
Abstract
Background:
Gender inequality, cultural taboos, poverty and lack of proper information can cause menstrual health needs to go unmet. It restricts mobility, personal choices, work participation and well-being. Nevertheless, self-efficacy in the menstrual hygiene management of college students has been relatively unexplored.
Objectives:
We aimed to assess the self-efficacy of menstrual hygiene management and its association with college absenteeism, demographic and academic profiles. The study also aimed to explore concerns and beliefs related to menstruation.
Materials and Methods:
A cross-sectional descriptive mixed-method study was conducted to assess the self-efficacy of the menstrual hygiene management (using a novel scale) of students from a general college in Kolkata, West Bengal, India. The study also explored concerns and beliefs related to menstruation among the study subjects. The sample size was calculated to be 96. For the qualitative part, 30 willing students were purposively chosen.
Results:
The mean age of participants was 19.38 years (SD ± 1.23). Predominantly they belonged to nuclear families (65.6%) with a median family income of ₹12,000. Absenteeism for menstrual reasons was 12 (12.5%). There were 50 (52.1%) participants who reported facing religious restrictions. Self-efficacy had a mean score of 29.90 (standard error of mean = 0.513) and a median score of 31. The presence of religious restrictions, any restrictions and type of family were significantly associated with college absenteeism by the chi-square test (P < .05). The logistic regression model showed a significant association with religious restriction.
Conclusion:
The study revealed multiple concerns of college-going students regarding menstrual hygiene despite reported high self-efficacy for menstrual hygiene management.
Introduction
Menstrual health and hygiene is essential to the well-being and empowerment of women and adolescent girls. An estimated 500 million women lack access to menstrual hygiene products and adequate facilities for menstrual hygiene management. 1 Girls and women require access to water, sanitation and hygiene facilities, affordable appropriate menstrual hygiene products, supportive environment and information on good practices to effectively manage menstruation without embarrassment or stigma.
Unmet need of menstrual hygiene affects school attendance, participation in community life and also compromises women’s safety, causing additional stress and anxiety. 2 A meta-analysis on the status of menstrual hygiene among adolescent girls in India found that a quarter of the girls did not attend school during menstruation because of the lack of adequate toilets. 3 In South Sudan, the percentage of school absenteeism was 57% during menstruation. 4 A survey in Bangladesh found that only 6% of schools provide education on health and hygiene, and only 36% had prior knowledge about menstruation before their first period. 5 Successful approaches in Ghana effectively combined information and education with appropriate infrastructure and menstrual products. 6 Menstrual issue is shrouded by taboos in traditional societies, with various restrictions imposed on menstruating women.7,8 Mahila Visava Kendras or Women’s Rest Centres of Gadchiroli innovatively addressed such taboos, emphasizing a broad range of issues around menstruation beyond hygiene—questions of security, safety, stigma, taboo and policy ownership. 9
Besides matters of policy and community engagement, the role of self is no less important in managing menstrual issues. Self-efficacy is an individual’s belief in their capacity to act in the ways necessary to reach specific goals. Perceived self-efficacy refers to people’s beliefs about their ability to control their own activities and can be an important tool for health promotion. 10
Our objectives were to assess the possible role of self-efficacy in menstrual hygiene management and its association with absenteeism, demographic and academic profiles.
While menstrual absenteeism has been well researched among school-going girls, not many studies are there among college students. Moreover, self-efficacy scales were not used in research on menstrual health. The study also aimed to explore concerns and beliefs related to menstruation among the study subjects.
Materials and Methods
Study Design and Setting
This was single-institution–based cross-sectional, observational descriptive mixed-method study.
The study was conducted at a girls’ general college in Kolkata, West Bengal, India. The college had 3 streams—humanities, commerce and science—with an intake of 400 students per year. At the time of data collection, the college had 1,200 students in 3 batches.
Study Participants and Sampling
All students of first and second-year batches understanding English and willing to participate were eligible.
For the quantitative part, first- and second-year batches were selected as the final years were unavailable due to upcoming exams. Thus, out of 800 students, the requisite sample was selected randomly from students’ roll numbers, and for the absence of selected roll numbers, the next available roll number was taken.
The sample size was 87, considering the prior prevalence of 82.3% 8 of desirable menstrual hygiene management, with α error of 10%, an estimated population size of 800, a precision of 99% and a design effect of 1.3. To this, 10% non-response was added to make a final sample size of 96.
For the qualitative part, 30 willing students were purposively chosen.
Study Tools
The study tool consisted of a pretested predesigned structured self-administered questionnaire for data collection. The tool for self-efficacy was a self-administered novel scale, developed by the research team and content-validated by in-house experts in the field. The tool captured variables such as self-efficacy score, absenteeism and variables related to socio-demographic characters. For qualitative exploration, a free listing of concerns about menstrual hygiene was done by the participants.
Technique of Data Collection
Data were collected in September 2022. Participants were asked to fill out the questionnaire. Then, 30 willing students were asked to free-list their menstruation-related concerns. The entire study was completed in 3 months, from August to October 2022.
Data Entry and Statistical Analysis
After verification, the data were entered into a Microsoft Excel worksheet (2010 version). Analysis was done with Statistical Package for Social Sciences version 17. Descriptive measures were reported in terms of frequencies and percentages for categorical variables. Mean, median and standard deviation were used to describe the continuous variables. The difference of means for the self-efficacy score was checked across subgroups. Finally, multiple logistic regression was done to check for associations. For all statistical tests, P < .05 was considered statistically significant.
For qualitative exploration, free-listed items were coded and similar codes were grouped into themes.
Ethical Consideration
This study was compliant with Helsinki Declaration on bioethics policy. All respondents provided informed consent. Data collection was anonymous and data were unlinked during data entry. Blinded analysis was performed. The study protocol was approved by the institutional ethics committee of Medical College Kolkata with reference number MC/KOL/IEC/NON-SPON/1488/08/2022 dated 08/08/2022.
Results
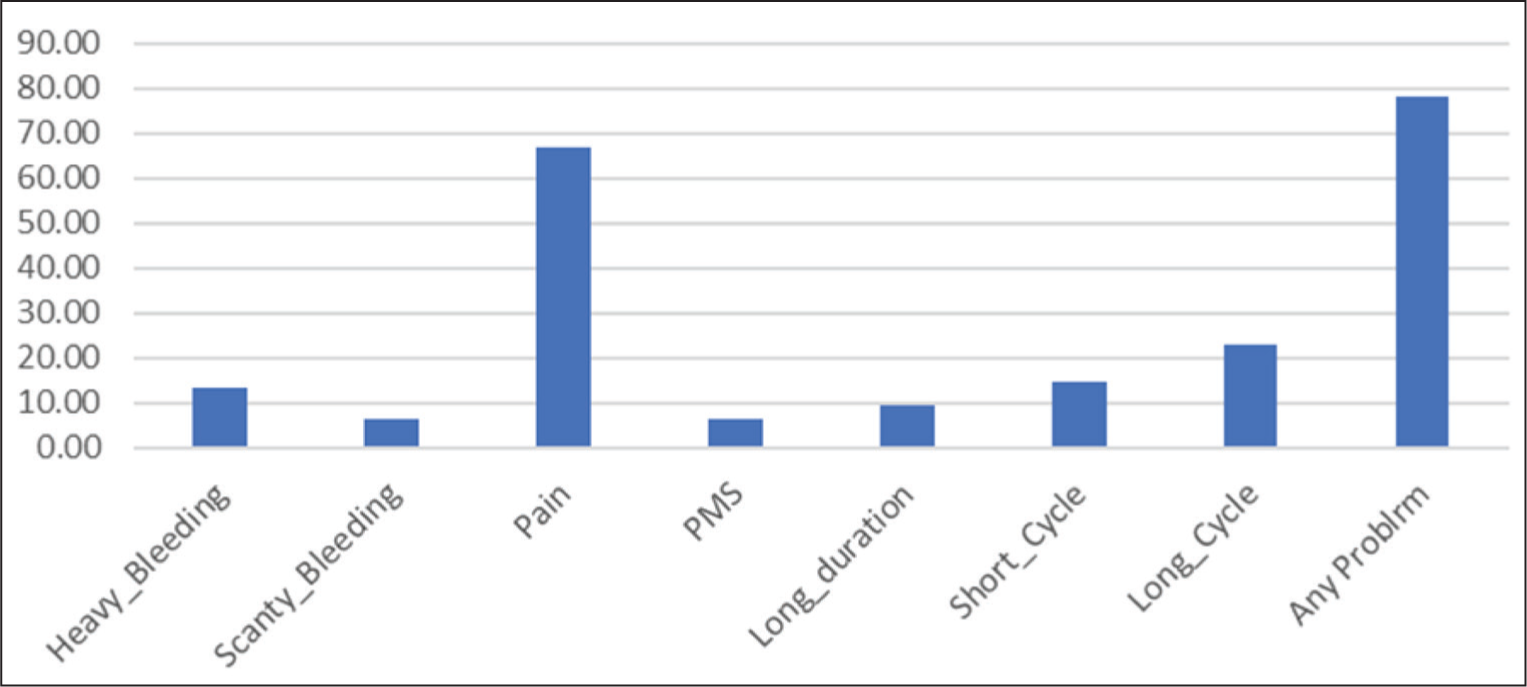
A total of 96 respondents completed the questionnaire. The mean age of the respondents was 19.38 years (SD ± 1.23). Predominantly, respondents belonged to nuclear families (65.6%), and the median family income was ₹12,000, with an income range of ₹3,000–₹90,000 per month. The majority, that is, 76 (79.2%) respondents, reported that they acquired information about menstrual hygiene from their mother while only 14 (14.6%) reported having acquired information from the internet. There were 75 (78.12%) girls who reported having menstrual problems, but none had sought professional consultation. Figure 1 shows various menstrual problems reported by the respondents. Among the respondents, 12.5% reported having been absent from college during their menstrual cycle within the last 3 months. Fifty (52.1%) participants reported facing religious restrictions during their menstrual period at their family level.
Bar Diagram of Menstrual Problems as Reported by the Respondents (n = 96).
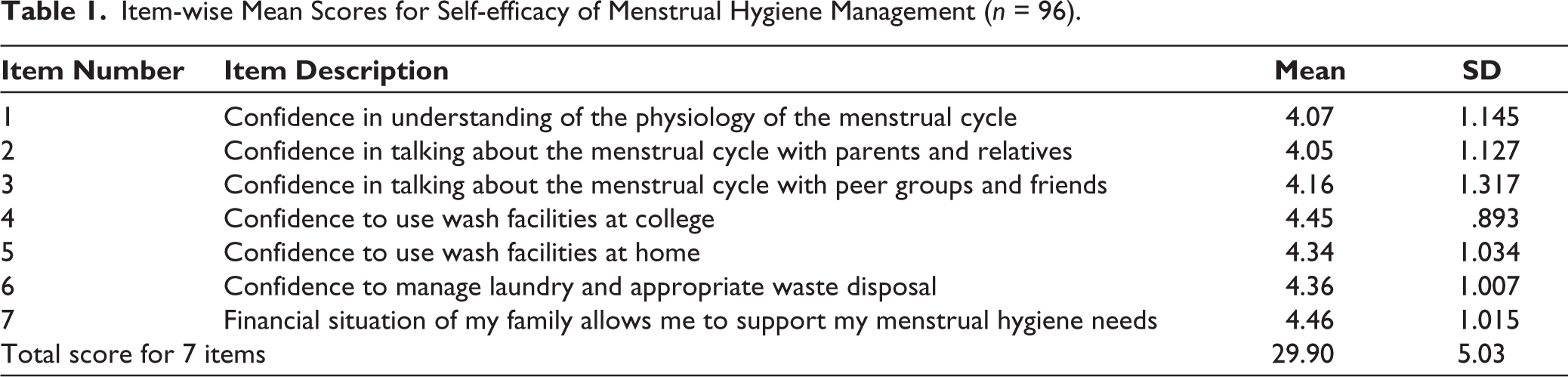
Cronbach’s α for the 7 items, related to self-efficacy of menstrual hygiene management, was 0.787, showing good reliability. The minimum self-rated score was 7 and the maximum score was 35, with a mean score of 29.90 (standard error of mean 0.513) and a median score of 31. Although the respondents reported a high level of self-efficacy for all items, the mean for items 1 and 2 was comparatively lower. Table 1 shows each item’s mean score and standard deviation.
Item-wise Mean Scores for Self-efficacy of Menstrual Hygiene Management (n = 96).
Mean scores were not significantly different across demographic, scholastic and menstrual hygiene categories except for the year of study (higher for first-year students) and the number of absorbents used per day (higher for those who used 4 or more absorbents) as shown in Table 2. All the subcategories were dichotomized, and equal variances were assumed for both categories. Only the subcategories of the number of absorbents used per day had unequal variance by Levene’s test, the degrees of freedom were corrected to 93.998.
Mean Scores for Self-efficacy of Menstrual Hygiene Management Across Subcategories of Respondents (n = 96).
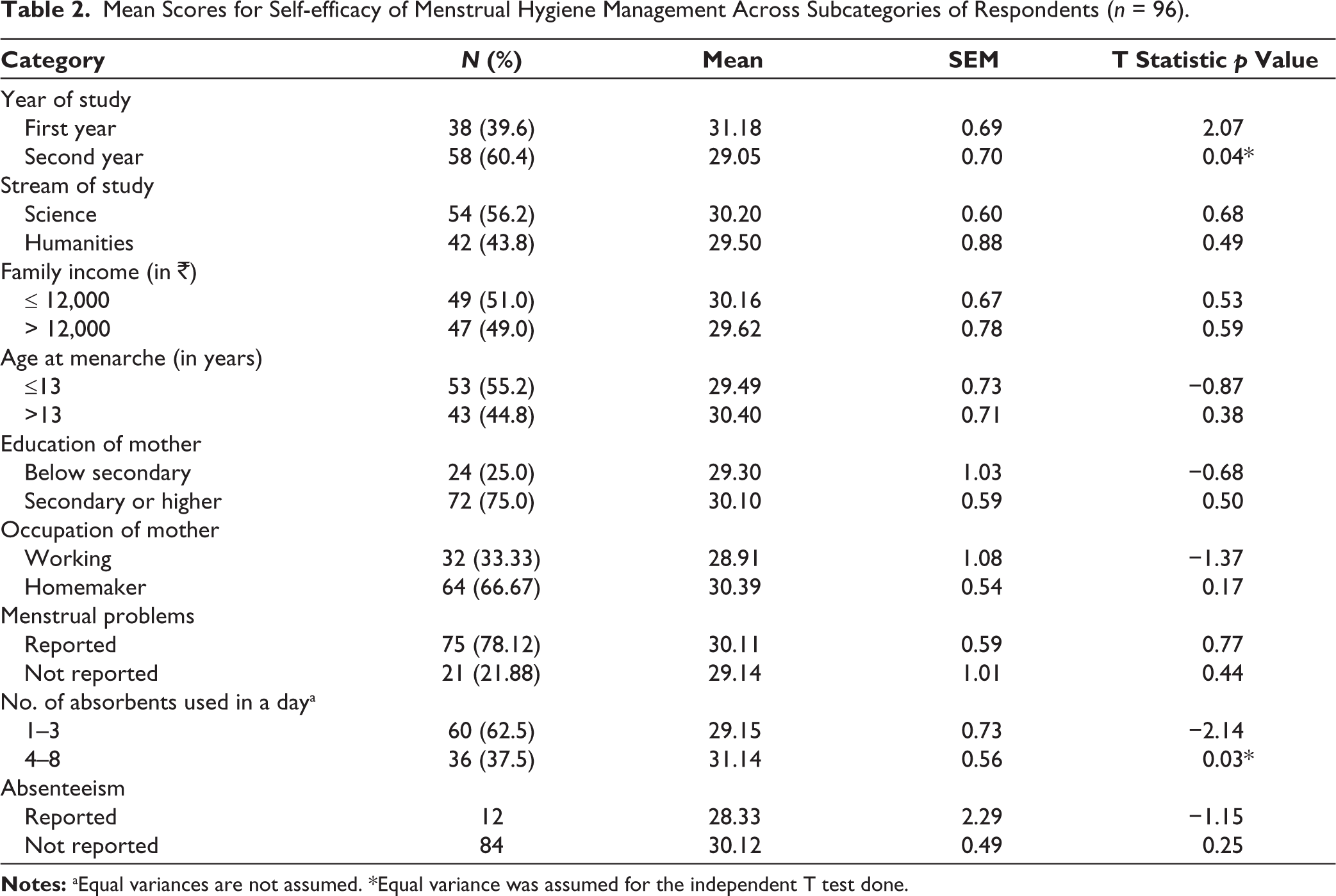
Statistical analysis revealed that students who reported being absent during their menstrual cycles did not rate their self-efficacy any differently from their peers.
The variables presence of religious restrictions, any restrictions and type of family were significantly associated with college absenteeism by the chi-square test (p < .05). Categories were created by recoding self-efficacy scores into ≥ mean score (higher scores) and < mean score (lower score) categories. This score category and a few other variables having P values between 1 and 0.5 were included in the logistic regression model besides those variables showing significant association by the chi-square test. Nagelkerke pseudo-R2 value for the model was 0.816, indicating good model fit. Table 3 shows the parameter estimates for logistic regression; only religious restriction was associated with college absenteeism during menstrual cycles in this model. Girls who reported having religious restrictions were 99% more likely to be absent from college during their menstrual cycles.
Parameter Estimates by Logistic Regression for College Absenteeism During Menstrual Cycles Across Subcategories of Respondents (n = 96).
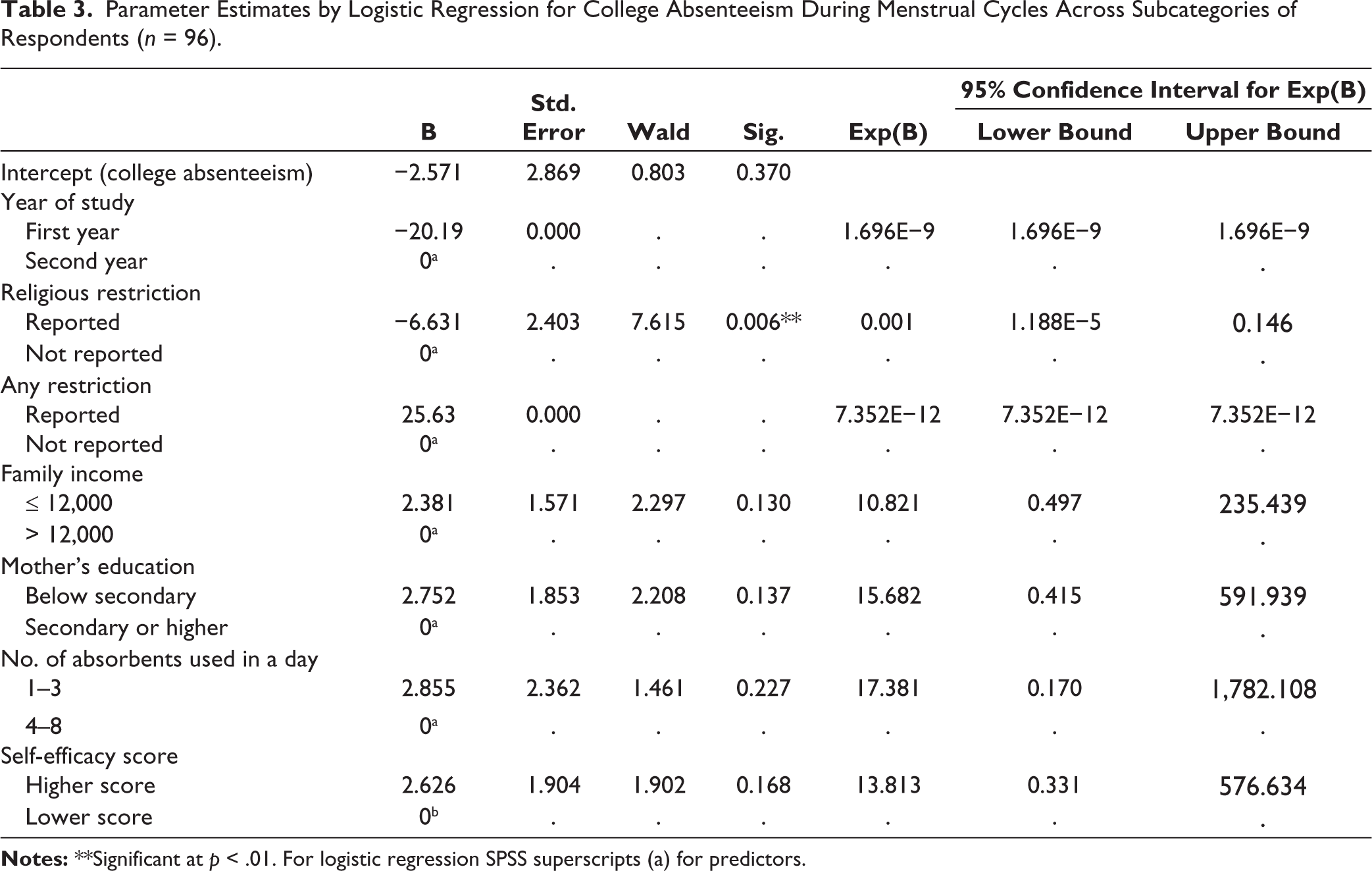
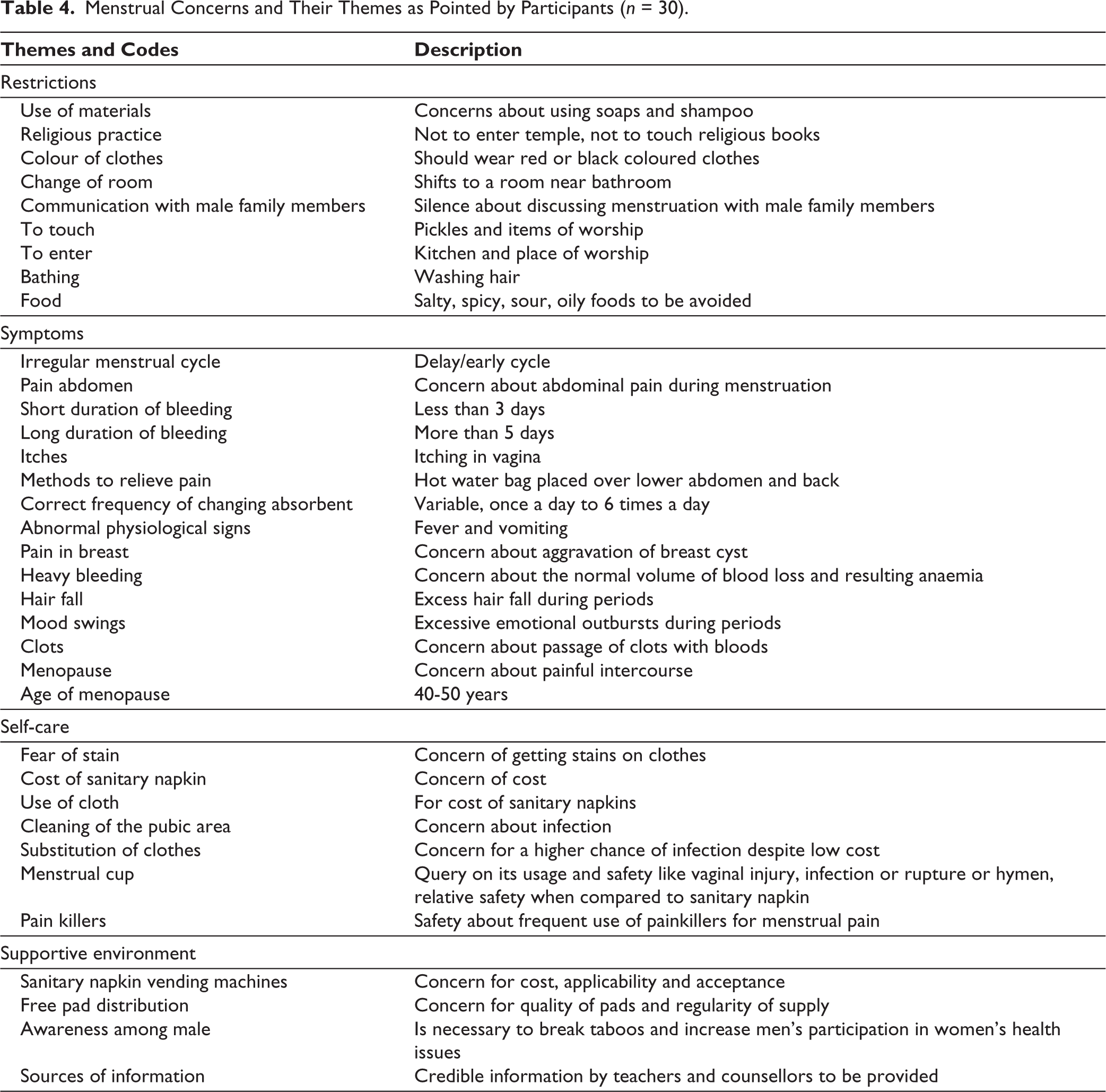
Table 4 shows the free listing of menstrual concerns by the participants. Thirty students volunteered to take part. Concerns expressed were coded under 4 themes: restrictions, symptoms, self-care and supportive environment. There were 34 different codes under these 4 themes.
Menstrual Concerns and Their Themes as Pointed by Participants (n = 30).
Discussion
This study explored self-efficacy and concerns of college- going young women about their menstrual cycles. The participants reported a high level of self-efficacy, which was similar across categories and had no association with college absenteeism. Concerns expressed by the participants were coded under 4 themes: restriction, symptoms, self-care and supportive environment.
Despite various medico-social advancements, menstrual hygiene remains poorly understood. Comparison of the knowledge-practice gap across populations is limited by the lack of valid, reliable and agreed-upon indicators. Measurement challenges have been considered major barriers to research on menstrual hygiene. 11 The scale used in the present study attempted to measure a specific construct, self-efficacy, in managing menstrual hygiene. However, this scale measure did not show any association with absenteeism. It is also possible that there are latent constructs of self-efficacy which remained unmeasured by this scale.
In the present study, 12.5% of girls reported absenteeism. Between 11% and 23% of women aged between 15 and 49 years from the African countries of Burkina Faso, Niger and Nigeria had reported school and work absenteeism due to menstruation. 12 It had been reported that restrictions imposed during menstruation and lower education levels of mothers were associated with higher school absenteeism while the availability of pain medication at school lowered this.13,14 In the present study, absenteeism did not appear to be higher with menstrual problems, rather it pointed to a cause within the family. Restrictions imposed during menstruation are much related to the perceived gender roles. A study from Nepal reported that 66.1% of participants had a range of restrictions during menstruation, the commonest being religious restrictions. Around 70% of participants reported their mothers encouraged them to impose restrictions. 15 Near universal religious restriction was also reported from the survey of school girls in 3 states of India. 3 A meta-analysis of Indian studies had the pooled prevalence for religious restrictions during menstruation in adolescent girls as 77% (95% confidence interval: 71%–83%), which was much higher than the present study. Garg et al attempted to measure menstruation-related activity restriction with a 6-factor questionnaire by principal component analysis. In this questionnaire, restrictions related to work, religion and social life are mentioned as 3 different factors. 16 This corroborates with the present study result where only the religious restriction was associated with absenteeism.
Mother was the primary source of knowledge in the present study and agreed with the meta-analysis by Sooki et al. 17 An intervention with 3 arms (girls’ education, mothers’ education and no education) conducted by Afsari et al among school-going adolescent girls of Tabriz city, Iran, reported significantly improved attitude score compared to other 2 groups. 18 In the present study, however, the educational variables of either the girls or their mothers had no relation with absenteeism or self-efficacy.
Participants of the qualitative component of this study expressed 1 or more concerns related to menstruation. While the items on the self-efficacy scale are more related to sanitation practices, these concerns go beyond washing and disposal of absorbents; they touch upon the vital transactions between the menstruating girl and her surrounding social environment. Some girls expressed concerns about the non-engagement of men in menstrual issues. A qualitative study conducted in Nashik, Maharashtra, India, reported the positive effect of mothers’ college education and comfort level with teachers on influencing the boys’ belief in menstrual hygiene. 19
The strength of this study is the attempt to find a quantitative measure for behaviours related to menstruation that can be used in programmatic management.
Limitation and Recommendation
Limitations of the study are a small sample size, sampling from a single site and possible unmeasured latent factors of self-efficacy. Further research should involve necessary modification and construct validation of the self-efficacy tool. Behaviour change related to myths and taboos of menstruation is much needed.
Conclusion
The study reveals the concerns of college-going students of a developing country regarding menstrual hygiene and their self-efficacy for menstrual hygiene management. Even though the scores were high, the study revealed universal religious restrictions and persistent taboos clouding their thoughts.
Footnotes
Acknowledgements
The authors are grateful to all the study participants for sharing their views. We are also grateful to the principal, faculties and counsellor of Victoria College, Kolkata.
Author Contributions
Concept and study design: MD and DG; permissions, implementation and data collection: SY; planning of data analysis: MD; data analysis, literature review: MD and SY; editing the draft: MD and SY.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed
The authors certify that they have obtained all appropriate participant consent forms. In the forms, participants have given his/her/their consent for his/her/their images, data and opinion to be reported in the journal. The participants understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Disclosure
Mousumi Datta was posted in Medical College Kolkata, West Bengal, India during the study period.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.