
Abstract
Background:
HIV is often perceived by many Rohingya individuals as a common ailment, similar to a cough or fever. Given the biological vulnerability of Rohingya women, increasing awareness programs within this population becomes crucial. Therefore, it is important to assess the current knowledge status of STIs/HIV among Rohingya individuals.
Objectives:
This study aimed to evaluate the knowledge of STIs/HIV and explore the impact of media usage and communication activities among Rohingya refugee women residing in Cox’s Bazar, Bangladesh camps.
Methods:
A quantitative research approach was employed, utilizing a camp-based cross-sectional sample survey with a structured and facilitator-administered questionnaire. The study involved 415 refugee women as respondents. Hierarchical regression analysis was conducted to identify factors influencing STI/HIV knowledge.
Results:
The findings revealed that approximately two-thirds of Rohingya refugee women lacked accurate knowledge regarding STI/HIV-related myths and misconceptions. Regression analyses indicated that being a professional (β = 0.14; p = .003), engaging in discussions about STI/HIV with healthcare workers (β = 0.25, p < .001), visiting clinics or health facilities (β = 0.18, p < .001), and observing banners/posters on STI/HIV (β = 0.20, p < .001) were associated with better STI/HIV knowledge among refugee women. The utilization of communication activities by Rohingya women emerged as a stronger predictor of STI/HIV knowledge compared to socio-demographic factors and media usage-related variables.
Conclusions:
The study findings can inform the development of appropriate communication programs, campaigns, and effective communication materials aimed at preventing STIs within this vulnerable community.
Introduction
The number of individuals forcibly displaced, often classified as refugees, has witnessed a significant increase in recent decades. Among these displaced populations, the Rohingya diaspora in Myanmar, who fled their homes on August 25, 2017, has garnered considerable attention.1–3 This mass migration of over 700,000 Rohingya into Bangladesh has led to the world’s most rapidly escalating refugee crisis.2-–6 Prior to this recent influx, Bangladesh had approximately 220,000 unregistered refugees.2,7 However, as of March 31, 2021, the number of Rohingya refugees residing in 34 camps in Cox’s Bazar District, Bangladesh, reached approximately 884,000, 8 making it one of the world’s largest and most densely populated refugee settlements. 9
Within this densely populated refugee setting, the risk of abuse and the prevalence of diseases such as sexually transmitted infections (STIs) are significantly high. Several factors contribute to this situation, including an escalation in gender-based sexual violence and exploitation,10–14 insufficient information regarding STIs, 13 disrupted healthcare services and limited access to STI/HIV prevention and treatment,15–17 inadequate availability of condoms and other preventive tools,18–20 stigma and discrimination, 19 unsafe sexual practices, and limited access to diagnostic and treatment facilities for STIs. 15
Moreover, poverty and food insecurity can contribute to risky behaviors such as transactional and commercial sex, 19 while migration and displacement disrupt social networks and increase the risk of STI/HIV transmission. 19 The failure to meet basic human needs further exacerbates the situation, leading to transactional sex and a rapid increase in the number of individuals affected by STIs and HIV.15,21 Alarmingly, HIV and other STIs are already prevalent among the people of Myanmar.15,21 According to UNAIDS, 0.23 million people in Myanmar are living with HIV, and 7,800 have died as a result of the illness. Myanmar is listed among the 35 nations where 90% of new HIV infections occur. 22
In 2017, soon after the Rohingya people moved to Bangladesh, a testing program identified 83 cases of HIV. 21 Since then, the total number has steadily increased, from 273 in August 2018 to 319 in March 2019, with the latest estimate of 395 cases in 2019.23–25 Furthermore, as of December 22, 2022, 612 Rohingya individuals residing in Cox’s Bazar camps have been diagnosed with HIV/AIDS, resulting in 61 deaths from the disease.26,27 The actual number of infections could be much higher than the official figure, as many cases go unidentified and asymptomatic.15,24
Experts attribute the spread of the disease to social stigma and a lack of knowledge. 24 Media reports indicate that akin to other conservative societies, the Rohingya people often isolate individuals who are HIV-positive.24,26 Due to fear of stigma, those living with HIV are reluctant to seek medical treatment, and persuading them about the seriousness of the disease has proven challenging. Many patients even disregard their doctor’s advice regarding matters such as sexual intercourse.
The aforementioned background highlights the importance of increasing awareness programs among the Rohingya population, particularly women who are more vulnerable due to biological factors. Therefore, assessing their current knowledge about STIs/HIV is essential. In light of this background, the aim of this study is to evaluate STI/HIV knowledge and explore socio-demographic, media use, and communication activity-related factors among Rohingya women. The findings of this study are expected to provide evidence for the development of integrated and effective strategies to promote knowledge about STIs/HIV within the refugee population.
The article will commence with a concise review of existing literature on STI/HIV in the Rohingya community, followed by a tailored conceptual framework. The subsequent section will introduce the methods and materials employed in the study, and the results will be presented thereafter. The discussion section will provide a summary of the study, practical implications, and limitations.
Literature Review
Most of the studies conducted on the Rohingya population have primarily focused on their sexual and reproductive health (SRH), family planning knowledge, perceptions, and needs, as well as contraceptive usage rates.1,4,9,15,16 However, there is a significant dearth of scholarly work that examines the STI/HIV knowledge status among Rohingya women, leaving a knowledge gap regarding the effectiveness of interventions aimed at improving STI/HIV knowledge among refugee women.
In a study by Khan et al. 15 that explored HIV transmission knowledge among Rohingya refugee women, certain socio-demographic factors such as education and occupational status were found to be associated with higher levels of knowledge among refugee women. However, evidence suggests that improving their socioeconomic conditions within the current settings is challenging. Therefore, employing communication interventions utilizing behavioral change theories and strategic communication approaches may prove to be an effective strategy for enhancing their knowledge. 28 Notably, Khanet al. 15 did not include communication-related factors that could be utilized to enhance STI/HIV knowledge.
Previous literature suggests that the level of HIV/STI knowledge among people in humanitarian and refugee settings is low.29–32 Andari studied people’s knowledge of HIV/AIDS in Yogyakarta and found that many people do not know the transmission mode of HIV/AIDS and nearly half of respondents cannot name a single cause of HIV/AIDS. 31 Globally refugee populations are heavily affected by the HIV/AIDS pandemic and millions of lives and caused suffering to many people and their communities. 33 Conflict displacement increases vulnerability to HIV/AIDS and refugees face discrimination and blame for the disease. 34 HIV prevalence rising in countries refugees emigrate from and providers serving refugees should be well-acquainted with principles of HIV testing and treatment. 35 Beckwith et al. studied HIV-infected refugees from West Africa studied and reported that refugees had a higher likelihood of facing heterosexual risk for HIV. 36 Besides, Dahab et al. measured trends in HIV-related behaviors among refugees and surrounding communities living in Kenya, Tanzania and Uganda and emphasized the importance of ongoing efforts to address HIV-related behaviors and knowledge among both refugee and surrounding national populations in order to sustain and further improve the positive trends observed. 37
There is also some scholarly evidence exploring factors associated with HIV/STI knowledge. Rodríguez-Álvarez et al. argued that inadequate knowledge about HIV is associated with various social factors such as place of birth, education level, and immigration status. 38 The authors suggest that initiatives are needed to promote equity in healthcare provision for immigrants, considering their specific needs and gender issues. 38 Rowley et al. conducted an HIV behavioral survey in a refugee camp and surrounding villages in Tanzania and reported that factors increasing HIV risk among refugees compared to surrounding villages include young age of sexual initiation, high-risk sex partners, limited access to income, and vulnerability of refugee women. 39 Milic et al. revealed factors associated with higher HIV knowledge are studying health-related disciplines, using the internet as a source of information, positive attitude towards HIV testing, low self-perceived risk for HIV infection, and willingness to maintain contact with HIV-positive individuals. 40 Banagi et al. found that upper socioeconomic status is an important factor associated with higher HIV knowledge. 41
Assessing the utilization of NGOs’ health communication activities related to SRH among the Rohingya women in refugee camps can be approached from various perspectives. Zakaria et al. 28 examined the effectiveness of certain health communication interventions, excluding media influences, among Rohingya women living in refugee camps, focusing on SRH but not addressing STI/HIV issues. However, the study suggests that the utilization of health communication programs offered by NGOs emerged as a more significant determinant of positive SRH status than socio-demographic characteristics.
Apart from the socioeconomic status, literature also suggests that health communication activities which are implemented through interpersonal, organizational, and media channels can be utilized to increase HIV/STI knowledge among people.42,43 Accordingly, this study measured the utilization of health communication activities using six variables, including two variables related to organizational communication channels (awareness program in camp, visiting a health centre), one variable associated with the interpersonal channel (discussion of STI/HIV with a health worker), and three variables related to the media channel (listening to the radio, Internet use, viewing posters, banners, and billboards about STI/HIV). Thus, this study aims to address the research gap by examining the six dimensions of media use and the utilization of communication activities to assess the overall influence of health communication on STI/HIV knowledge among Rohingya refugee women.
Research Questions and Hypotheses
Based on the reviewed literature and conceptual framework, our research questions and hypotheses are as follows:
H1: Different characteristics, for example, education, occupation, and age will have an association with the Rohingya refugee women’s good STI/HIV knowledge. H2: Media use will positively affect the Rohingya refugee women’s good STI/HIV knowledge. H3: Utilizations of communication activities have a positive association with the Rohingya refugee women’s good STI/HIV knowledge. H4: Utilizations of communication activities will appear as stronger predictors than demographic variables.
Methods
Study Design and Setting
This study employed a quantitative research approach utilizing a camp-based cross-sectional survey in order to achieve the desired research outcomes. The aim was to explore the descriptive functions related to STI/HIV knowledge among Rohingya refugee women. The study was conducted at Camp-4, located in Cox’s Bazar district, Bangladesh. Camp-4 was purposively selected as the study area due to its status as one of the largest camps with the involvement of various NGOs and INGOs.
Sampling Procedure, Sample Size, and Study Participants
The study included all Rohingya refugee married women of reproductive age (15–49 years) residing in the camps in Cox’s Bazar during the study period. A total of 415 Rohingya refugee women living in the refugee camp in Cox’s Bazar were selected as study participants. Literature suggests that forcibly displaced women across the world are experiencing intensified SRH concerns women, particularly those of reproductive age, are biologically more susceptible to STIs, including HIV.3,44,45 Having accurate STI/HIV knowledge is not only crucial for their health but also has implications for maternal and child health, especially preventing mother-to-child transmission of STI/HIV. Besides, married women often work as the primary source of SRH knowledge for their adolescent daughters. 46
Over a million displaced Rohingya currently reside in specified Rohingya camps 4 , while more than half of Rohingyas in Bangladesh are women.3,47 Conditions of all Rohingya camps are almost the same, while camp-4 was purposively selected as the study area for conducting this camp-based cross-sectional study due to its size and organization, along with the presence of different international and local NGOs. 28 Given the challenges of finding a suitable sampling methodology in the humanitarian context and limited funds, the study participants were chosen using a convenient method. This methodological challenge has been previously encountered in a similar study. 48 The sample size was calculated using the single population proportion formula, taking into account these parameters: p = 50%, significance level at 5% (α = 0.05), Z α/2 = 1.96, and a 5% margin of error (d = 0.05). Assuming a 5% nonresponse rate, the sample size was calculated as follows: n = n + 5% = 384 + 19 = 403. Finally, 415 refugee women were included as study participants. The average age of the individuals was 25.52 (± 6.32) years. Concerning the educational background of the Rohingya refugee women, over half (218, 52.5%) had not received formal schooling. Additionally, 111 (26.7%) achieved less than a primary education level followed by lower secondary (34, 8.2%), primary (33, 8%), and secondary (19, 4.6%). Most of the respondents, 327 (78.8%) were housewives, and the rest of them (88, 21.2%) were involved in different professions. On average, the study participants had 4 (3.96 ± 2.58) children.
Data Collection
Data collection was conducted using a structured and facilitator-administered questionnaire. The questionnaire’s items were taken from existing literature. Ten female facilitators with prior experience in data collection were hired to lead and administer the survey. Additionally, 10 Rohingya women from the survey area accompanied them to assist in data gathering within the camp, creating a comfortable environment for the study participants to engage with the interviewers. All recruited Rohingya women had previous experience working within their community. The facilitators were proficient in the Rakhine/Arakanese language and fluent in the Rohingya dialect, enabling them to effectively communicate the questionnaire’s questions. They had completed higher studies and had extensive experience working in Rohingya camps. To ensure unbiased data collection, data collectors who had worked in NGOs in sectors other than health were recruited. Before distributing the questionnaire to the study participants, the data collectors explained the study’s importance and goals. Each questionnaire took between 20 and 30 minutes to complete, and data collectors reviewed the filled-out questionnaires for completeness.
Data Quality Control Issue
The data collectors received comprehensive training focusing on interview techniques, questionnaire content, ethical considerations, participant safety, and maintaining confidentiality. The training took the form of a workshop moderated by the principal investigator. During the training session, the questionnaire was clearly explained and subsequently pre-tested. Following this, a pilot study involving 40 Rohingya refugee women was conducted to assess the questionnaire’s understandability and ensure its completeness and consistency in providing the required information. The pilot study participants were excluded from the final analysis.
Variables
Independent Variables
We included following independent variables based on previous literature.28,39–41
Socio-demographic variables: Respondents’ age (continuous), education (1 = yes, 0 = no), and profession (1 = yes, 0 = no).
Internet and radio use: Respondents’ radio listening habits (1 = yes, 0 = no), and Internet use (1 = yes, 0 = no). In the camp, the refugee women can listen to the radio and use the internet on their mobile on a limited scale as they stay inside the camp. Their husbands have access to television as they go outside.
Communication activities: Participation in an STI/HIV awareness program in the camp (1 = yes, 0 = no), discussion with a health worker about STI/HIV issues (1 = yes, 0 = no), visit to a health centre or facility for SRH services (1 = yes, 0 = no), viewing a banner/poster about STI/HIV issues (1 = yes, 0 = no).
Dependent Variable
STI/HIV knowledge among Rohingya refugee women was assessed through 13 items related to STI/HIV transmission, prevention, myths, and misconceptions.
Measurements
Primarily the independent variables had more than two categories and were mostly based on the Likert scale. We recode them as dummy variables as we performed linear regression. The STI/HIV-related items utilized a five-point Likert scale. Positive statements were scored from 1 to 5, ranging from “Extremely Unlikely” to “Extremely Likely,” while negative statements were scored in reverse. The total score for STI/HIV knowledge was obtained by summing the scores for the 13 items. However, due to low frequencies at the scale’s endpoints for the percentage distribution of respondents’ responses regarding STI/HIV, the five scales of items were recoded into three categories.
Reliability of the Items
Internal consistency was also assessed to evaluate reliability, and the scale of STI/HIV knowledge items demonstrated very good internal consistency reliability, with a Cronbach’s Alpha (α) value of 0.88 for this study’s scales.
Statistical Analysis
The respondents’ knowledge of STIs and HIV was analysed using descriptive statistics. A hierarchical regression analysis was conducted to determine the percentage of variation in STI/HIV-related knowledge explained by socio-demographic, media usage, and communication intervention-related factors. Variables with p < .05 in the independent-samples t-test and Pearson correlations were included in the regression models, while multicollinearity was examined. Besides, tolerance and VIF were also checked. The regression model demonstrated good predictive power for the key outcome variables, as indicated by the ANOVA results for total STI/HIV knowledge (F = 41.163, p < .001). Each step’s R2 showed significant changes, and the changes in F were statistically significant (p < .001) as well. SPSS 24.0 was used to conduct these analyses, with statistical significance set at p < .05 for variables in the regression models.
Results
Rohingya Women’s Utilization of Media and Communication-related Activities
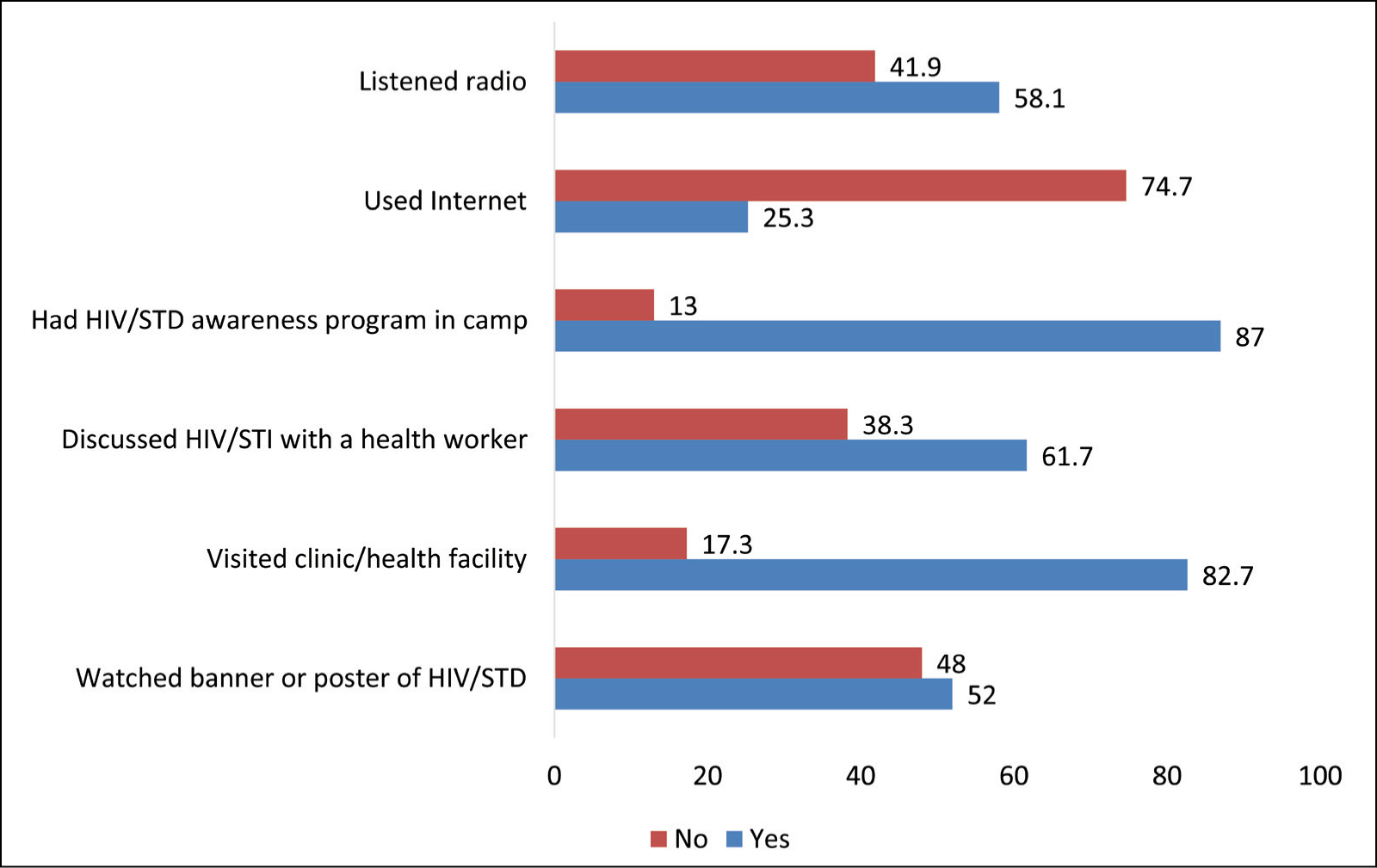
Figure 1 illustrates the respondents’ access to health services and communication interventions. Of the 415 Rohingya refugee women, 58.1% listened to the radio, while one-fourth of the respondents used the Internet. Besides, of the respondents, 87% had an awareness program in the camp, while 61.7% discussed STI/HIV issues with a health worker. Moreover, 82.7% visited a health centre or facility to receive SRH services, whereas more than half (52%) watched a poster or banner about STI/HIV.
Rohingya Refugee Women’s Utilization of Media and Communication-related Activities.
Distribution of Study Participants’ STI/HIV-related Knowledge
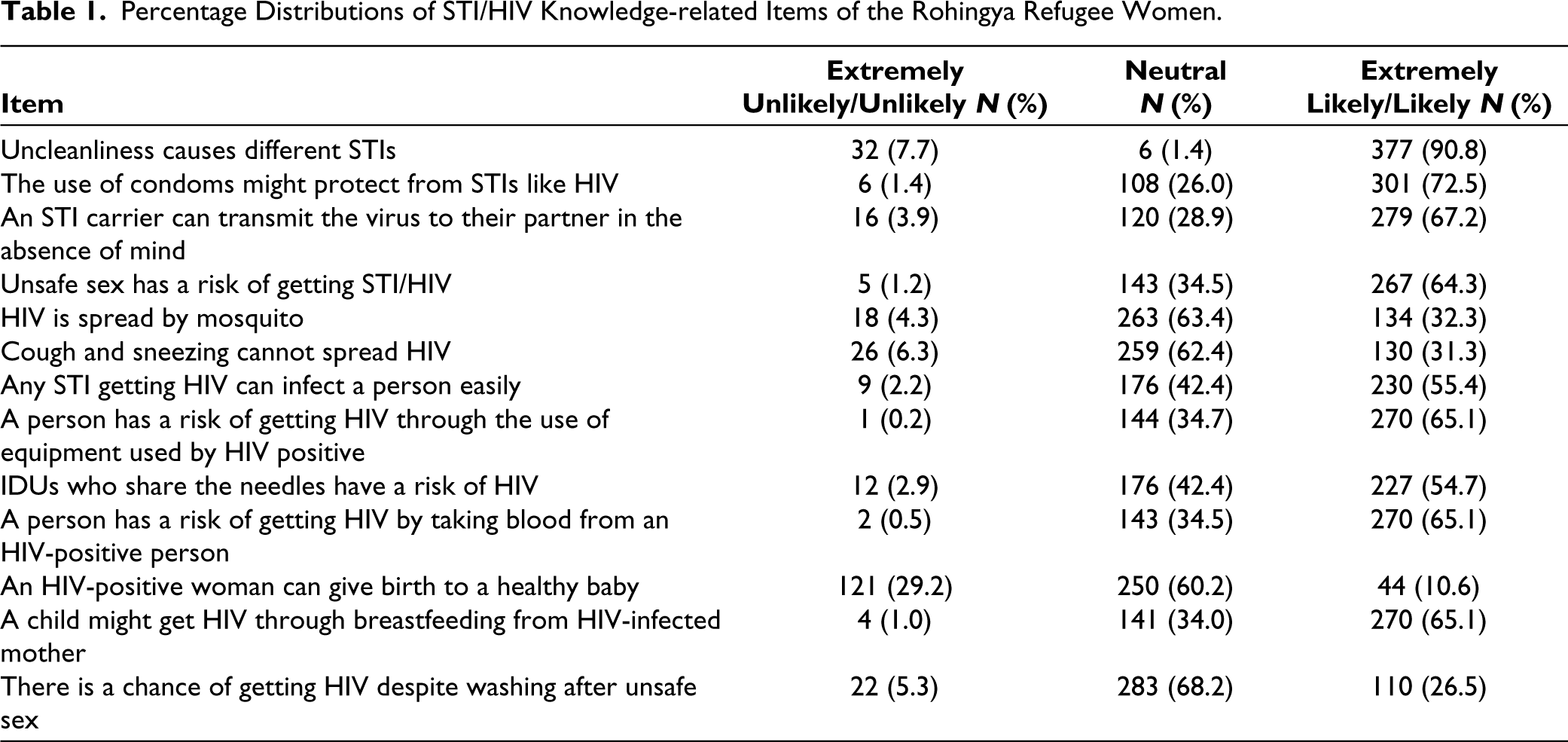
To address the research question, percentage distributions and mean scores of respondents’ STI/HIV knowledge-related items were reported in Tables 1 and 2. Regarding the item, “uncleanliness causes different STIs,” 377 (90.8%) of respondents had accurate knowledge, while the mean score was 4.53 (± 0.91). As to the item “the use of condoms might protect from STIs like HIV,” 301 (72.5%) of the Rohingya women confirmed, and the corresponding mean score was 4.23 (± 0.91). Relating to the item, “an STI carrier can transmit the virus to their partner in the absence of mind,” 279 (67.2%) of them gave an affirmative reply, and the mean score was 3.99 (± 0.96). With regard to the item, “unsafe sex has a risk of getting STI/HIV,” 267 (64.3%) of respondents gave the correct answer, and the mean score was 4.02 (± 0.91).
Percentage Distributions of STI/HIV Knowledge-related Items of the Rohingya Refugee Women.
Descriptive Analysis of STI/HIV Attitude-related Items of the Rohingya Refugee Women.
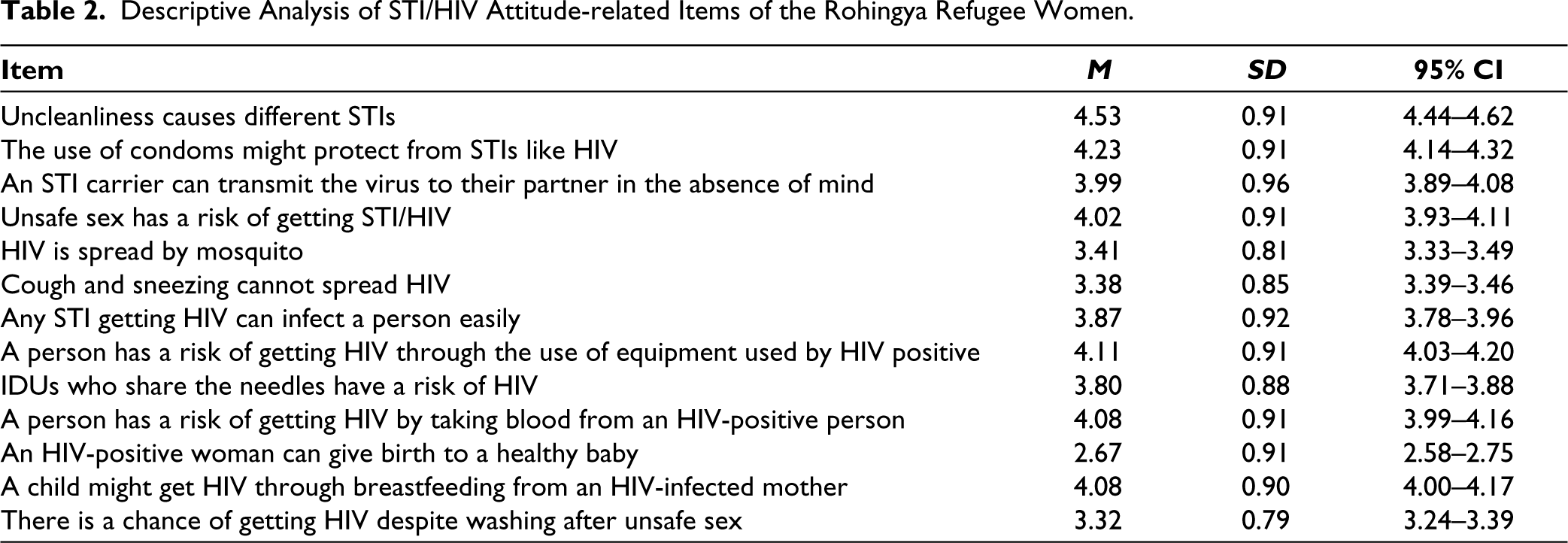
Of the respondents, 263 (63.4%) were neutral about the statement “HIV is spread by mosquito” with a mean score of 3.41 (± 0.81). Pertaining to the item, “cough and sneezing cannot spread HIV,” 259 (62.4%) of the respondents were neutral, and the corresponding mean score was 3.38 (± 0.85). Moreover, 230 (55.4%) of respondents agreed with the statement, “any STI getting HIV can infect a person easily”; the mean score, in this case, was 3.87 (± 0.92). Relating to the item, “a person has a risk of getting HIV through the use of equipment used by HIV positive,” 270 (65.1%) of respondents gave an affirmative reply, while the mean score was 4.11 (± 0.91).
Regarding the item, “IDUs who share the needles have a risk of HIV,” 227 (54.7%) of the Rohingya women agreed, and the mean score was 3.80 (± 0.88). Furthermore, 270 (65.1%) of the Rohingya refugee women agreed with the statement “a person has a risk of getting HIV by taking blood from an HIV-positive person” with a mean score of 4.08 (± 0.91). Regarding the item “an HIV-positive woman can give birth to a healthy baby,” 250 (60.2%) of the Rohingya women confirmed, and the corresponding mean score was 2.67 (± 0.91). Relating to the item, “a child might get HIV through breastfeeding from HIV infected mother,” 270 (65.1%) of them gave an affirmative reply, and the mean score was 4.08 (± 0.90). About the item, “there is a chance of getting HIV despite washing after unsafe sex,” 283 (68.2%) of respondents gave the correct answer, and the mean score was 3.32 (± 0.79).
Bivariate Relationship Between Rohingya Women’s STI/HIV Knowledge by Demographic, and Communication Activities
To test the hypotheses, we conducted the independent-samples t-test (two-tailed) for categorical variable and Pearson correlation (two-tailed) for continuous variables exploring the relationship between respondents’ STI/HIV-related knowledge by the respondents’ socio-demographic factors, utilization of media and communication program. Table 3 demonstrates the respondents having education (M = 51.95, SD = 7.14) had a better STI/HIV knowledge score than the respondents with no education (M = 47.25, SD = 6.99, t = 6.78, p < .001). In addition, a significant difference was found in STI/HIV knowledge score for the respondents who were professional (M = 54.95, SD = 6.02) and who were housewives (M = 48.01, SD = 7.09, t = 9.24, p < .001). Pearson correlation found a significant negative relationship between respondents’ STI/HIV knowledge score and the age of respondents (r = –0.22, p < .001).
Socio-demographic, Media and Communication-related predictors of STI/HIV Knowledge Among the Rohingya Refugee Women in Bivariate Analysis.
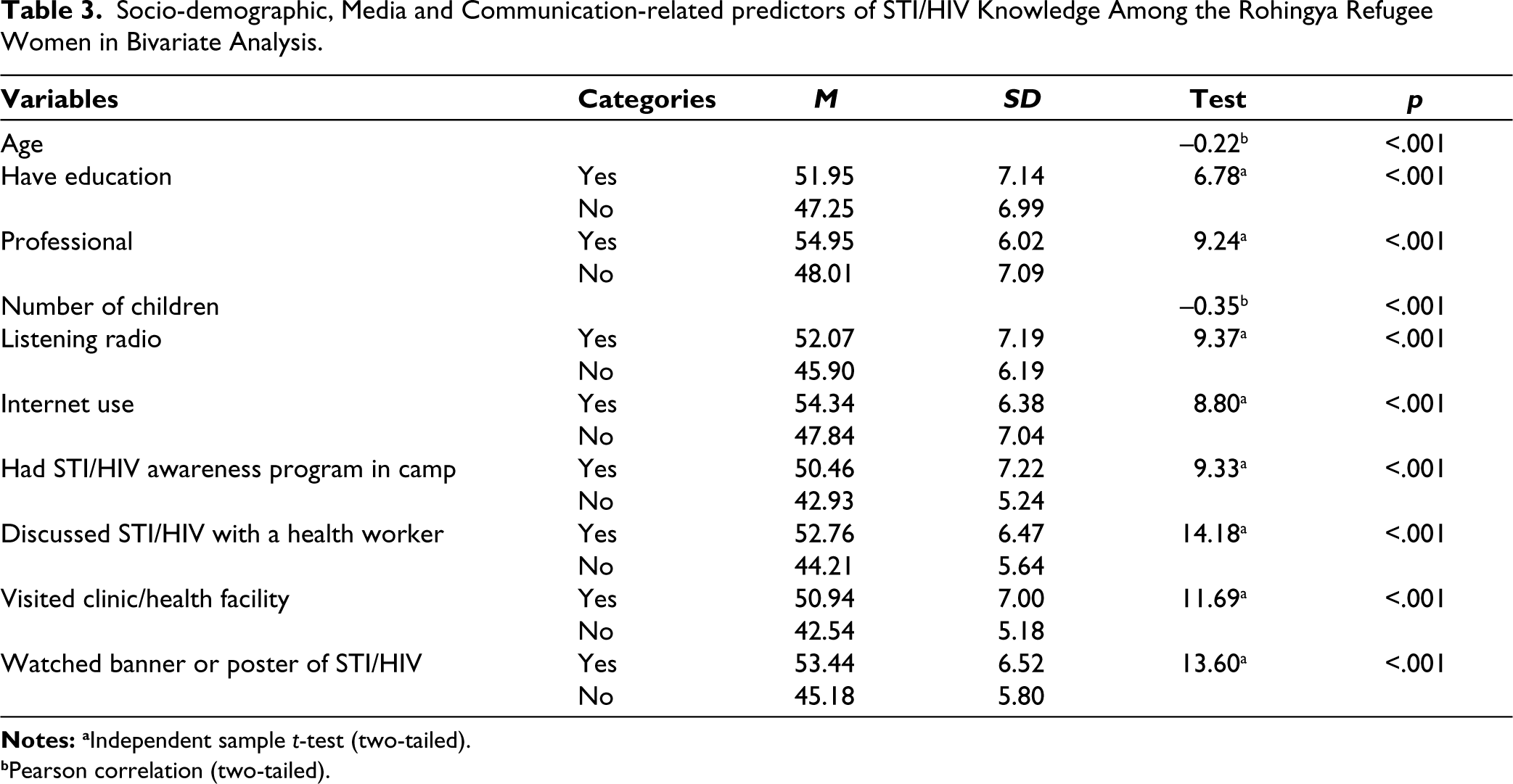
Besides, there was a significant difference in STI/HIV knowledge score between the respondents who listened to the radio (M = 52.07, SD = 7.19) and those who did not listen (M = 45.90, SD = 6.19, t = 9.37, p < .001). In addition, a significant difference was found in the STI/HIV knowledge score between the respondents who used the Internet (M = 54.34, SD = 6.38) and those who did not use it (M = 47.84, SD = 7.04, t = 8.80, p < .001).
The study findings depict that there was also a significant difference in STI/HIV knowledge score between the respondents who had an STI/HIV awareness program in camp (M = 50.46, SD = 7.22) and who did not have (M = 42.93, SD = 5.24; t = 9.33, p < .001). In addition, the respondents who ever discussed STI/HIV with a health worker (M = 52.76, SD = 6.47) had higher STI/HIV knowledge scores than those who did not participate (M = 44.21, SD = 5.64, t = 14.18, p < .001).
Besides, there was a statistically significant difference in STI/HIV knowledge score for the respondents who ever visited a clinic/health facility (M = 50.94, SD = 7.00) and who did not go to any clinic (M = 42.54, SD = 5.18, t = 11.69, p < .001). This study also found a statistically significant difference in STI/HIV knowledge score for the respondents who watched banner or poster of STI/HIV (M = 53.44, SD = 6.52) and who did not watch (M = 45.18, SD = 5.80; t = 13.60, p < .001).
Hierarchical Regression for Variables Predicting Respondents’ Good STI/HIV Knowledge
The model summary for good STI/HIV knowledge among Rohingya women is shown in Table 4. In addition, Table 5 provides the analysis of variance and the coefficients. The hierarchical multiple regression as shown in Tables 4 and 5, reveals that in Model 1, all three characteristics of respondents’ STI/HIV knowledge, age (β = –0.14, t = –3.08, p = .002), having education (β = 0.14, t = 2.78, p = .006), and being professional (β = 0.30, t = 5.79, p < .001) contributed significantly to the regression model (F = 31.57, df = 3/411, p < .001) and accounted for 18% variations in good STI/HIV knowledge among the respondents.
Regression Model Summary for the Predictors of STI/HIV Knowledge Among the Rohingya Refugee Women.

Hierarchical Regression Depicting Factors of Good STI/HIV Knowledge Among the Rohingya Refugee Women.
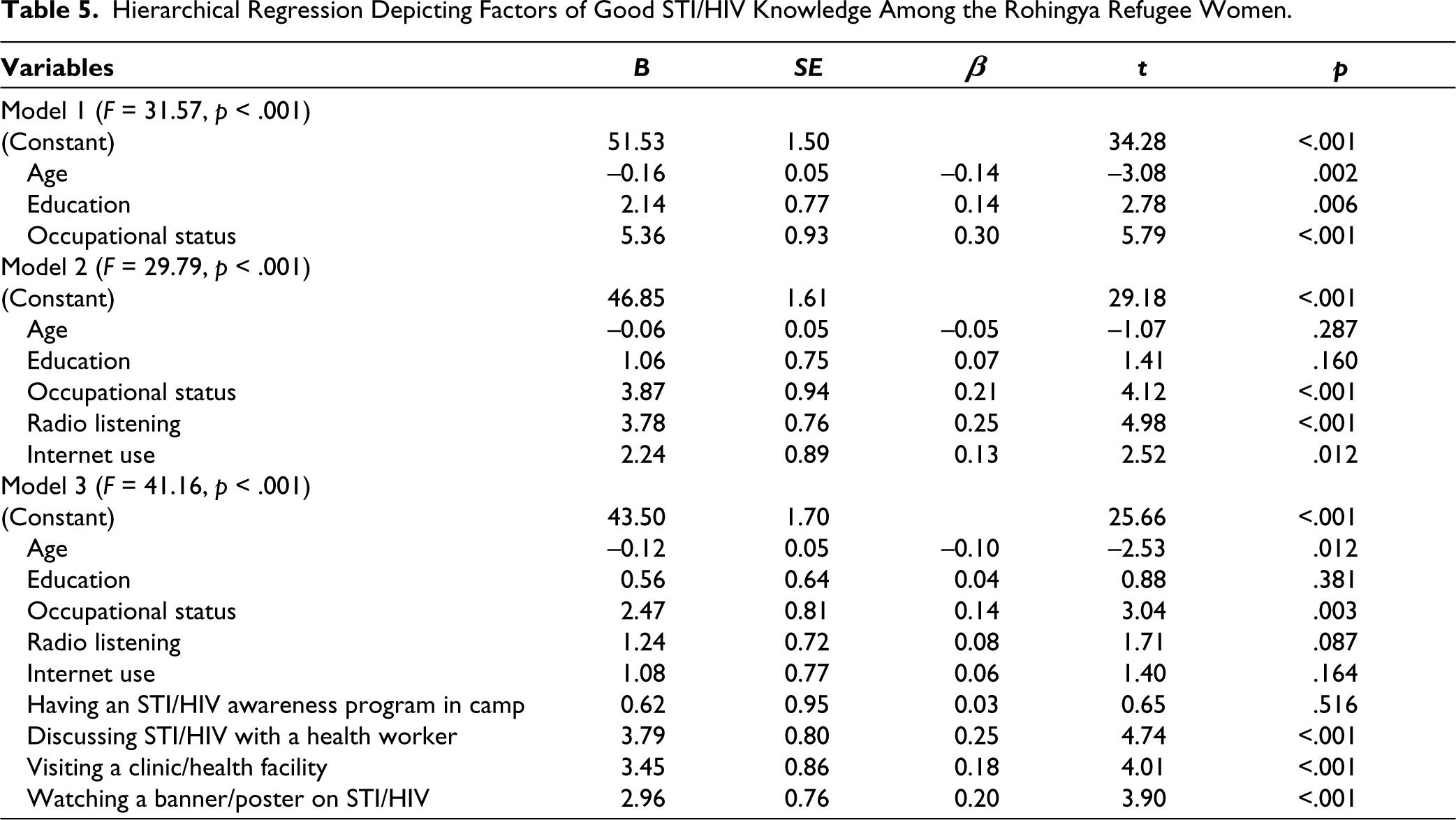
Adding the other two predictors in Model 2, explained an additional 8% variation in good STI/HIV knowledge above and beyond the effects of the predictors in Model 1. In Model 2, among the five predictors of respondents’ good STI/HIV knowledge, being professional (β = 0.21, t = 4.12, p < .001), listening to the radio (β = 0.25, t = 4.98, p < .001) and Internet use (β = 0.13, t = 2.52, p = .012) contributed significantly to the regression model (F = 29.79, df = 2/409, p < .001) and accounted for 26% variations in good STI/HIV knowledge among the respondents.
Introducing the other four predictors in Model 3, explained an additional 21% variation in good STI/HIV knowledge above and beyond the effects of the predictors in Model 2. In Model 3, among the nine predictors of respondents’ good STI/HIV knowledge, being professional (β = 0.14, t = 3.04, p = .003), discussion of STI/HIV with a health worker (β = 0.25, t = 4.74, p < .001), visiting clinic/health facility (β = 0.18, t = 4.01, p < .001), watching banner/poster on STI/HIV (β = 0.20, t = 3.90, p < .001) contributed significantly to the regression model (F = 41.16, df = 4/405, p < .001) and accounted for 47% variations in good STI/HIV knowledge among the respondents.
Findings of bivariate analyses and R2 Δ in different hierarchical regression models supported all our hypotheses. In contrast, the final model of hierarchical regression suggests that being professional among the socio-demographic variables and discussing STI/HIV with a health worker, visiting a clinic/health facility, and watching banners/posters on STI/HIV were reported as the significant predictor of STI/HIV knowledge among refugee women.
Discussion
A cohort of Rohingya refugee women exhibits a lack of accurate knowledge regarding STI/HIV-related myths and misconceptions, which can impede their adoption of appropriate preventive measures. This finding is similar to previous studies.29–32 For instance, approximately two-thirds of the participants have no knowledge about whether HIV can be transmitted through mosquitoes, coughing and sneezing, the possibility of an HIV-positive woman giving birth to a healthy baby, the efficacy of washing after unsafe sex in preventing infection, and the ease of HIV infection in individuals already affected by an STI.
Our findings revealed that the higher socioeconomic status of the study participants, such as having education, professional status and internet use appeared as the predictors of HIV/STI knowledge which is in line with other studies.38,40,41
This study also aimed to examine the relative predictive strength of socio-demographic factors, media use-related factors, and utilization of communication activities-related variables in determining STI/HIV knowledge among Rohingya refugee women. The R2 value indicated that the utilization of communication activities emerged as a stronger predictor of good STI/HIV knowledge compared to socio-demographic variables. When comparing R2 values across different models predicting STI/HIV knowledge, a significant improvement was observed with the respondents’ utilization of communication activities, followed by socio-demographic and media use-related variables. This result is consistent with a previous study conducted in the same setting. 28
Furthermore, the utilization of various communication-related activities by the refugee women, such as discussing with health workers, observing banners and posters, and visiting health facilities, emerged as the most influential predictors. Communication is recognized as a crucial strategy for enhancing knowledge and understanding of health-related issues, including STI/HIV. 43 Existing literature suggests that communication can shape positive perceptions and beliefs regarding SRH issues. 49 Globally, health communication, including health education, has proven to be an effective approach in promoting behavioral changes among large-scale target audiences concerning specific problems. 50
The findings of this investigation hold significant contributions with broad-reaching consequences. By examining the status of STI/HIV knowledge among Rohingya women, this study enhances our understanding, as well as that of policymakers and administrators. It will facilitate the design of appropriate communication programs, campaigns, and the development of effective communication materials to prevent STIs within this vulnerable community. Given the challenging socioeconomic conditions faced by the Rohingya, this study suggests focusing on improving communication interventions using behavioral change theories and strategic communication approaches. Such efforts can lead to a more efficient and effective distribution of resources from government bodies (GOB), non-governmental organizations (NGOs), and international non-governmental organizations (INGOs).
Conclusion
The findings highlight the significant impact of communication activities on the STI/HIV knowledge of refugee women, emphasizing that greater utilization of communication activities is associated with higher levels of knowledge. Consequently, the utilization of communication activities by Rohingya women emerges as a stronger predictor of STI/HIV knowledge than socioeconomic variables. Interpersonal communication with health workers, observing banners and posters, and visiting healthcare facilities were particularly influential factors.
This study has several limitations that should be acknowledged. First, the data collected may have been influenced by social desirability bias, potentially impacting the validity of the outcomes. Second, gathering fully representative data on sensitive topics like STIs is inherently challenging. Additionally, the logistical challenges were exacerbated by the distances between different blocks where data collection occurred simultaneously. Due to financial constraints, the study data were obtained from only one camp. Besides, convenience sampling technique to select the study participants is also a limitation of the study. Besides, we used items to assess the knowledge that was not validated. The oversimplification in the categorization of the variables is also a drawback of the study.
To address the potential social desirability bias, further qualitative research is recommended to gain deeper insights into the effectiveness of communication activities regarding STI/HIV issues among Rohingya refugees and to inform policy decisions. Empirical research should also be conducted to gain a better understanding of the demographic characteristics, culture, needs, and demands of the refugee population.
Implications in a Global Context and for International Audiences
The study has some implications in a global context and for international audiences. Such as, it underscores that displaced and refugee populations, like the Rohingyas, may have significant gaps in essential health knowledge. This finding can be extrapolated to other refugee groups, indicating a larger global challenge that requires attention. Our results emphasize the need for health campaigns tailored to specific demographics within refugee populations. International health agencies can take cues from such research to design targeted interventions, rather than one-size-fits-all solutions. The prominence of certain communication activities, such as discussions with healthcare workers or observing banners/posters, in influencing knowledge implies that effective communication channels are crucial. For international audiences, this could mean reassessing and redirecting resources to the most impactful communication strategies. The findings underscore the broader issue of health equity, suggesting that displaced populations lag in essential knowledge, placing them at increased risk. This aligns with global discussions on health rights, social justice, and the need to ensure health knowledge and resources are accessible to all, regardless of their circumstances.
Footnotes
Abbreviations
ANOVA: Analysis of variance; df: Degree of Freedom; GOB: Government of Bangladesh; HIV: Human Immunodeficiency Virus; IAWG: Inter-Agency Working Group; INGO: International Non-Government Organization; IOM: International Organization for Migration; ISCG: Inter Sector Coordination Group; NGO: Non-governmental organization; SD: Standard deviation; SE: Standard Error; SPSS: Statistical Package for Social Sciences; SRH: Sexual and Reproductive Health; STI: Sexually Transmitted Infection; UNHCR: United Nations High Commissioner for Refugees; WRC: Women’s Refugee Commission.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Participant Consent
The university’s Ethical Review Board gave ethical approval for the study (reference number: CU SOC-21-0002). Participants signed or thumb-stamped a permission form to indicate their written informed agreement to participate.
Funding
This study used data from a research project supported by the University of Chittagong, Bangladesh [246(17)/POU/7-37(8)/2ND-2019].
Informed Consent
An informed consent was obtained from each participant.