
Abstract
Background and Objectives:
Risky behaviors are common among patients with substance use disorders. Knowing the determinants of risky sexual behaviors can identify individuals who may benefit from targeted interventions. The primary aim of the study was to assess unprotected risky sexual behavior and its sociodemographic and clinical correlates in treatment-seeking opioid-dependent patients.
Methods:
A cross-sectional exploratory study was done on 112 married treatment-seeking opioid-dependent male patients. A semi-structured proforma consisting of sociodemographic and clinical details was used to assess sexual behavior, other risky behaviors like injecting drug use (IDU), and knowledge of and attitude toward risky sexual behavior.
Results:
The mean age of the sample was 34.1 years, and that at first sexual intercourse was 18.6 years. History of unprotected risky sex (unprotected sex with a casual partner or female sex worker or person having a sexually transmitted disease or with males or having sex for rewards) was present in 30 patients (26.8% of the sample). Unprotected risky sex was found to be significantly associated with younger age at first sexual encounter (p = .010), more sexual partners (p < .001), greater frequency of masturbation (p = .031), and watching pornography (p = .028). However, it was not found to be related to other risky behaviors such as IDU (p = .210) and sex under intoxication (p = .149) and also did not vary between treatment-naïve and under-treatment populations (p = .434). No significant relationship was found between knowledge and attitude about risky sexual behavior and unprotected risky sex in the present sample.
Conclusion:
Risky sexual behavior in opioid-dependent patients is a concern, as this may be an additional mode of transmission of blood-borne viruses apart from IDU. Safe sex practices need to be emphasized in this population, and efforts at behavioral changes are desirable.
Introduction
Unprotected risky sex is one of the major concerns in substance using population. It increases the risk of contracting sexually transmitted infections (like HIV). 1 These consequences can increase the burden of illness in patients suffering from substance use disorder. Use of illicit substances as well as alcohol and tobacco have been associated with risky sexual behavior with the risk being about double for male substance users than female users. 2 Studies have documented people receiving treatment for alcohol and drug use or who use multiple drugs to be more likely than others to engage in risky sexual activity. Literature suggests consistent links between illicit drug use and reduced use of condoms.3,4
Opioid-dependent patients are also exposed to a greater risk of contracting these infections when opioids are used through the injecting route and drugs/paraphernalia are shared. In India, opioids are the most common drugs that are used through the injectable route. 5 Most studies regarding unprotected risky sex have looked into patients abusing multiple substances or patients who are only on some specific treatment for opioid dependence.
Risky sexual behavior has been prevalent in patients suffering from substance use disorder.6,7 A study of risk behaviors among 303 opioid-dependent individuals entering integrated buprenorphine/naloxone and HIV care reported risky unprotected vaginal or anal sex in the previous 90 days in 24% of the individuals. 8 Apart from substance use, behaviors like injection drug use contribute to an increased risk of HIV transmission among individuals with substance use disorders. 9 Persons who inject drugs are involved in various risky sexual practices such as casual sex, unprotected sex, and multiple partners. 10 In a study of 1,250 patients with opioid dependence, 36% participants reported condomless sex with a primary partner, 4% reported condomless sex with a non-primary partner, and 6% reported multiple sex partners. 10 These risky sexual behaviors, however, did not differ significantly between those on agonist maintenance and those on short-term detoxification. Another study reports that initiation of methadone maintenance treatment seems to be reducing the risk of risky sexual behavior in opioid-dependent male patients but composite sex risk score increased in the buprenorphine group. 11 However, a significant reduction in risky sex was seen in female patients receiving methadone or buprenorphine, the two effective treatment options for opioid dependence. In another randomized trial comparing outcomes in opioid-dependent patients on buprenorphine or methadone, only the methadone group had consistent declines in risky sexual behavior while both the groups had marked and equal reductions in injecting risk. 12
Evidence is currently lacking on the risk of indulging in unprotected risky sex in patients with opioid use disorders in India and whether initiation of treatment reduces this risk. One study from India reported that opioid-dependent male patients decreased their contact with commercial sex workers after the initiation of maintenance treatment, either buprenorphine or naltrexone. 13 Most of the Indian literature currently exists on the risk of unprotected risky sex in people who inject drugs, thus not making it clear if injecting drug use (IDU) increases the risk of indulging in unprotected risky sex as compared to the non-injecting population with substance use disorders.13-18 Also, literature on risky sexual behavior predominantly looks into adolescents who are generally non-dependent users of substances. So, it is of relevance to assess the risk of unprotected sexual behavior in adult married males who are using substances in a dependent pattern. In previous studies, terms like “risky sexual behavior” have been used, which include any behavior that increases one’s likelihood of sexually transmitted infections, including having unprotected intercourse, having multiple sexual partners, and having intercourse with an intravenous drug user. 19 Such risky sexual behavior is often very often missed in assessment because of the silence of such behavior. 20 Clinical information and research about such risky behavior has definitive translational value. Another important aspect to be looked into is the relationship between knowledge and attitude toward risky behavior and actual sexual practices. Literature suggests that despite good knowledge, unprotected sexual intercourse and risky sexual behaviors are common.21,22 Therefore, it is necessary to see if awareness regarding sexual risk behaviors translates to the practice of safe sex, especially in opioid-dependent patients who are at an increased risk of contracting infections. Hence, this study aimed to assess risky sexual behavior and knowledge and attitude about risky sexual behavior among patients with opioid dependence (both treatment naïve and maintaining well under opioid substitution treatment). We also aimed to find out the predictors of such risky sexual behaviors.
Methods
Study Type and Settings
The study was a cross-sectional assessment of patients attending the outpatient department of a tertiary care addiction treatment facility, affiliated with a medical school. The participants were recruited by purposive sampling. Only married adult males suffering from opioid dependence syndrome (heroin users), as per the International Classification of Diseases-10th edition (ICD-10), were included provided there was a history of sexual intercourse (viz., vaginal/anal/oral) within the last month and if the participants were living with their partners. They were recruited irrespective of treatment status (treatment-naïve, i.e., seeking formal treatment for opioid dependence for the first time, or under buprenorphine maintenance treatment and abstinent, as per self-report). Those who had ever injected drugs in their lifetime were categorized as people who inject drugs (PWID). The exclusion criteria included history of dependence on any other psychoactive substance as per ICD-10 (except tobacco), significant psychiatric/cognitive/medical comorbidity (as per history and clinical examination), or unwillingness to give written informed consent and participate in the study.
Study Instruments
The study instruments included semi-structured proforma consisting of sociodemographic and clinical details. The proforma also included details on sexual history, particularly information about unprotected risky sex (unprotected sex with a casual partner or female sex worker or person having a sexually transmitted disease or with males or having sex for gifts/money/rewards). The proforma also included 12 questions about knowledge and attitude toward risky sexual behavior and the risk of contracting HIV/sexually transmitted disease.
Procedure
Ethical clearance was taken from the institutional ethical committee before starting to recruit patients for the study. Written informed consent was taken from patients who were included for participation in the study after screening. The assessments were carried out in a single session (NC, AC, and SV). The data collection was done from October 2018 to February 2021. The study was done in accordance with the principles enshrined in the Declaration of Helsinki.
Statistical Analysis
Statistical analysis was carried out using SPSS 25.0. The descriptive data was described using means, standard deviations, frequencies, and percentages. The various sociodemographic and clinical variables were compared between those having a history of unprotected risky sex versus those who did not have such a history using an independent sample t-test or Chi Square test. For non-normal distribution, Mann Whitney U test was applied. Knowledge of and attitude toward risky sexual behavior were also compared between these two groups.
Results
All 112 participants were married males, suffering from opioid dependence, of whom 63 (57.27%) were treatment-naïve and 49 were on buprenorphine maintenance treatment. The average monthly family income of the group was around ₹24,000. The age of the patients varied from 21 to 56, with the mean age of the sample being 34.1 ± 8.1 years. The age at first sexual intercourse varied from 11 to 35 years, and the mean age at first sexual intercourse was 18.6 ± 3.5 years. The average duration of heroin use in the sample was 9.71 years. All of the patients reported tobacco use. No significant relationship was found between substance use behaviors and involvement in unprotected risky sex (Table 1). The number of sexual partners in a lifetime ranged from 1 to 30.
Demographic and Clinical Differences Associated with Unprotected Risky Sex (n = 112).
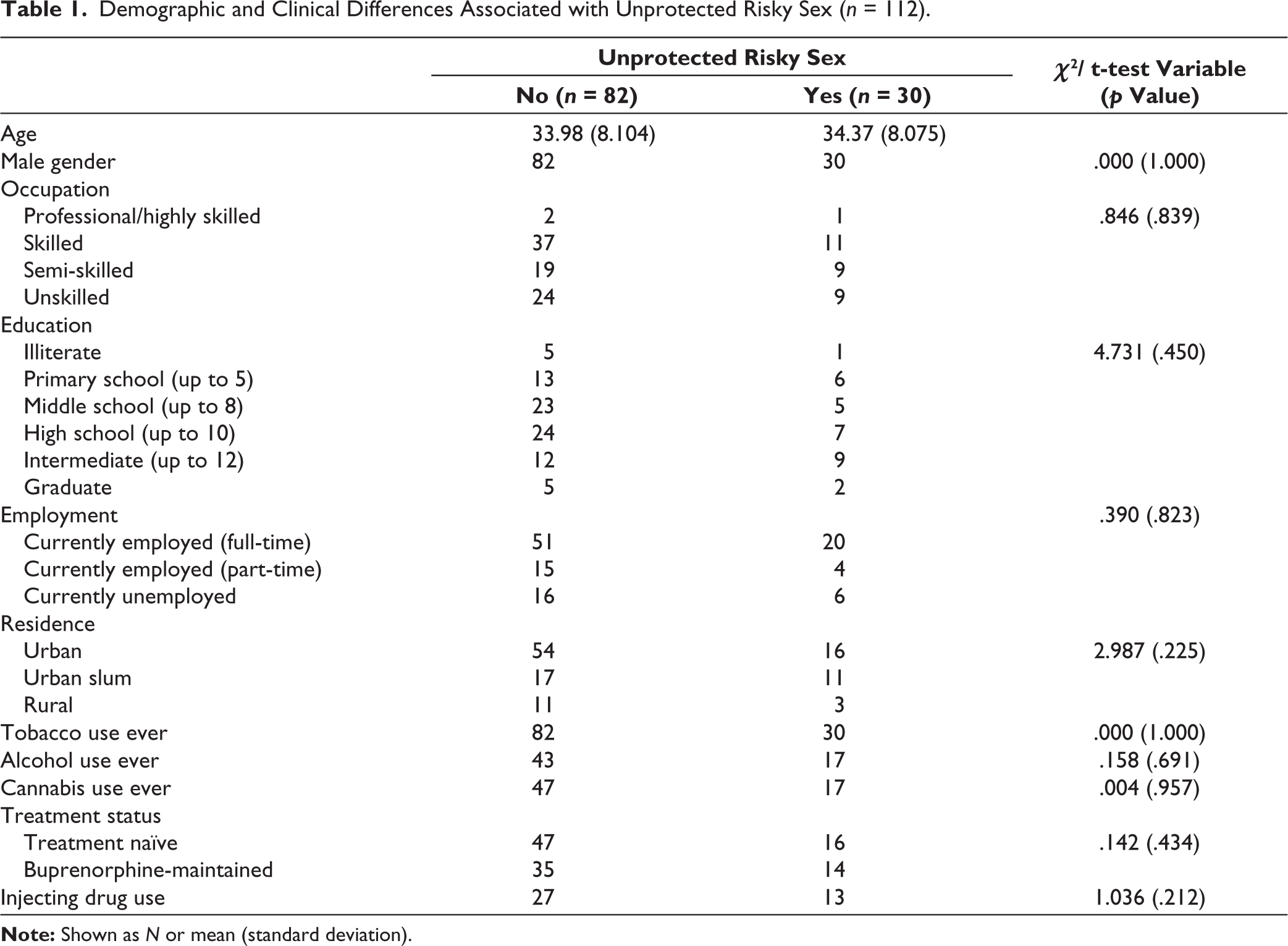
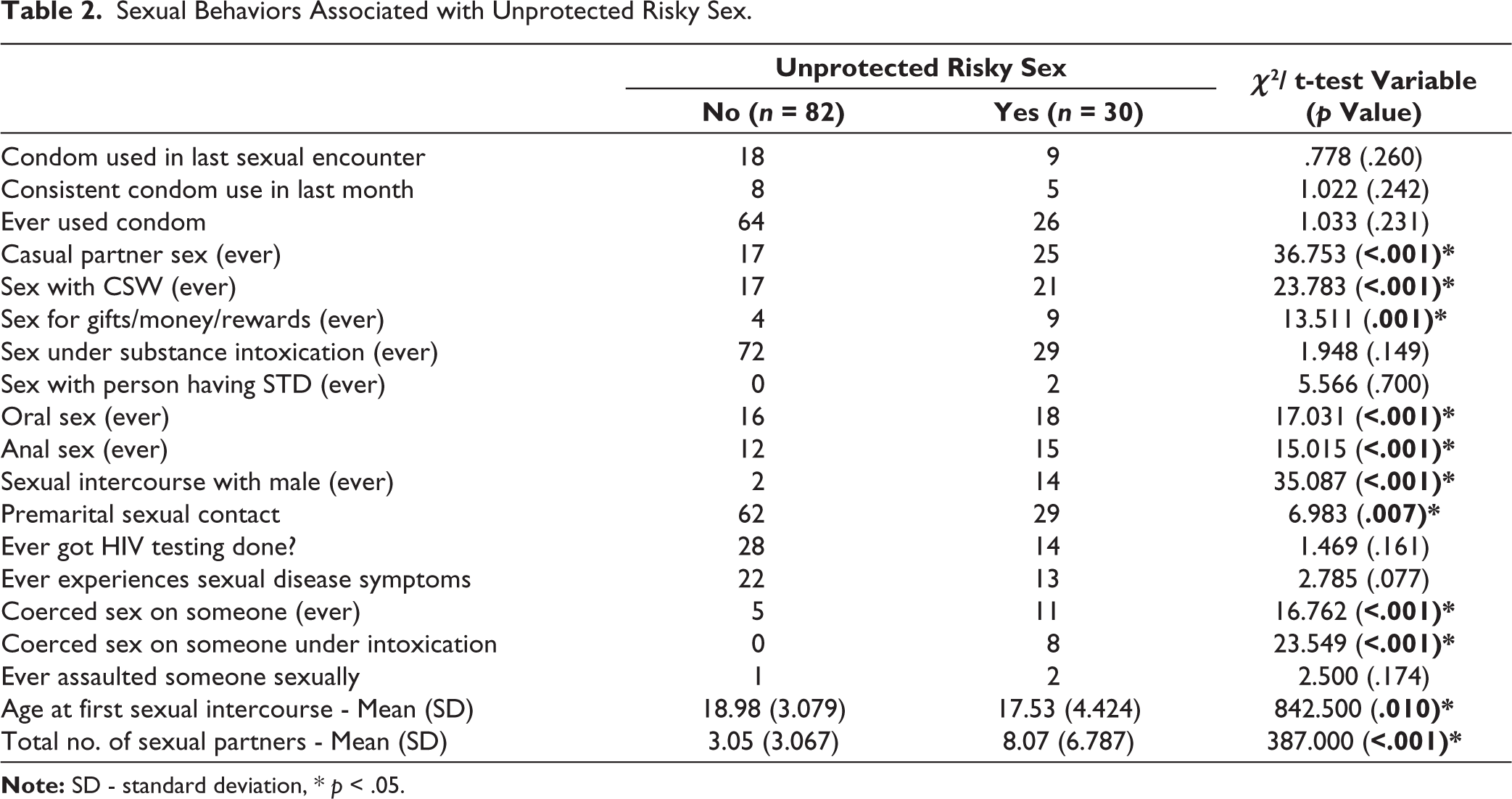
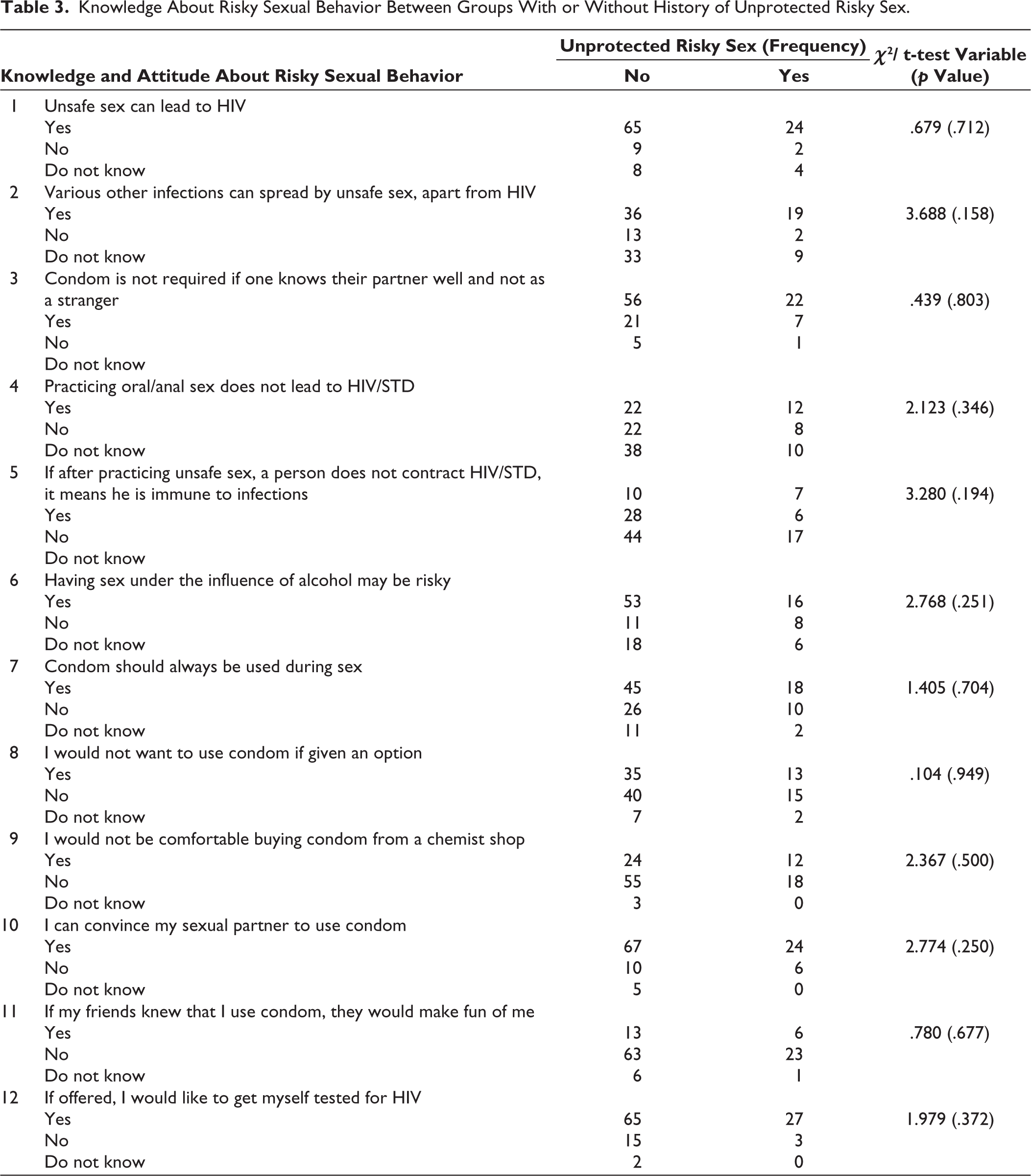
History of unprotected risky sex (unprotected sex with a casual partner or female sex worker or person having a sexually transmitted disease or with males or having sex for gifts/money/rewards) was present in 30 patients (26.8% of the sample). The frequency distribution of each of these risky sexual behaviors has been listed in Figure 1. Unprotected risky sex was found to be significantly related to younger age at first sexual encounter (p = .010), more sexual partners (p < .001), greater frequency of masturbation per week (p = .031), and greater frequency of watching pornography per week (p = .028) (Table 2). However, it was not found to be related to other risky behaviors such as IDU (p = .210) and sex under intoxication (p = .149) and also did not vary between treatment-naïve and buprenorphine-maintained populations (p = .434) (Tables 1 and 2). There seemed to be a significant relationship between a history of unprotected risky sex and oral sex (p < .001), anal sex (p < .001), premarital sex (p = .007), ever coercing sex on someone (p < .001), and ever coercing sex on someone under intoxication (p < .001) (Table 2). There seems to be a trend trend-level significance of association between having a history of symptoms suggestive of sexually transmitted diseases and a history of unprotected risky sex (p = .077). No significant relationship was found between knowledge and attitude about risky sexual behavior and unprotected risky sex in the present sample (p = .158– .803) (Table 3).
The Frequency Distribution of Risky Sexual Behaviors.

Sexual Behaviors Associated with Unprotected Risky Sex.
Knowledge About Risky Sexual Behavior Between Groups With or Without History of Unprotected Risky Sex.
Discussion
This study captured the risky sexual behaviors in opioid-dependent patients who are married and therefore expected to otherwise have a consistent sexual partner. The mean age of the study sample was in the mid-30s, as we have restricted the sample to married patients only in the study design. Most of the available literature looks into risky sexual behaviors in adolescent or young adult age groups, especially, at the initiation of substance use. 19 But in this study, the sample of the patients had an average use of heroin for 9.7 years, and thus, the study focused on a population of fairly long-term dependent opioid users.
More than one-fourth of the study population (30 patients) had a history of unprotected risky sex (unprotected sex with a casual partner or female sex worker or a person having a sexually transmitted disease or with males or having sex for gifts/money/rewards). This is contrasting to previous studies on opioid-dependent patients, which suggest that being married or living with a partner is associated with a protective effect with significantly fewer reports of multiple sex partners and unprotected sex with a nonprimary partner.10,23
Unprotected casual partner sex was the most common followed by unprotected sex with female sex workers or with males followed by unprotected sex for rewards and lastly unprotected sex with someone having a sexually transmitted disease. This pattern resonates with previous studies on injecting drug user population in India, where a high prevalence of unprotected anal sex has been documented among men who have sex with men.24,25 Though unprotected sex with a casual partner was the commonest, it was still low as compared to a previous study on injecting drug users in Delhi, where consistent condom use was seen only in 27% of cases. 17 Interestingly, in this study, unprotected risky sex was not found to be related to IDU. While much literature points to IDU being associated with risky sexual behavior, there is some literature to the contrary as well.10,26,27 Overall, unprotected risky sex was significantly related to younger age at first sexual encounter, more sexual partners, greater frequency of masturbation per week, and greater frequency of watching pornography per week, which reiterates the importance of taking adequate sexual history in the patients. Previous literature shows a significant association of lower risky sexual behaviors among HIV-uninfected persons with IDU in older age. 10 But in the current study, risky sexual behavior was not found to be significantly associated with age, probably due to less heterogeneity in the study sample in terms of age.
In the existing literature, substance use, especially alcohol use, is significantly associated with unprotected sex acts among injecting drug users primarily dependent on opioids. 10 Even in men undergoing treatment for substance use disorders, sex under the influence of alcohol or other substances increased the likelihood of engaging in unprotected casual vaginal or anal intercourse. 28 But in our study, we could find no significant relationship between additional substance use behaviors and involvement in unprotected risky sex. This indicates that the tendency to engage in any substance use predisposes to risky sexual behavior, pointing to a common risk-taking trait at the individual level rather than an effect of different substances. Also, unprotected risky sex did not vary between treatment-naïve and buprenorphine-maintained populations, which is consistent with previous studies that have shown long-term buprenorphine to be significantly associated with a reduction in drug injection risk, but not associated with a reduction in risky sexual behavior. 10 This finding points to the need for more focused and intensive efforts to educate and promote safe sex practices in the treatment-seeking population, even as the treatment progresses and drug use reduces.
In the current study, no significant relationship was found between knowledge and attitude about risky sexual behavior and unprotected risky sex, making it important to assess and understand the risky sexual practices of all patients irrespective of their knowledge and attitude about the same. This finding points out the fact that just having adequate knowledge about risky sexual behavior might not translate into safe sexual practices, for which other individual factors like personality traits may play a role.
Thus, adequate efforts are needed to assess the sexual history in detail in these patients where unprotected risky sex can add to their morbidity and mortality subsequently. The contact with the treating team should be considered as a serious opportunity to reiterate the necessity of safe sex practices to prevent unwanted infections and pregnancies. In India, hetero-sexual transmission is the leading cause of transmission of HIV (83.1%). 29 Therefore, it is very essential to prevent such transmission through unprotected risky sex. Safe sex practices need to be emphasized more diligently in this population where good knowledge and attitude toward risky sexual behavior fail to prevent the same. Efforts at behavioral changes regarding the same during seeking treatment are therefore desirable to prevent further risk of infections and subsequent morbidity. Such efforts should be tried for all substance users irrespective of the number or type of substances being used and the degree of dependence. Previous literature suggests that a greater change occurs when information provision is coupled with skill-based safe sex training and risk sensitization. 30 Another study used two personalized sexual behavior counseling sessions and three booster telephonic sessions and reported improvement in the median percentage of safe sex episodes (though a significant difference was seen in the main outcome of no unprotected intercourse in the last three months). 31 Thus, different methods including information provision, counseling, and skills enhancement can be implemented.
Our study, however, had a few limitations. It was limited to married males; therefore, the risk of unprotected risky sex in opioid-dependent patients who are single may vary. It was a cross-sectional study, with purposive sampling; thus, causal attributions must not be drawn. The study has been done in a tertiary care addiction treatment facility, thus limiting the generalizability of the findings. There was no control group to compare the findings with.
To conclude, risky sexual behavior in opioid-dependent patients is a concern, as this may be an additional mode of transmission of blood-borne viruses especially in patients, who also practice other risky behaviors like IDU. Presence of any history of sex with a casual partner or female sex worker or with males or having sex for gifts/money/rewards or oral sex or anal sex or premarital sex or ever coercing sex on someone or ever coercing sex on someone under intoxication should alert the clinician about increased possibility of unprotected risky sex in the patient. Future studies might look into the change in the occurrence of unprotected risky sex longitudinally during the treatment course of the patient and its relationship with intermittent safe sex education being received by the patient during outpatient follow-ups. It would be interesting to see if similar findings occur in female opioid-dependent patients as well and investigate further into the variables associated with unprotected risky sex in them.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was taken from the institutional ethical committee before starting to recruit patients for the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was taken from patients who were included for participation in the study after screening.