
Abstract
Introduction:
Sexual and reproductive health (SRH) education is crucial to prevent unwanted pregnancies and sexually transmitted infections (STIs) among young people. However, in Sri Lanka, little is known about the level of access to SRH education and knowledge among unmarried youth. This study aimed to assess perceptions of SRH education at school and the level of knowledge on selected aspects of SRH among unmarried youth aged 15–24 years in Sri Lanka.
Methods:
A cross-sectional study was conducted among 1057 unmarried male and female youth aged 15–24 years in three selected districts of Sri Lanka. A semi-structured, self-administered questionnaire was operationalized after receiving informed consent. Twelve focus group discussions were also conducted with the youth.
Results:
A sizable proportion of youth demonstrated low access to SRH education and a low level of knowledge on pregnancy, contraception, and STIs. Although it is limited, respondents felt that the SRH education received in school is useful for their life. Friends and the Internet were identified as the primary sources of information among boys, whereas the mother was the primary source for the majority of girls. Boys demonstrated better SRH knowledge compared to girls for most of the aspects. SRH knowledge was increased among both boys and girls significantly with maturity.
Conclusion:
Results conclude that there is a significant knowledge gap on SRH among unmarried youth. Introduction of age-specific and gender-sensitive SRH education is important to address the current gap in SRH knowledge.
Keywords
Introduction
In Sri Lanka, although significant progress has been made in the health and education domains, there is still a concerning lack of knowledge among young people when it comes to sexual and reproductive health (SRH) issues 1 . This knowledge gap can be attributed to the societal norms and values influenced by various religious and cultural traditions, which discourage open dialogue and discussion on matters related to sex. As a result, young people in Sri Lanka have limited access to information and awareness on SRH, which has been identified as a key concern 2 . In the meantime, attempts at the school level, to generate interest in open discussions on human SRH issues among adolescents and youth, have achieved only limited success3,4.
Over the past decade or so, Sri Lankan youth have experienced significant changes in their social and economic environments, as well as advancements in technology and communication due to globalization. As a result, they have been able to access a broader range of information on sex and reproduction than before 5 . This transformation has been noted by De Silva, 15 who highlights the impact of these changes in facilitating access to information on SRH for Sri Lankan youth. The print and electronic media in Sri Lanka offer varying degrees of knowledge on SRH 6 . However, the commercialization of such information has often taken advantage of the vulnerability of youth, focusing more on sexual content rather than scientific and health-related aspects. Consequently, this approach has led to the misinterpretation of SRH issues among Sri Lankan youth, resulting in a lack of accurate knowledge on the subject7,8.
In the early 1990s, the Sri Lankan government took a progressive step by introducing SRH education in state schools. To achieve this, the National Institute of Education launched a population and family life education project, with funding from the United Nations Population Fund 9 . The project aimed to incorporate various reproductive health components into the school curriculum at different grade levels 4 . Following the International Conference on Population and Development in 1994, the Sri Lankan government expanded the reproductive health sections included in the school curriculum. This move was in line with the recommendations made at the conference and aimed to promote better SRH knowledge among young people 9 .
Currently, the Sri Lankan school curriculum includes “Sexual and Reproductive Health Education” in two primary subjects––the Science stream and the Health and Physical Education stream. These study areas aim to provide a comprehensive understanding of SRH. However, due to religious and cultural sensitivities, family planning is not included in the curriculum. Despite this, the effectiveness of teaching SRH in schools remains a major concern, as the actual extent of teaching and learning of SRH within the school system is not well established 3 .
The Ministry of Education’s recent structural changes to the General Certificate Examination—Ordinary Level (GCE O/L) examination process have had a significant impact on sexual and reproductive health (SRH) education in Sri Lankan schools. Presently, only six subjects, referred to as “Core subjects,” are considered prerequisites for entry into GCE (A/L). Science is included in this list, but Physical Education, which encompasses a major proportion of SRH, is not. While Physical Education is a compulsory subject, students tend to pay less attention to it because obtaining a pass is not required to pass the Ordinary Level or fulfill entry criteria for the Advanced Level. Moreover, the importance given by teachers to deliver SRH components in Physical Education is low due to the same factor 3 . Additionally, Sri Lanka has yet to implement comprehensive sexual education (CSE). Nepal is currently the only South Asian country where CSE has been formally introduced into the school curriculum and teacher training 3 . In Sri Lanka, studies have shown that young people primarily receive SRH information from sources that are not well-informed 1 .
Given this background, previous studies have indicated that Sri Lankan youth typically acquire SRH knowledge through life experiences such as pregnancy after marriage, rather than through formal education6,10. While previous studies have examined the SRH knowledge of youth and young people in general, there is limited scientific evidence available on unmarried Sri Lankan youth. Thus, it is crucial to investigate the SRH knowledge of unmarried Sri Lankan youth as they are more susceptible to engaging in sexual risk behaviors. The purpose of this study is to assess the SRH knowledge of young people in three selected districts of Sri Lanka.
Materials and Methods
To ensure a comprehensive understanding of the SRH knowledge among youth in contemporary Sri Lanka, a three- layered data collection approach was adopted. The first layer involved a review of existing literature on the SRH knowledge of unmarried youth in Sri Lanka. The second layer was designed to collect qualitative data through focus group discussions (FGDs), case studies with unmarried youth, and key informant interviews with health professionals, NGO workers, and government officials involved in youth service provision in the Hambantota, Nuwara-Eliya, and Puttalam districts. These districts were chosen to ensure a diverse representation of socio-cultural and geographical factors in Sri Lanka. The third layer involved a field survey to collect quantitative data on the SRH knowledge of unmarried youth in the selected districts.
The Second Layer: Case Studies and Focus Group Discussions
Young people who are not married and are between the ages of 15 and 24 were chosen as study participants for case studies and FGDs. To gather enough information from both younger and older youth, purposive sampling technique was used for FGDs to account for younger (15–19) and older (29–24) youth; inclusion of three selected districts; selection of both male and female youth. The research team held four FGDs in each of the three Sri Lankan districts of Puttalam, Nuwara-Eliya, and Hambantota. The team realized that because the topics were so delicate, people were more at ease sharing their opinions honestly if they felt like other group members were going through similar things. Participants were divided into two segments: males and females. So, there were two FGDs with young, single men and two with women. counterparts were conducted with male and female FGDs further divided into younger youth and older youth separately.
Fifteen case studies involving young people who are not married were conducted by the research team. Unmarried youth were also recruited from a variety of backgrounds, including those without a high school diploma, those in technical and higher education, as well as those who were employed and unemployed, to improve representation and capture a wider range of practices. Hambantota, Nuwara-Eliya, and Puttalam districts all hosted interviews. Unmarried young people with the aforementioned traits participated in five case studies each per district. The assistance of many Non-Governmental Organizations, universities, and other educational institutions in the region was used to identify the eligible youth of the chosen districts. The selected respondents were requested to attend the specific center for FGDs/ case studies. The NGOs that were chosen had experience in the health field and worked with the data collection exercise. In addition to them, a few vocational, technical, and educational centers in the predetermined districts assisted with data collection.
A total of eight key informant interviews were conducted with executives from the public and private sectors who were either involved in or interested in youth-related activities. These interviews were designed to gather information to evaluate the status of romantic relationships, dating, and sexual behavior among Sri Lankan unmarried youth because the key informants were experts on the topic.
The Third Layer: Sample Survey
An observational descriptive cross-sectional sample survey was carried out in Sri Lanka within three districts from the 1st of March 2019 to the 31st of January 2020. A complex mix sampling method was adopted due to possible bottlenecks that could limit any single sampling technique from capturing a representative sample. These bottlenecks include the stigma associated with the study question and difficulty in approaching the target population. Urban (Puttalam), rural (Hambantota), and estate (Nuwara-Eliya) were selected as the three study districts conveniently. To select a representative sample, the research team used both probability and non-probability sampling techniques.
Sampling Technique
Among the selected three districts, only unmarried youth representing the selected sector were recruited from each district (I.e. Rural sector youth Hambantota, urban youth-Puttalam, estate youth Nuwara-Eliya). Mix sampling techniques (Stratified cluster sampling and snowball sampling) were used together to capture the study population––the youth outside their place of residence due to the culture-sensitiveness of the study questions. 19 The youth were recruited from educational institutes such as vocational centers and private educational institutes by stratified cluster sampling whereas support of NGOs was sought to recruit out-of-school youth who are not seeking either higher education or vocational training by snowball techniques. A sample of 1100 never-married youth of age 15–24 years was targeted using a self-administered questionnaire with 780 (260 per district with a cluster size of 20) to be selected by stratified cluster sampling and 320 youth through snowball technique; Hambantotaa-64, Nuwara-Eliya-101, and Puttalam-155).
Data Collection and Analysis
The young persons were requested to fill out the questionnaire individually in a common place after an informal introductory session on the study and the data collection tools. The total number of youth who responded was 1057 with 305 from the rural sector, 345 from the estate sector, and 407 from the urban sector. We used SPSS version 22 for analysis. The results were presented as proportions. Ethical clearance was obtained from the Ethical Review Committee of ChildFund International.
Results
The sample showed roughly equal age-wise representation, with a slightly higher proportion of females (55.3%) compared to males (44.7%). The majority of the youth (91.2%) reported living with their parents, which is in line with the socio-cultural norms of Sri Lanka. A significant number of the respondents (58.8%) belonged to the Sinhala ethnicity, which is the major ethnic group in the country. Regarding employment, only 10% of the youth reported being employed, while close to 20% were actively seeking employment.
SRH Education at Schools
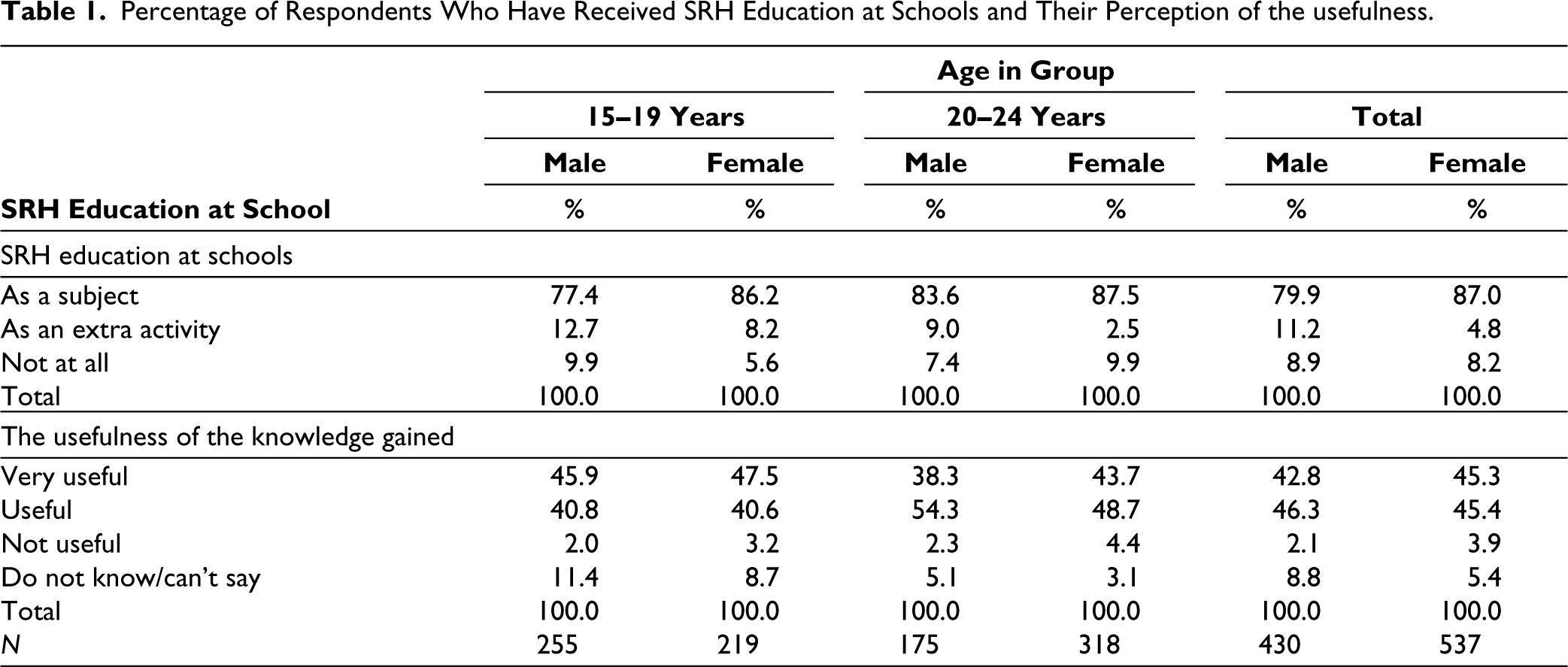
Approximately 84% of the respondents had received information about reproductive health as a part of their school curriculum, while an additional 8% had received SRH education as an extra activity at school. However, 9% of the respondents had not received any SRH education from their schools. The percentage of respondents in the 15–19 age group who received SRH education as a subject at school varied between males (77%) and females (86%) (Table 1).
Although a significant proportion of respondents reported receiving SRH education as a subject at school, the adequacy of the actual content delivered is a major concern. Several youths in both Hambantota and Nuwara-Eliya districts expressed dissatisfaction with the quality of the SRH education provided, stating that the subject was often skipped or not adequately covered by their teachers. For example, a 17-year-old male youth from Hambantota district stated, “I don’t know much about reproductive health… As it was not taught by the teacher and was skipped.” Similar views were expressed by several youths in Nuwara-Eliya district, who felt that female teachers were often shy or uncomfortable teaching the subject, and would often skip over it entirely. These concerns were echoed by the majority of youth who participated in FGDs and case studies across all three surveyed districts, highlighting the urgent need for improving the quality and adequacy of SRH education in state schools.
Despite the importance of SRH education, there are significant challenges in delivering this education to school children. In addition to the concerns about the quality of education mentioned above, there are also concerns about the lack of opportunities to provide SRH education due to poor cooperation from school administrative staff. According to a Medical Officer of Health in the Puttalam district, school principals often do not provide adequate time slots for conducting SRH education in schools, particularly in schools headed by clergy. This lack of cooperation from school administrators is hindering efforts to provide students with the necessary SRH education. Although there are concerns about the actual proportion of SRH education delivered in schools, the limited amount of SRH education provided was considered useful by the respondents. Approximately 90% of the youth, regardless of their gender, found the SRH knowledge imparted at school to be useful or very useful (Table 1).
Percentage of Respondents Who Have Received SRH Education at Schools and Their Perception of the usefulness.
Other Sources of Knowledge
The sources of SRH information among youth were investigated and revealed that a significant percentage of male youth in the 15–24 age group, approximately 42%, obtained information from their friends (Table 2). On the other hand, for females, their mothers were the most common source of SRH information, with nearly half (47%) of the female youth aged 15–24 reporting their mothers as the primary source. In contrast, only 10% of male youth reported their fathers as a source of SRH information. These findings suggest a gender difference in the primary sources of SRH information for youth, with friends being more significant for males and mothers being more prominent for females.
Sources of SRH Knowledge by Age and Gender.
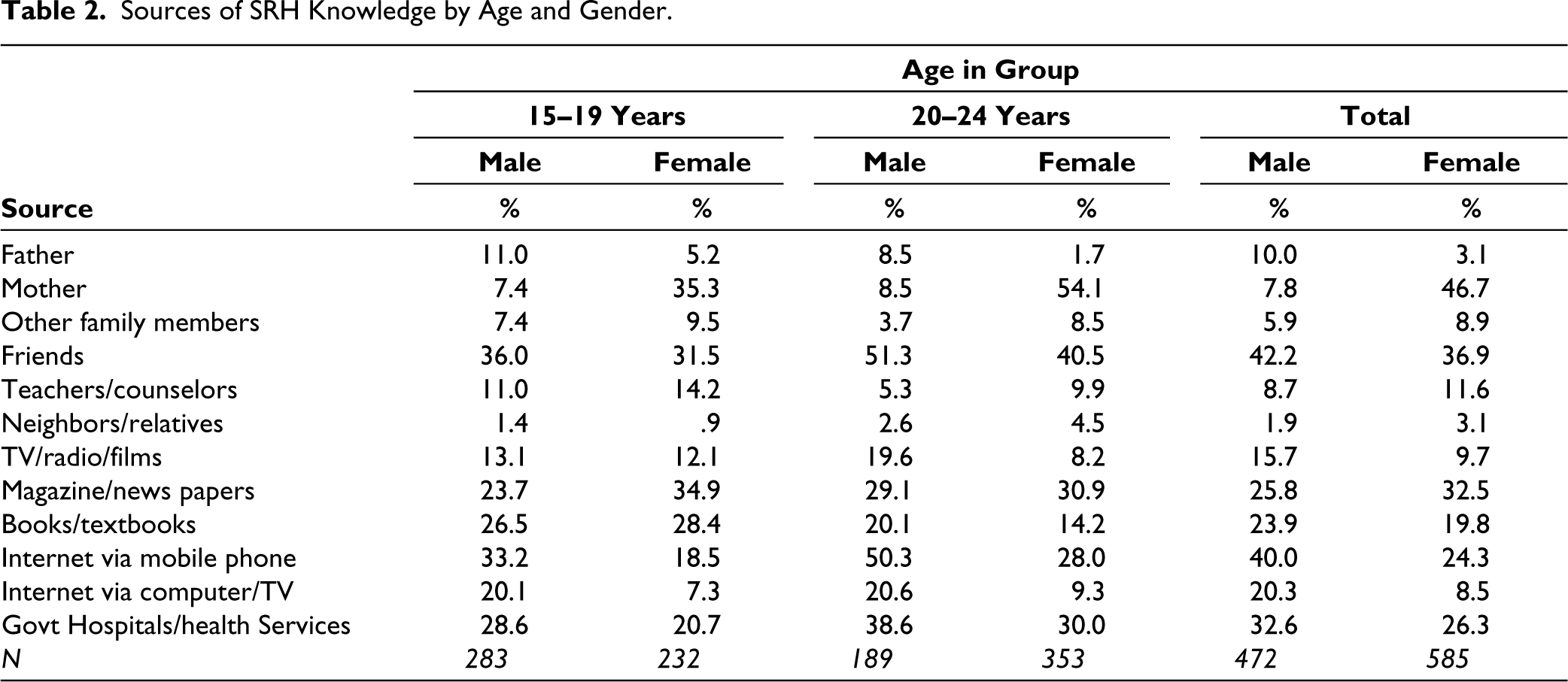
According to the survey, 40% of male youth reported that the Internet via mobile phone was one of the most popular sources of SRH information, second only to friends (Table 2). An additional 20% of male youth reported using the Internet via computer/TV (including tablets, etc.) as a source of SRH information. Therefore, as many as 46% of male youth rely on the Internet for SRH information. It is noteworthy that the Internet is the most significant source for searching SRH information among youth in Sri Lanka, indicating that the communication revolution and globalization have had a substantial impact on the dissemination of SRH information. Further analysis of sources of SRH information revealed that 24% of female youth received information about SRH from the Internet via mobile phones, while an additional 8% received it from computers/TVs. collectively, 28% of female youth used the Internet for SRH information. However, the Internet was the 4th most profound source of information for females, with their mother being the most common source, followed by friends. This is in contrast to males, for whom the Internet was the second most popular source after friends.
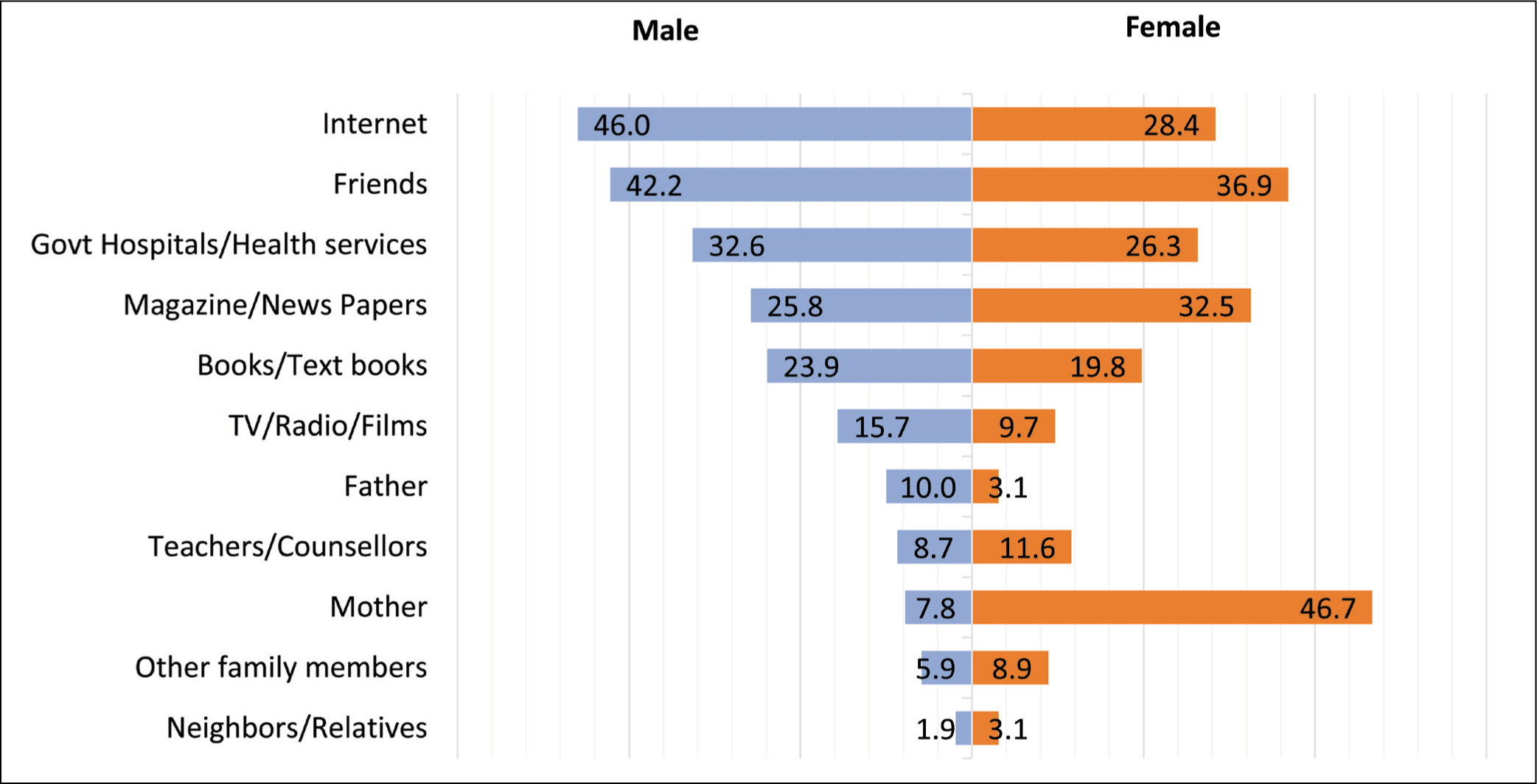
The Internet emerged as the most popular source of SRH information among males, with 40% and 55% of respondents in the 15–19 and 20–24 age groups respectively, reporting it as a source (Table 2). However, a significant proportion of males still relied on friends and government hospitals/health services for SRH information. The use of mother, father, and teacher/counselor as sources of SRH information was very minor among males. For both age groups of female youth, the most commonly used source of SRH information was their mother, with approximately 47% and 57% of respondents in the 15–19 and 20–24 age groups respectively, reporting it as a source. Among females aged 20–24, friends and the Internet were the second and third most popular sources respectively, while among younger females, friends and the Internet ranked at the second and third positions. The Internet was the fifth most popular source of SRH information among younger females but ranked at the third position among more mature female youth. It is noteworthy that although modern technology, including the Internet, has penetrated many parts of the country, still a sizable proportion of youth in both age groups preferred to use print media such as magazines and newspapers for the same purpose (Figure 1).
Source of SRH Information by Sex
Knowledge on Procreation
Nearly half of the surveyed youth, regardless of their gender, were aware of procreation. When examining the age-specific patterns, it was found that 44% of males and 42% of females in the 15–19 age group were familiar with the term. The highest percentages of awareness were observed in the 20–24 age group, with 51% of males and 54% of females indicating knowledge about procreation (Table 3). The analysis of youths’ knowledge of procreation showed no significant difference between genders, but an age-specific trend was observed, indicating an increase in knowledge with maturity. While only 43% of youths in the 15–19 age group had correct knowledge of procreation, over 53% of those in the 20–24 age group reported such knowledge. Interestingly, while females in the 15–19 age group were less knowledgeable about procreation compared to males, the opposite was observed in the 20–24 age group.
Knowledge of Reproductive Organs
The questionnaire administered to the participants included a diagram featuring four male reproductive organs and four female reproductive organs. Participants were asked to identify and name all eight reproductive organs correctly, and their ability to do so is presented in Table 3. The results show that only 30% of the youth aged 15–24 were able to correctly identify all eight male and female reproductive organs presented in the diagram. Out of the total 1,057 youth respondents, only 313 identified all organs correctly, with over 38% of male youth and 23% of female youth being able to do so. Interestingly, the proportion of youth who were able to identify all eight reproductive organs correctly increased significantly with age, from ages 15–19 to 20–24 years. While a similar percentage of males in both age categories were able to identify all organs, the difference was more pronounced among females, with only 12% of females aged 15–19 correctly identifying all organs compared to 29% of females aged 20–24.
Extent of Knowledge on Procreation and Reproductive Organs by Age and Sex.
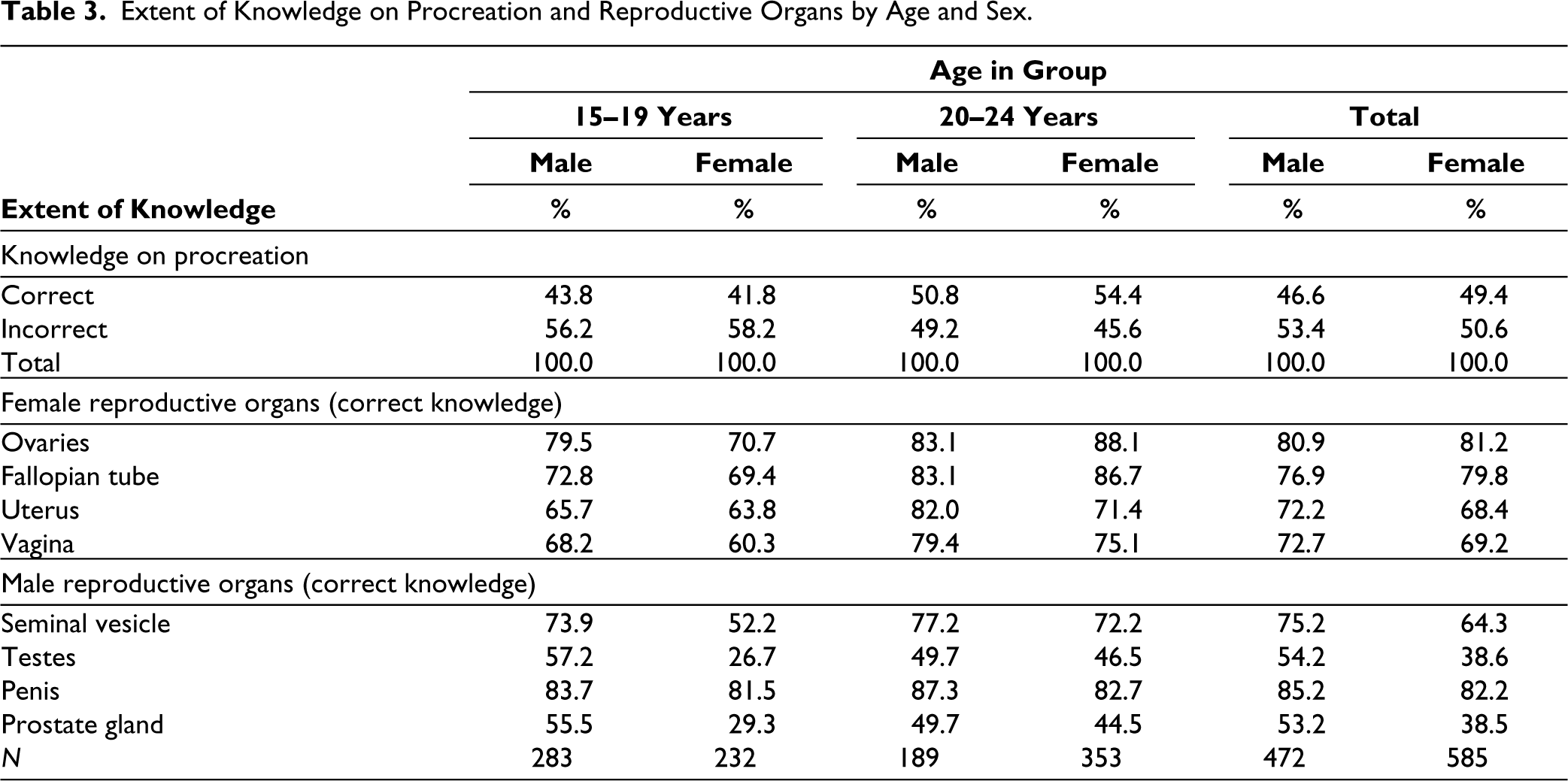
The analysis further revealed an age-specific trend, where the proportion of youth possessing knowledge increased with increasing age. The study also found that a majority of males in the 20–24 age group had better awareness of the female reproductive system than females in the 15–19 age group. Similarly, a higher percentage of males in each age group possessed knowledge of the female reproductive organs than females in the same age group. In general, more males than females in each age group were aware of the male reproductive system.
Upon analysing the responses of male and female youth separately (aged 15–24), it was found that males tend to have a better understanding of both male and female reproductive organs compared to their female counterparts, except for knowledge of ovaries and fallopian tubes. Males reported better knowledge not only about their reproductive system but also about female reproductive organs. Interestingly, both male and female youths possessed a relatively low level of knowledge on male reproductive organs, except in the case of the penis, in comparison with female reproductive organs. When analysed separately, the lowest level of knowledge was noted for the prostate gland, while the highest was noted for the penis (Table 3).
Knowledge of Pregnancy and Conception
The most common human sexual activity is the union of the male and female reproductive organs, and many youths believe that only sexual intercourse can lead to conception. However, youth need to be aware of the risks associated with sexual activity in other circumstances as well. To assess the level of knowledge among youth regarding these risks, participants were asked to respond to two statements with three possible answers: correct, incorrect, or don’t know. The correct responses to these statements were analysed and presented in Table 4.
Respondents’ Correct Knowledge of Specific Areas of SRH by Age and Sex.
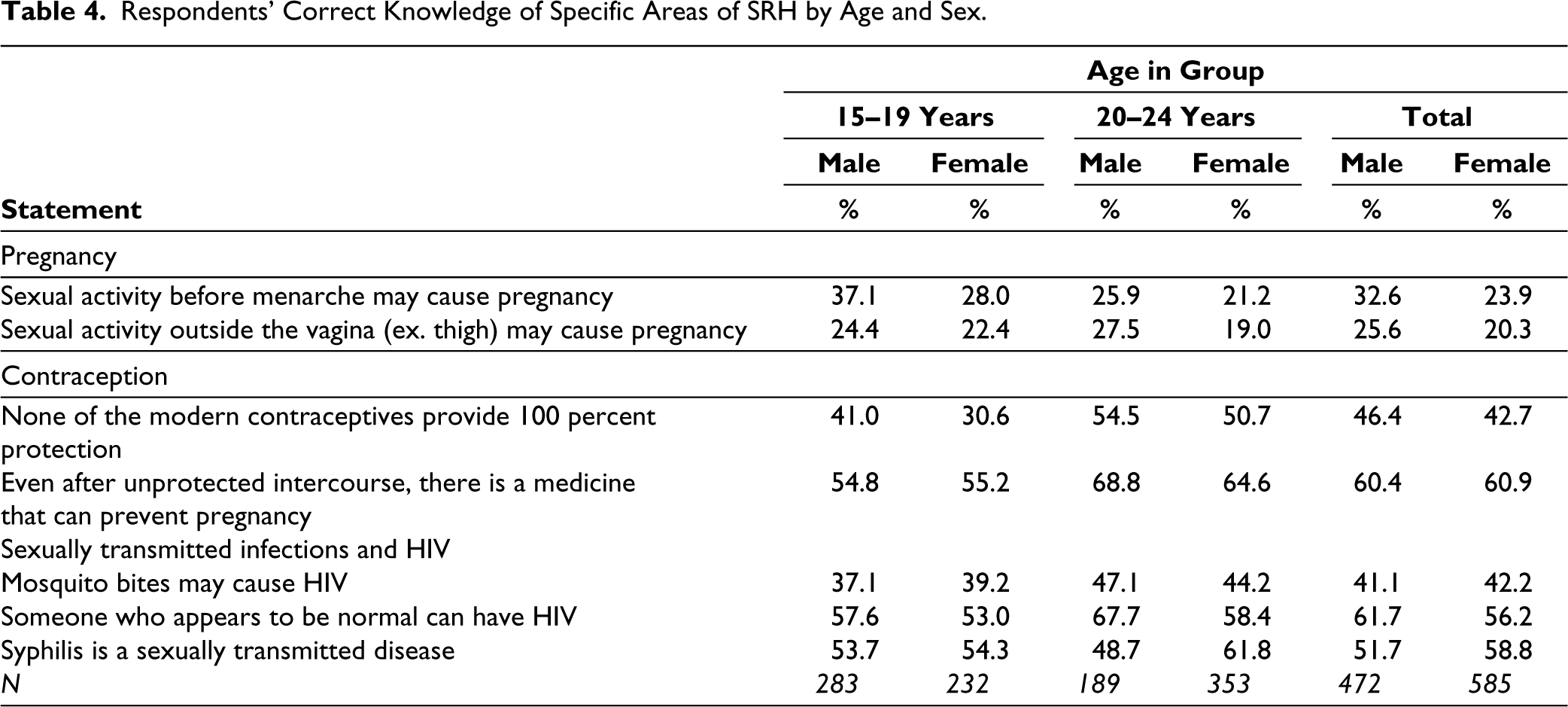
Out of the total male youth surveyed, 33% were aware that sexual activity before menarche may cause pregnancy. However, among female youth, only 24% gave the correct response, indicating a lower level of knowledge compared to their male counterparts. Notably, both males and females had a relatively low level of knowledge in this area, with females displaying significantly less knowledge than males. The analysis of correct responses by age and sex showed an intriguing finding––the younger age group had a better understanding compared to their older peers. This trend could be attributed to the recent expansion and improvement in the delivery of SRH education in schools, resulting in increased knowledge among the younger cohort. Additionally, males across both age groups had a significantly higher level of knowledge compared to females.
The results of further analysis of responses given to the statement regarding sex outside the vagina and the risk of pregnancy demonstrated a common pattern similar to earlier observations. Male youth had a higher level of correct knowledge compared to their female counterparts, with 26% of males possessing correct knowledge compared to 20% of females. However, in general, the level of correct knowledge reported in response to this statement was relatively lower than that of the first statement. Regarding the age-sex classification, young females again (22%) possessed higher knowledge than their older counterparts (19%). Conversely, the correct knowledge among younger males (24%) was lower than their older counterparts (27%). Presumably, older males who were sexually more active would have searched for information related to this area more frequently than their younger counterparts, perhaps using the Internet as a source of information 11 .
Knowledge on Contraception
The study found that an overwhelming majority (96%) were aware of contraception. The younger cohort (15–19 years) had a slightly lower level of awareness at 94%, compared to the more mature youth (20–24 years) at 98%. There was no significant difference in awareness between males and females in the total sample, with both groups reporting 96% awareness. However, a closer look at the age groups revealed some interesting patterns. Among females, awareness was 93% in the 15–19 age group and rose to 97% in the 20–24 age group. For males, awareness was already high at 94% in the 15–19 age group but reached 100% in the more mature group (20–24 years). Overall, the study suggests that the majority of youth in the sample had a good awareness of contraception, with higher levels of awareness among the more mature age group and males.
The study further investigated the respondents’ knowledge of specific areas of contraception. For the statement “None of the modern contraceptives provide 100 percent protection”, the percentage of males who knew this fact was higher than females in both age groups. Among the total youth, 46.4% of males and 42.7% of females had correct knowledge about this fact. The percentage of correct knowledge among the older age group (20–24 years) was higher compared to the younger age group (15–19 years) for both males and females. However, for the statement “Even after unprotected intercourse, there are medicines that can prevent pregnancy” which is on Emergency Contraception, the percentage of males and females who knew this fact was similar in both age groups. Among the total youth, 60.4% of males and 60.9% of females had correct knowledge about this fact. The percentage of correct knowledge among the older age group (20–24 years) was higher compared to the younger age group (15–19 years) for both males and females.
Knowledge of Sexually Transmitted Infections and HIV
Given that Sri Lanka is a low-prevalence country concerning HIV and is currently at the initial stage of the epidemic11,12,13, the knowledge, attitudes, and practices of the country’s youth must be assessed to successfully control the spread of the disease. With this context in mind, three statements were presented to the youth respondents to evaluate their knowledge in specific areas of STI/HIV (Table 4).
Approximately 60% of both male and female youth had the misconception that mosquito bites may cause HIV. After cross-classifying the correct answer by age and sex, a common pattern emerged––the older cohort had more knowledge compared to their younger counterparts. Presumably, the increased maturity of the older cohort is reflected in their better knowledge. The statement “Someone who appears to be normal can have HIV” also showed a similar pattern to the previous responses. While more male youth demonstrated correct knowledge than their female counterparts (62% vs. 56%), the overall level of correct knowledge reported for this statement was relatively higher than for the first statement. Nevertheless, 38% of males and 44% of females were still unable to understand the scientific reality behind this statement. Further analysis by age and sex revealed that older males and females had a higher level of knowledge than their younger counterparts. For example, the corresponding figure increased from 58% to 68% among males in the older age group. This may be because older youth who are more sexually active would have been exposed to more information about HIV from the Internet or other sources than their younger counterparts.
To assess knowledge on another specific area; Sexually Transmitted Infections (STIs), the respondents were asked to answer the statement “Syphilis is a sexually transmitted disease.” The results showed that a relatively higher percentage of both male and female youth groups had correct knowledge of this statement compared to the first statement, with 52% of males and 59% of females identifying syphilis as an STI. However, it is important to note that almost half of the youth still lacked knowledge in this area. Furthermore, when the responses were analysed by age and gender, it was found that although older females were significantly more knowledgeable about syphilis compared to older males, the difference in knowledge between younger males and females was marginal.
Discussion
Upon analysing the responses of male and female youth separately, it was observed that males tended to have better knowledge than females, not only about their reproductive organs but also about female reproductive organs, except knowledge regarding ovaries and fallopian tubes (Table 3). This could be partly attributed to the significant exposure that females received during mid-2019 from various media platforms regarding alleged forced female sterilization incidents, where discussions and graphical demonstrations were made on those two organs by experts 14 . Interestingly, except for those two organs, males were more knowledgeable about female organs than their reproductive organs.
As noted, both male and female youth respondents exhibited a lower level of knowledge regarding male reproductive organs, except the penis, in comparison to female reproductive organs (Table 3). Upon further analysis, it was found that the least knowledge was recorded for the prostate gland, whereas the highest knowledge was recorded for the penis. This disparity in knowledge could be attributed to several factors. For example, young males may have more opportunities to observe their genitals during bath time compared to females. Additionally, male genitalia is frequently depicted in various forms of art, while female reproductive organs are seldom portrayed 15 . It is essential to note that the causes for this difference in knowledge are likely multifaceted and complex.
As identified in the current study, there was a significant increase in the proportion of youth who were able to correctly identify all eight reproductive organs as they aged from 15–19 to 20–24 years. While the percentage of males who correctly identified all organs was similar across both age categories, there was a significant difference among females, with 12% of those aged 15–19 identifying all organs compared to 29% of those aged 20–24. This pattern could be related to the transition from adolescence to adulthood, as this is a period associated with unmistakable physiological changes, which are more vivid and obvious in the female body. Distinctive stages of development, such as puberty, the onset of menstruation, breast development, and changes in physique, are more apparent in females 8 . Moreover, the focus of attention and demand for factual knowledge on female reproductive organs from an early stage likely contributes to the fact that more male and female youth were knowledgeable about female reproductive organs.
It is well established that education is positively correlated with knowledge of SRH, including procreation15,16. The data from this study also supports this finding. More than half (54%) of youth respondents aged 15–24 who have completed GCE (A/L) or higher education reported having the correct knowledge of procreation, while only 42% of those with education below GCE (A/L) reported the same. Further analysis by age group reveals that youth with higher education status in both the 15–19 and 20–24 age groups were more likely to correctly identify procreation than their counterparts with lower education. Half of the youth aged 15–19 with GCE (A/L) and 55% of those aged 20–24 with the same education level reported correct knowledge on procreation. Overall, these findings support the positive relationship between longer exposure to education and better knowledge of procreation.
Findings emphasize the urgent need to prioritize and improve access to comprehensive and accurate SRH education for Sri Lankan youth, particularly the unmarried population. This could be achieved through innovative approaches, such as incorporating technology and peer education programs and involving both schools and community-based organizations in the provision of education. Addressing the knowledge gap in SRH education is crucial for empowering young people to make informed decisions about their sexual health and well-being, and ultimately promoting a healthier and more equitable society.
The results also suggest the importance of tailoring SRH education to different age groups. The older youth demonstrated greater knowledge of certain aspects of SRH, such as HIV transmission, indicating that maturity and exposure to sexual experiences may contribute to increased understanding. In addition, gender differences were observed in certain areas of knowledge, highlighting the need for education that takes into account the specific needs and experiences of both male and female youth.
Findings related to SRH education and knowledge on selected aspects of SRH reported in the above sections are based on the data collected in the year 2018. Although study findings indicate the importance of comprehensive SRH education at schools, due to COVID-19, economic crises, and youth unrest, schools were closed for a significantly large number of days during the years 2000–2002. In this environment, a large proportion of school children in upper grades were unable to receive an adequate level of SRH education from the school education. Compared to their older cohorts, these youth will be in a vulnerable situation without having scientific knowledge of SRH education.
Comprehensive SRH education was conducted as a pilot study in the Western province of the country in 2019 3 . However, scaling up this course to be implemented country-wide and continuation in the schools of the Western province was disrupted due to COVID-19 and the economic recession. This was initially recommended to be included in the Grade 9 curriculum but was pushed back to Grade 12 due to the resistance from the Education and political sectors.
Among the unmarried male youth of the 15–19 group, more than 22% had experience in sexual intercourse, while 9% of female youth had the same. The same survey of 2018 further revealed that among the sexually active 15–19 age group 60% and 57% of males and females respectively used contraceptives to avoid unwanted pregnancies which indicated that more than one-third of the never-married youth who were sexually active had unprotected sex3,17. At the same time, national data indicate a significant increase in STI cases, particularly among the youth in the country10,13.
These findings highlight the vulnerability of unmarried youth in Sri Lanka and the limited contribution of school education and out-of-school education toward providing SRH information to them18,15,1. This situation would have further worsened due to the COVID-19 pandemic 3 . SRH targeted interventions to improve the present situation could be implemented effectively only with the right policies and strategies backed by a political, legal, and administratively conducive environment.
Conclusion
The study findings highlight a concerning lack of knowledge on SRH among unmarried youth in Sri Lanka, leaving them vulnerable to a range of challenges related to SRH. Despite recognizing the importance of SRH education, the majority of young people surveyed reported a lack of access to such education through schools. This underscores the need for comprehensive and age-appropriate SRH education to be integrated into both school-based and out-of-school settings.
The only policy/ strategic plan that covers the SRH aspects of youth adequately was the National Strategic Plan- Adolescent and Youth Health (2018–2025) by the Family Health Bureau. COVID-19 and the economic recession have impacted the implementation of key interventions in the National Strategic Plan on Adolescent and Youth Health (2018–2025). Many bottlenecks have prevented the progress of many interventions in the National Strategic Plan. Identifying and addressing such bottlenecks, and proper implementation of the policy with the support of the State, private, and NGO sectors could bring adequate scientific knowledge among the Sri Lankan youth, and that will reduce their SRH vulnerabilities to a greater extent.
Footnotes
Acknowledgements
We acknowledge all the heads and administrative staff of surveyed institutions including universities, vocational training centers, private tuition classes, workplaces and NGOs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was obtained from Ethics Review Committee of ChildFund, Sri Lanka (2019/01).
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by the Child Fund Sri Lanka.
Informed Consent
Informed written consent was obtained from all the participants recruited for this study.