad but now this thought has fully changed. I was worried and afraid. Now I am very much satisfied. I learnt a lot. Role play method was useful.”
“As a mother I learnt how to behave with him, I understood that they are not children, they are adults. Now he understands the concept of private and public, he is able to manage erections in his private body part. Earlier it was a big challenge for me. We have seen that other people take advantage of him, Sex education training is very useful to learn these concepts and prevent sexual abuse. I also learnt the method of teaching on these sensitive issues.”
“It is a much-needed program.”
“She used to share every detail of her personal life with anyone she meets, even strangers. Now, she understands and her habit is reduced.”
Conclusion
It is concluded that SET as capacity building tool for mothers and their children with ID is effective in enhancing awareness, knowledge, skills, practice on sexual health and reducing worries and anxiety in mothers about sexual abuse and harassment.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Formal approval from Ethical Committee has been obtained for the study.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written consent was taken from the mothers and their children.