
Abstract
Vaginismus is described as an involuntary pelvic muscular spasm that occurs due to “fear of pain” associated with vaginal penetration which prevents a woman from experiencing penovaginal sexual intercourse despite her wish to do so. In the context of heterosexual couples with subfertility, untreated vaginismus may result in unconsummated marriage and/or reduced quality of sex life and/or can affect a woman’s perception about her potential of femininity and motherhood. Though vaginismus is an easily diagnosable and treatable condition in many instances, it often gets ignored or inadequately/inappropriately managed. There is paucity of practice-informed clinical data on management of vaginismus in couples with subfertility that is contextualized to the Indian setting. The present viewpoint is based on real-world clinical scenarios who presented as couples to a tertiary fertility center with unconsummated marriage as their chief complaint. The intent of this viewpoint is not only to highlight the common pitfalls in the management of vaginismus but also showcase a clinically proven interdisciplinary management approach for assessment and management of vaginismus and any associated sexual problems.
Introduction
Vaginismus, prior to the release of Diagnostic and Statistical Manual, Fifth Edition (DSM-V), was defined as recurrent or persistent involuntary spams of the musculature of the outer third of vagina which interfere with coitus and cause distress and interpersonal difficulty. In DSM-V, 1 vaginismus and dyspareunia are included as part of genitopelvic pain penetration disorder (GPPPD) characterized by persistent or recurrent difficulties with 1 (or more) of the following: vaginal penetration during intercourse; marked vulvovaginal or pelvic pain during vaginal intercourse or penetration attempts; marked fear or anxiety about vulvovaginal or pelvic pain in anticipation of, during, or as a result of vaginal penetration; or marked tensing or tightening of the pelvic floor muscles during attempted vaginal penetration. 2 GPPPD, according to DSM-V, is classified as either lifelong (the disturbance has been present since the individual became sexually active) or acquired (disturbance began after a period of relatively normal sexual function). Further, GPPPD is classified as mild, moderate, or severe based on the distress over the symptoms and not on the severity of the symptoms per se. Though GPPD is the technically correct terminology, the authors have decided to use “vaginismus” throughout this article for ease of readers’ understanding. Vaginismus is still a popular clinical term.
In women with vaginismus, attempted vaginal penetration of any sort (such as with a tampon, gynecological vaginal examination, transvaginal ultrasound, or sexual intercourse) provokes involuntary pelvic muscular spasms which are the physical components of the condition. 3 In addition, vaginismus also has psychosocial and interpersonal components (fear, anxiety, depression, shame, embarrassment, self-image, and relationship difficulties). 4 Some common predisposing factors in the presentation of lifelong vaginismus are poor sexual health literacy, guilt about sexual pleasure, highly restrictive values-based sexual scripts, and childhood sexual violation/abuse 5 whereas untreated local organic pathologies and ongoing relationship conflicts have been postulated to be important perpetuating factors of vaginismus. 6 Often, vaginismus comanifests with a wide range of concerns relating to general, relational, and psychosexual well-being. 7
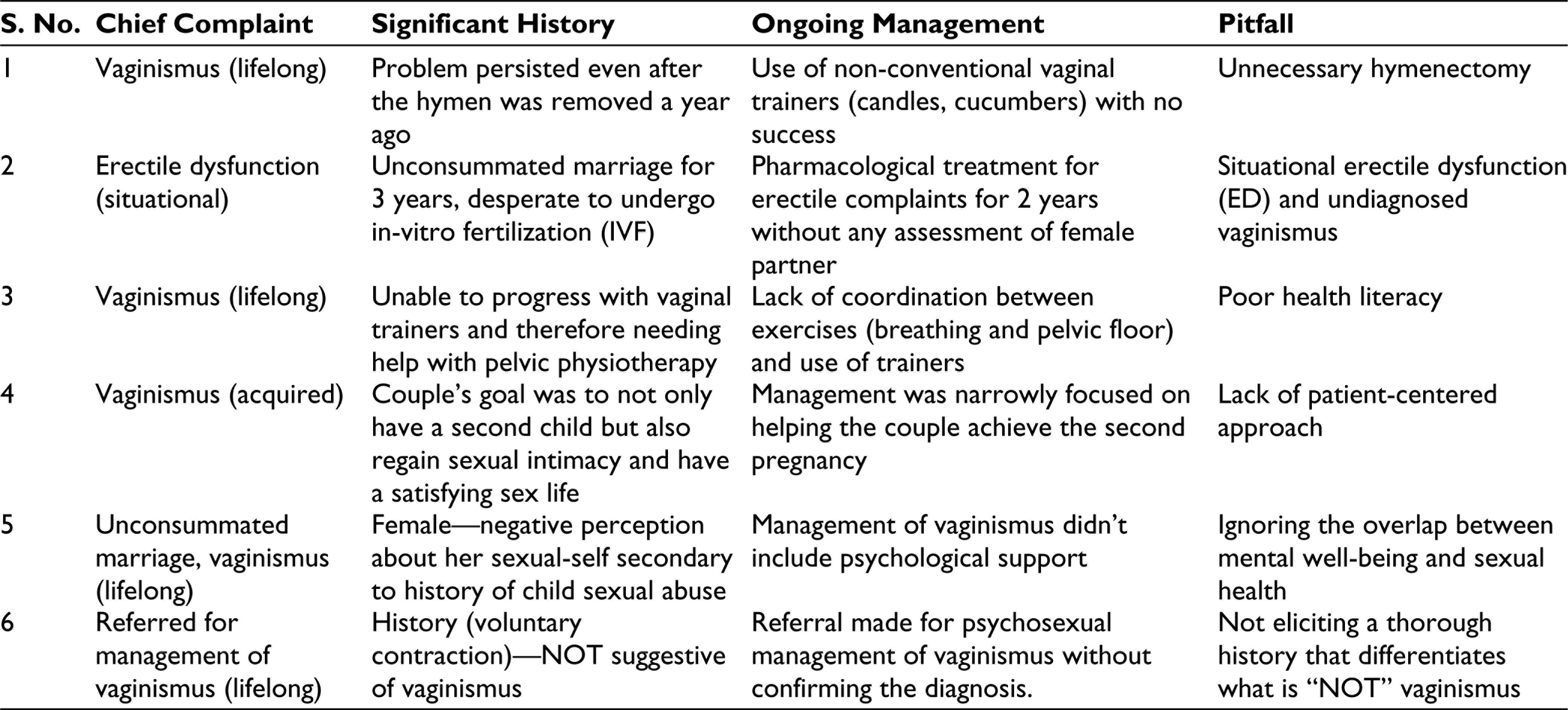
Some Pitfalls in the Management of Vaginismus
Six common pitfalls in the management of vaginismus are presented in Table 1 based on the insights derived from real clinical scenarios managed at a tertiary fertility center in a cosmopolitan city of Southern India.
Management of Vaginismus
There is paucity of evidence in favor of a specific management option for vaginismus7, 8 and a recent (2018) meta-analysis concluded that women with vaginismus benefit from a range of treatments in majority of cases. 9 Multifaceted and interdisciplinary approach to painful sex disorders could lead to successful management outcomes (pain and intercourse). 10 Anecdotal evidence (interaction with numerous gynecologists/fertility specialists) suggests a need for practical and Indian context-specific guidance to best manage women with vaginismus. The management guide presented here is not meant to be one-size-fit-all as it has been developed based on clinical experience managing women/couples with subfertility, presenting to a tertiary fertility center that has in-house access to a team of expert multidisciplinary health-care professionals. Botulinum toxin has been found useful in some patients with vaginismus, particularly in treatment-resistant cases 11 but this modality is not readily available in the setting where the authors practice and therefore not discussed.
Common Pitfalls in the Management of Vaginismus
Diagnostic Workup
Diagnosis of vaginismus can be complex due to its potential multifactorial etiology and certainly requires more than 1 or 2 questions about pain or difficulty with penetration. A rushed approach can result in overdiagnosis of vaginismus (as described in pitfall 6) which can have negative psycho-socio-sexual impacts for the woman, couple, and extended family. 12 Instead, diagnosis of vaginismus is best achieved by ruling out all common/possible causes for genitopelvic pain and/or difficulty with vaginal penetration.
Two critical issues that need diligence and caution when eliciting history are: (a) differentiating “fear of pain” from “actual realized pain” and eliciting which came first is crucial, followed by (b) assessing whether there is an involuntary element to the cascade of symptoms (fear of pain, pain, pelvic floor muscle tightening, and difficulty with penetration).
Some basic counselling skills (granting permission to a woman/couple to express their true concerns, active listening, demonstrating empathy (not sympathy), and remaining nonjudgmental) are highly vital in the initial phase of history-taking as it is very likely that it’s the first-time ever a woman/couple is expressing their true (sexual) issues to anyone. In women with vaginismus, digital or ultrasound examination of the vagina is often not possible nor required. It is important to bear in mind that any forceful attempt of vaginal examination can interfere with trust between a patient and treating gynecologist which in-turn can lead to disengagement from management. A general pelvic and vulval examination performed by a gynecologist in a highly supportive manner is encouraged. During such examination, a gynecologist can elicit a woman’s understanding of her own genitalia, clarify any doubts that a woman has about her genital anatomy, check for any signs of infection/inflammation in the external genitalia, and show her where the pelvic floor muscles are in the body and explain the role it plays in causing pain and difficulty with penetration.
Irrespective of the socioeconomic and educational status, it is critical to ensure that the couple is attempting intercourse in the right orifice and provide basic sex education, as necessary. Men are often excluded from being present with their sexual partners in the gynecology examination room. In the author’s view, with due consent of the woman being examined, having her male sexual partner present can provide an invaluable opportunity for the man and the couple to gain basic education on sexual anatomy relevant to vaginal intercourse. It is best practice, provided the treating health-care professionals are reasonably aware and trained, to combine history-taking, assessment, and patient education as the 3 components are complementary and have the potential to result in better patient outcomes when performed skillfully.
A recent (2019) systematic review of outcomes across various treatment modalities for female sexual dysfunction summarized that nonpharmacological interventions (self-performed vaginal penetration exercises with object introduced by therapists and pelvic floor rehabilitation) have successful desired treatment outcome of penovaginal intercourse ability (50–90%). 13 Best practice in the management of vaginismus, after exclusion of gynecological or any organic causes, encompasses pelvic floor physiotherapy, vaginal trainers, and psychosexual counselling/therapy.3, 13 Presence of underlying mental health conditions (eg, anxiety disorder, phobic disorder) requires appropriate referral to the mental health team (psychiatrists and/or psychologists) as highlighted in pitfall 5. A good interdisciplinary diagnostic workup for vaginismus can prevent/delay unwanted surgical procedures (as in pitfall 1) or the need for sophisticated artificial reproductive techniques (as in pitfall 2).
Pelvic Floor Physiotherapy
Sexual response is one of the key functions of pelvic floor muscles in addition to support, stabilization, sphincteric control, and lymphatic drainage. 14 Women with vaginismus, in comparison to dyspareunia, demonstrate significantly higher pelvic muscle tone and lower muscles strength. 15 The role of a pelvic floor-trained physiotherapist is of paramount importance because vaginismus involves varying degrees of powerful involuntary pelvic floor muscle contractions associated with pain which in turn results in anticipation of pain in future sexual intercourse attempts. 16 Helping a woman understand this physiological process and supporting them in breaking the vicious cycle of “fear-of-pain, involuntary contraction, and pain” is at the crux of successfully managing vaginismus. Pelvic floor physiotherapy in women with vaginismus involves 4 distinct aspects (assessment, patient education, breathing +/−pelvic floor exercise, and the use of vaginal trainers). After the initial assessment with the woman on her own, the following sessions are open for her to attend alone or as a couple. Patient feedback data indicates that daily scheduling of physiotherapy sessions (for about 7–10 days) seems to boost confidence and develop necessary skills to use vaginal trainers in a coordinated manner with pelvic and breathing exercises.
A. Assessment
The pelvic floor muscle assessment starts with eliciting the pain history using the Visual Analogue Scale, 17 followed by pelvic examination performed in a comfortable position (supine with knees bent). Vulval region is inspected for any signs of urinary tract infection and skin abnormality. Appropriate referral to GP, urologist, or gynae dermatologist may be required for treatment. Anecdotally, most women with vaginismus require considerable amount of time to be assessed. Enabling confidence in the patient that “it won’t hurt” and carrying out the assessment in a gentle manner with adequate explanation of each step is highly critical. Static observation includes skin condition, symmetry of tissue positions, redness, and so on. Dynamic observation includes contraction and relaxation of pelvic floor muscle and perineal lift and release and observation of pelvic floor muscles during coughing. Sensation test is done with the help of cotton bud over the pubic symphysis, labia majora and minora, vestibular area, and at sides of vaginal opening. A comprehensive physical assessment of pelvic and hip muscles was completed and strength was measured using the Modified Oxford Scale. 18
B. Education and Exercises
Educating a woman/couple about the pelvic floor muscles and their anatomical function during sexual intercourse and the invoked hypertonic response with vaginismus is critical. Anecdotally, explaining the response using a metaphor (involuntary closure of eyelids when a pencil is moved toward the eye) can help women/couples to quickly understand the protective reasoning behind involuntary contraction of pelvic floor muscles.
Combining benefits such as possible prevention or amelioration of urinary incontinence, better orgasms, and control during vaginal penetration may motivate women to maintain doing their pelvic floor exercises for their lifetime.
Combining pelvic floor exercise with simple diaphragmatic breathing and progressive relaxation exercises maximizes managing women with vaginismus. 19
C. Correct Use of Vaginal Trainers
The term vaginal “trainers,” 19 instead of “dilators,” sends a positive message to the woman that they are not dilating but only learning how to use their pelvic floor and vagina with penovaginal penetration. Vaginal trainers are most helpful with appropriate support and education. Use of unconventional vaginal trainers (pitfall 1) and lack of guidance trainers was the key barrier highlighted in pitfalls 1 and 3. Guidance on appropriate insertion of the trainers, that is, educating about coordinated pelvic floor and breathing exercises while inserting the trainers, so that insertion occurs only during relaxation is pivotal to good progress. Another factor is that if discomfort occurs then all movement in or out of the vagina stops till the sensation abates. Learning correct diaphragmatic breathing and pelvic floor exercises comes before vaginal penetration attempts. It’s important to get the woman to explore her vaginal opening with her finger before any insertion attempts so she gets a proprioceptive understanding of where she is going to insert the trainers. The female physiotherapist assists the woman to gently introduce a well-lubricated smallest size vaginal “trainer 1” into the vagina during exhalation phase of breathing which gives maximal relaxation of pelvic floor muscles. A couple of supervised attempts of self-practice of insertion is encouraged but not imposed. Too much of self-practice at the beginning has the risk of building aversion, if the experience is too unpleasant or stressful. The woman is encouraged, provided she is agreeable, to continue the same at-home with short frequent attempts better than infrequent longer sessions. At the next visit, if sufficient progress has been made with “trainer 1”, “trainer 2” is introduced in the same way and so on until “trainer 6”. The vaginal trainers are advised to be practiced for 2 to 3 months to help build adequate confidence. Adequate lubrication is advised/reminded to avoid any irritation. It is important to treat the couple as a single unit to alleviate pressure on any one person and avoid misunderstanding between the couple. The male partner is encouraged to be actively engaged during training and to assist and motivate the female partner during her vaginal dilator practice. Affection, cuddling, and kissing prior to vaginal exercises help natural arousal and good feeling in the sessions.
Transitioning from vaginal trainers to penovaginal penetration is a big step. Women are encouraged to be quite comfortable with “trainer 5 or 6” (depending on partner’s penis size) before attempting penovaginal penetration. Pivotal to this transition phase is that the women feel that they are in control of the insertion. Couples are encouraged to have 20 to 30 min of foreplay, at a time when both are not tired and are not likely to be disturbed, that is, privacy, subtle lighting to help with activity and possibly the woman in a “ woman on top position” or perhaps straddling a sitting partner. In these 2 positions, the woman can hold the erect penis and guide it inside the vagina mimicking use of the trainer. The woman can control the speed and depth of penetration and rest in between according to her needs.
The couple, especially the men, are taught to be assertive, not aggressive, in the process of penis insertion and more importantly not to be judgmental if the penis insertion does not happen on the first attempt. The angle of penetration needs to be discussed and accommodations made for a small or large penis. The couples are advised to have penile penetration every 2 to 3 days on a regular basis so that the learning process is cemented. If there is a regression, the advice is to go back to a smaller trainer and quickly go through the steps again building confidence and sense of control.
Psychosexual Education and Counselling/Therapy
Psychosexual education and counselling, either offered to a couple or individually to a woman (if needed), has been demonstrated to play a significant role in the treatment outcome of vaginismus.10, 20–22 It is common for couples to seek help for unconsummated marriage with a primary complaint of situational erectile dysfunction (ED). Upon eliciting a thorough sexual history of both partners, it is not uncommon for both individuals to have a sexual difficulty, sometimes having a protective component and sometimes as a precursor to the other partner’s difficulty. Contraction of the pelvic floor muscles can act like a brick wall preventing penetration which in turn can result in ED and/or premature ejaculation as the man loses confidence or becomes scared of hurting his female sexual partner. This can lead to blame, anger, sexual avoidance, and marital disharmony.
A nonjudgmental sexual history must be elicited from both the partners if correct treatment is to be given for the correct problem. Providing space and time for the women/men/couple is important to voice her/his/their true concern. It is this approach that made the clinicians become aware that the primary problem in pitfall 6 was not vaginismus and the couple’s primary goal (in pitfall 4) was to have a satisfying sex life and not primarily vaginal penetration. It’s important to bring in that intercourse may be a primary goal for pregnancy, but sexual intimacy may also be a legitimate goal and need different approaches. It is best not to assume that every couple’s goal is to have another child simply because they present to a fertility hospital. Every couple, irrespective of their demographic background, should be assessed for their awareness and knowledge about sexual functioning and be offered basic psychosexual education. Preexisting (prior to the presenting situational ED secondary to vaginismus) sexual problem(s) identified in either need to be appropriately managed. It is important to manage the clinical triad (unconsummated marriage, situational ED, and vaginismus) as a “couple” problem to avoid risk of creating marital disharmony. Often, sex is reduced to “intercourse” in couples with unconsummated marriage and achieving penetration has become the primary, if not the only, goal in their life. Encouraging couples to redefine the meaning they attach to sex (ie, sex is not just about intercourse) and supporting them to widen the sexual schema (ie, engage in pleasurable, mutually consenting, outercourse activities together) while continuing working on their goal of successful intercourse can help the couple (re)build sexual intimacy which may have long been avoided.
Conclusion
In India, lack of public awareness about vaginismus coupled with shame and fear of judgment makes it exceedingly difficult for many women/couples with subfertility to seek help directly for vaginismus. Etiologic factors are spread across various health disciplines and therefore an interdisciplinary approach is at the core of best practice management of vaginismus. A thorough sexual history and assessment, educating and empowering women/couples, dedicated support of a pelvic floor physiotherapist, correct use of vaginal trainers, and psychosexual counselling/therapy (if needed) forms the core aspects of management of vaginismus. Clinical data shows that a systematic and interdisciplinary approach to management of vaginismus has a potential for high success rate. This viewpoint article presents some common pitfalls using clinical cases that are highly representative of the most common clinical presentations within tertiary fertility care settings in India.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.