Culture-bound syndromes (CBS) have been a subject under remarkable criticism since many decades. Many pertaining and persisting issues associated with CBS have been in several controversies that time and again stir up debates among Western and non-Western researchers. In this regard, we have tried to summarize the major critiques in this area.
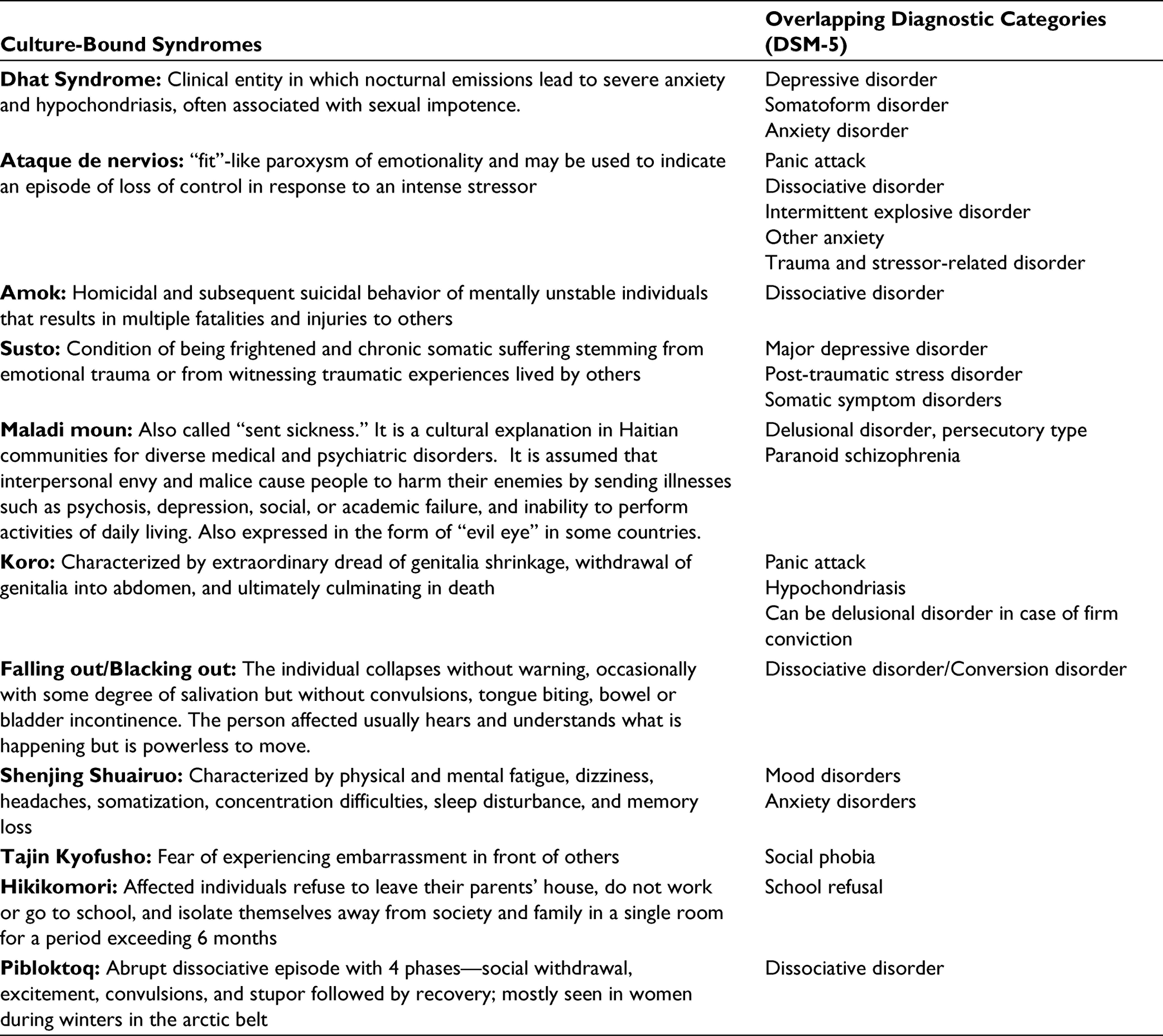
Issues over the diagnostic overlap of CBS with existing psychiatric disorders: The most striking critique of CBS is that the symptomatology often overlaps with the symptomatology of the existing psychiatric disorders, which often ignites the fire of controversy. For instance, several studies had tried to highlight the diagnostic overlap between common CBS disorders and common mental disorders (see Table 1). In this regard, the major chunk of controversy hovers around the Dhat syndrome. From the time of its inception and description by Prof NN Wig,1 there have been several studies which had tried to establish the syndrome to be either a subtype of depressive spectrum2, 3 or somatoform spectrum4 (as the patients predominately present with depressive and multiple somatic symptoms attributing from “semen loss”). However, the point to note is that authors have not attempted to clarify if the reported symptoms could be attributed to a comorbid depressive disorder.2 The psychological distress or “idioms of distress” related to loss of semen (Dhat) may be responsible for high rates of depression or somatic symptoms. Therefore, we conclude that although there is no actual strong evidence supporting Dhat syndrome to be a depressive or somatoform disorder entity per se, yet the possibility cannot be entirely ruled out. More robust studies, mainly focusing on the cultural beliefs, symptom attributions, and phenomenology, can enlighten this area. Similar issues can be debated for Ataque de nervois (Latin American) vis-à-vis panic disorder, Hwabyung (Korea), Neurasthenia (China) with depression, and Taijin-kyofusho (Japan) with social phobia and many more (Table 1).5
Unclear boundaries and different explanations of CBS by different researchers: The criteria of classification of the CBS group of disorders had changed over time due to differences in theoretical views and meaning of the phenomena rather than due to the natural changes of the disorder/s consideration.7 Kraepelin had reported that different cultures do not give rise to different psychiatric disorders but modify their phenomenology and this holds true till date. However, identifying predominance of symptoms has been found to be a problematic issue. For example, Bernstein and Gaw considered “Koro” as a somatoform disorder, whereas Levine and Gaw deemed “Koro” to be an anxiety disorder.8 This deliberation is disputable because “Koro” encompasses symptoms from dissociative, sexual, anxiety, and somatoform disorders. Thus, grouping of “predominant” symptoms has not decisively solved the classification problem due to unclear boundaries of diverse presentation. Similarly, in case of “Latah,” while a group of researchers presented a psychobiological explanation stating that the predominant feature of “Latah” is a neurophysiological startle reflex, another group of researchers opposed the same and argued that difficult social situation of being an older woman of childbearing age and its violations of Malaysian norms of self-control and courtesy being the main explanation behind origin of “Latah”.8 Therefore, there lies the complexities of inconsistencies in different explanations as well as unclear boundaries to fit the different CBS in the current ambit of known diagnostic systems.9
Culture-Bound Syndromes and Their Overlap With DSM-5 Diagnosis6
Culture-Bound Syndromes
Overlapping Diagnostic Categories (DSM-5)
Dhat Syndrome: Clinical entity in which nocturnal emissions lead to severe anxiety and hypochondriasis, often associated with sexual impotence.
Ataque de nervios: “fit”-like paroxysm of emotionality and may be used to indicate an episode of loss of control in response to an intense stressor
Panic attack Dissociative disorder Intermittent explosive disorder Other anxiety Trauma and stressor-related disorder
Amok: Homicidal and subsequent suicidal behavior of mentally unstable individuals that results in multiple fatalities and injuries to others
Dissociative disorder
Susto: Condition of being frightened and chronic somatic suffering stemming from emotional trauma or from witnessing traumatic experiences lived by others
Major depressive disorder Post-traumatic stress disorder Somatic symptom disorders
Maladi moun: Also called “sent sickness.” It is a cultural explanation in Haitian communities for diverse medical and psychiatric disorders. It is assumed that interpersonal envy and malice cause people to harm their enemies by sending illnesses such as psychosis, depression, social, or academic failure, and inability to perform activities of daily living. Also expressed in the form of “evil eye” in some countries.
Delusional disorder, persecutory type Paranoid schizophrenia
Koro: Characterized by extraordinary dread of genitalia shrinkage, withdrawal of genitalia into abdomen, and ultimately culminating in death
Panic attack Hypochondriasis Can be delusional disorder in case of firm conviction
Falling out/Blacking out: The individual collapses without warning, occasionally with some degree of salivation but without convulsions, tongue biting, bowel or bladder incontinence. The person affected usually hears and understands what is happening but is powerless to move.
Dissociative disorder/Conversion disorder
Shenjing Shuairuo: Characterized by physical and mental fatigue, dizziness, headaches, somatization, concentration difficulties, sleep disturbance, and memory loss
Mood disorders Anxiety disorders
Tajin Kyofusho: Fear of experiencing embarrassment in front of others
Social phobia
Hikikomori: Affected individuals refuse to leave their parents’ house, do not work or go to school, and isolate themselves away from society and family in a single room for a period exceeding 6 months
School refusal
Pibloktoq: Abrupt dissociative episode with 4 phases—social withdrawal, excitement, convulsions, and stupor followed by recovery; mostly seen in women during winters in the arctic belt
Dissociative disorder
Controversy regarding considering CBS disorders as a separate entity: A long ongoing debate among researchers is whether the CBS should be considered a separate entity than existing diagnostic entities. Differences in the emotional, symptomatic, and contextual aspects of cultural syndromes signal different comorbid relationships with psychiatric diagnosis or even lack of such a relationship.8, 10 Proponents of CBS being a separate entity put forward the viewpoints that if cultural syndromes are incorporated into descriptive oriented classificatory systems, it would lead to the loss of their unique individual meaning from a cultural perspective, as the international classificatory systems have rigid (phenomenological) boundaries of the disorders to enable research and clinical practice. This might also lead to exclusion of culturally influenced alternative variants of these disorders.10 Further, the criteria of classification of CBS have been changing over time,7 which makes the debate unending and add on new controversy every time.
Is merging culture bound syndromes into pre-existing diagnostic categories the way ahead? To establish the salience of a new CBS and the extent of its recognition within a cultural group is a herculean task.7 Long back in 1994, Late Prof NN Wig had cautioned that separately categorizing CBS will not necessarily improve the management of these cases in any country’s health services.11 Further, it had been highlighted by prominent cross-cultural researchers that once cultural considerations are accepted as part of all diagnostic categories in the classification system, it will no longer be necessary to group specific, culturally determined behavior patterns into the disjunctive category of “culture-bound syndromes” in the DSM-IV.12 Moreover, if one thinks of abandoning CBS, it will lead to considering all psychiatric illnesses to be culture-bound and recognizing the cultural aspect will make culture-bound patterns as an afterthought.13 All these arguments made by the proponents of CBS makes one to introspect that in the face of globalization, the CBS are likely to disappear in the increasingly homogenous world culture and still, there is no rule-based system for relating cultural syndromes to psychiatric diagnosis.14 In the absence of any established standards, it isn’t easy to make definite inferences.
Issues related to the changing concepts of CBS over time: Another point of contention is determining whether the culture-related specific syndromes are always static and permanently bound to a culture.15 In this regard, researchers have reported that few recognized syndromes evolve or fade away as the cultural traits or circumstances that contribute to specific syndromes are modified in association with changes in society. Many culture-related specific syndromes recognized in the past are either changing in nature or diminishing in occurrence unless the cultural impact is very significant and deserves special attention.15, 16 There is also an unsettled issue to determine if a particular CBS disorder is culture-induced or culture interpreted disorder. For example, “Hwabyung,” “Susto,” and “Ataques de nervios” fall into culturally interpreted or culturally labeled disorders. However, many psychiatrists are of the view that there lies a great risk of misinterpretation in attempts to identify and explain culture-related specific disorders based exclusively on secondary information in literature, without psychiatric examination of actual cases.
Issue related to the authenticity of few CBS: genuine phenomena or a myth? One of the most pertinent questions that still need to be answered remains whether few CBS are genuine phenomena or just myths. The most straightforward way a CBS may fail to be a real disorder is if the behaviors that characterize it do not actually occur.17 To do research on a particular culture-bound syndrome that is limited to a specific geographical area/location, the researcher must closely observe the cases. He/she might have to travel far and wide and may have to have to rely on interpreters to understand the behavior frequently. While this can be quite tedious, observing genuine cases first-hand may be impossible in many scenarios; consequently, those who describe the disorder/syndrome may resort to relying on reports that are second or even third-hand interpretations of native people or regional interpreters. For example, in case of “Windigo psychosis,” stories of penis-shrinking anxieties or “Koro,” sudden homicidal rages or “Run Amok,” cannibalism, and so on have been told and retold, and with each interpretation, some interpretation might get embellished with each retelling. “Windigo psychosis” which represents a psychotic state characterized by an obsessional craving for human flesh that occurs among the Northern Algonkian people can be a perfect example of such confusion in which tales and facts had led to several bewilderment. Lou Marano,18 spent 5 years for doing the fieldwork on “Windigo psychosis” among Northern Algonkians, conducted an extensive archival search, analyzed the case reports, and found out that none of the previously published data provided any first-hand accounts of psychotic cannibalism and thereby, concluded that “Windigo phenomenon” is more of an example of mass suggestibility amongst anthropologists rather than a true phenomena. Such scenarios often create dilemma among the researchers and question the authenticity of the actual phenomena.18 To overcome such confusion, the non-local researchers should collaborate with local/native speaking researchers to carry out research to derive meaningful and authentic data on any CBS.
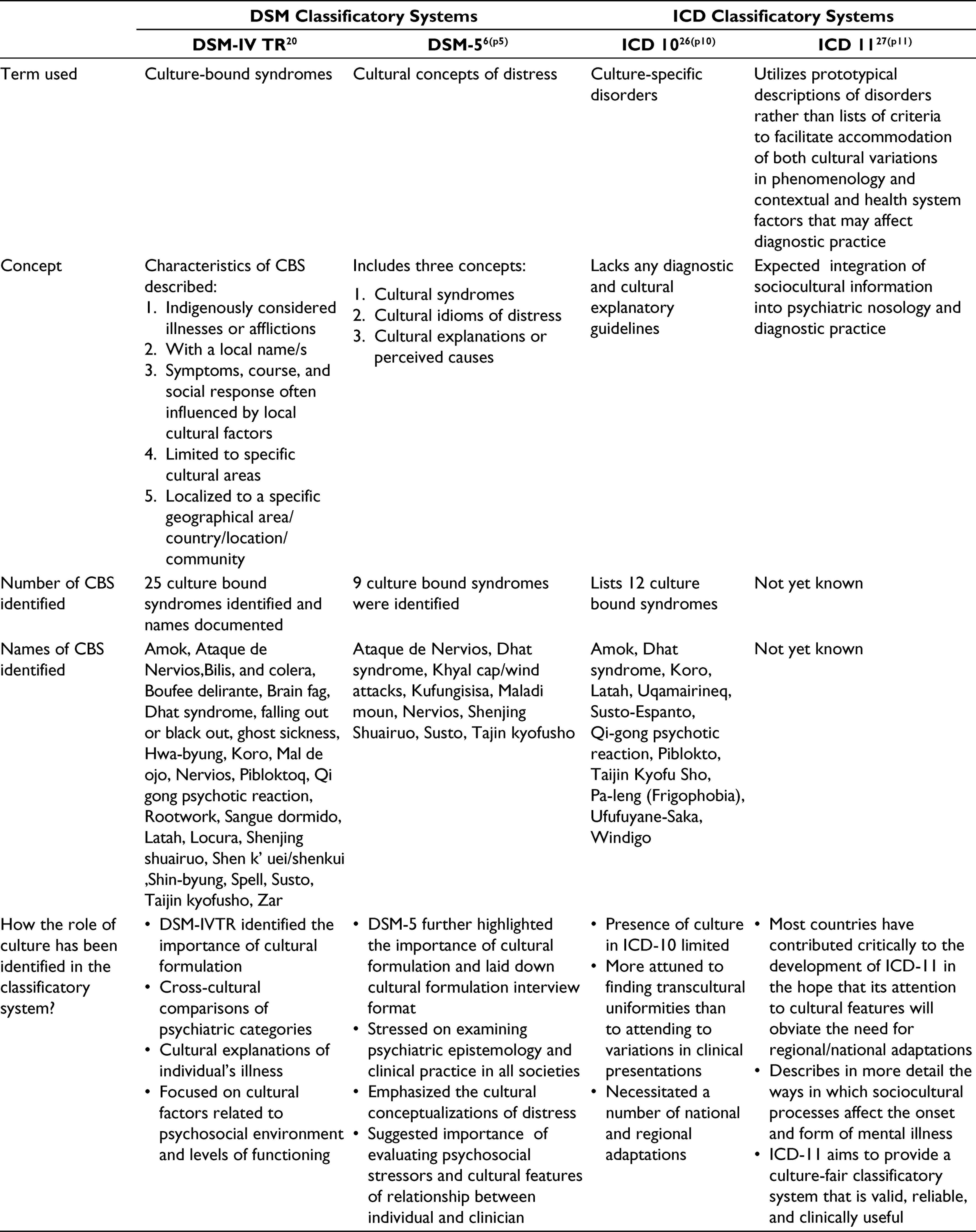
Issues related to the nosology of CBS in current classificatory systems: Classification of CBS within the DSM embraces putative disorders that invoke different levels of theoretical maturity.19 Over the years, the nosology of CBS had undergone a pragmatic shift both in DSM systems and International Classification of Disease (ICD) classificatory systems. While in DSM classificatory system, the DSM-5 had replaced the term CBS with “cultural concepts of distress” and had reduced the number of CBS in the glossary of cultural concepts of distress from 25 (DSM-IV TR, 2000)20 to only 9 (DSM-5, 2013).6 Similarly, in the ICD systems, the CBS were termed as “culture-specific disorders” and were mentioned in annex 2 containing 12 CBS; the upcoming ICD-11 summarizes the information on cultural variations in modes of describing the distress, symptom patterns, and dysfunctions of each disorder in order to promote the culturally sensitive application of the diagnostic system. ICD-11 further had mentioned that cultural idioms of distress are not equivalent to trauma and the gender and cross-cultural issues working group of ICD-11 is working on this issue.5Table 2 depicts the different changes in the nosology of CBS so far.
Differences in the Concept of Culture-Bound Syndromes Amongst the Classificatory Systems
Utilizes prototypical descriptions of disorders rather than lists of criteria to facilitate accommodation of both cultural variations in phenomenology and contextual and health system factors that may affect diagnostic practice
Concept
Characteristics of CBS described: 1. Indigenously considered illnesses or afflictions 2. With a local name/s 3. Symptoms, course, and social response often influenced by local cultural factors 4. Limited to specific cultural areas 5. Localized to a specific geographical area/country/location/community
Includes three concepts: 1. Cultural syndromes 2. Cultural idioms of distress 3. Cultural explanations or perceived causes
Lacks any diagnostic and cultural explanatory guidelines
Expected integration of sociocultural information into psychiatric nosology and diagnostic practice
Number of CBS identified
25 culture bound syndromes identified and names documented
9 culture bound syndromes were identified
Lists 12 culture bound syndromes
Not yet known
Names of CBS identified
Amok, Ataque de Nervios,Bilis, and colera, Boufee delirante, Brain fag, Dhat syndrome, falling out or black out, ghost sickness, Hwa-byung, Koro, Mal de ojo, Nervios, Pibloktoq, Qi gong psychotic reaction, Rootwork, Sangue dormido, Latah, Locura, Shenjing shuairuo, Shen k’ uei/shenkui, Shin-byung, Spell, Susto, Taijin kyofusho, Zar
How the role of culture has been identified in the classificatory system?
• DSM-IVTR identified the importance of cultural formulation • Cross-cultural comparisons of psychiatric categories • Cultural explanations of individual’s illness • Focused on cultural factors related to psychosocial environment and levels of functioning
• DSM-5 further highlighted the importance of cultural formulation and laid down cultural formulation interview format • Stressed on examining psychiatric epistemology and clinical practice in all societies • Emphasized the cultural conceptualizations of distress • Suggested importance of evaluating psychosocial stressors and cultural features of relationship between individual and clinician
• Presence of culture in ICD-10 limited • More attuned to finding transcultural uniformities than to attending to variations in clinical presentations • Necessitated a number of national and regional adaptations
• Most countries have contributed critically to the development of ICD-11 in the hope that its attention to cultural features will obviate the need for regional/national adaptations • Describes in more detail the ways in which sociocultural processes affect the onset and form of mental illness • ICD-11 aims to provide a culture-fair classificatory system that is valid, reliable, and clinically useful
It has been highlighted by several working group of researchers that systematic scientific investigation into the explanations for the behavior expressed by those with these CBS “disorders,” 1 of 4 outcomes with respect to each CBS can be expected. These can either be (a) retention as a bona fide disorder, caused by culture-specific factors, and therefore correctly listed as legitimate, (b) retention and refinement of the “disorder” under a scientifically improved description, which is justifiably deemed to be a CBS, (c) assimilation of the “disorder” as a variant of a currently listed (and furthermore, justifiably listed) non-CBS, or (d) there can be elimination of the “disorder” outright as invoking false explanations for behavior.16, 19 So it is time to rethink whether the nosology of CBS would be assimilated or eliminated in the near future. For both the scenarios, robust research on each individual CBS needs to be carried out to reach to any definite solution.
Issues related to publications and research on various culture-bound syndromes: Most of these controversies arise due to limited research on various CBS, especially from non-Western countries where the bulk of CBS originates.7 Moreover, around 50% of all transcultural investigations are related explicitly to CBS, yet the research output is sparse. Few reasons behind this are the high rate of rejection (85%-99%) of the submitted papers from low- and middle-income countries by high impact journals, low scientific production in most of these countries, the concentration of research in less than one-third of the countries in Latin America and the Caribbean, and lack of adequate manpower, financial, and infrastructural resources for scientific research on the pertinent issues of various CBS. Research biases toward topics of interest to high-income countries, paucity of transcultural studies involving publication biases resulting in the poor visibility of such studies, and difficulty in elaborating adequate research strategies for various CBS contribute to inadequate research related to this area.15, 21 For example, on PubMed search of “Dhat syndrome” it was revealed that even after more than 50 years of introduction of the concept, only 74 articles appear in the search, of which 64 were published between 2000 and 2020. Although less studied, the silver lining is that a growing number of researchers are exhibiting interest in the “Dhat syndrome.” However, more studies in each culture-bound syndrome needs to be carried out to establish the impact on the specific population affected so that the relevance of the CBS does not fade out.
What is the Future of CBS: The Way Forward
The concept of culture-bound syndromes is shrouded in controversy and of uncertain nosological validity.7 The relabeling of “culture-bound syndromes” as “cultural concepts of distress” is a welcomed change.22 The relevance of CBS in the 21st century is worth-noticing. Rapid globalization and rampant immigration have led to intermingling of cultures, resulting in significant changes in the world’s social and economic changes where such syndromes were seen more often.21 There is every possibility that the presentation and phenomenology of the CBS might undergo a drastic change in the near future. Although the DSM-5 had highlighted the role of culture in management of different psychiatric disorders (cultural formulation), yet the changes have not been made part of the main sections of different psychiatric disorders and only have been suggested in glossary, appendices, and conditions requiring further study.23 While every now and then, a new CBS is being reported in some or other part of the world, the nosological status and validity of the CBS is always questioned.24, 25 A better understanding across the cultures of the CBS would require epidemiological studies in this area to ascertain if a specific CBS needs to be classified as separate disease entity or be explained on the basis of predominant presenting features under an established psychiatric diagnosis per the DSM/ICD system. Some of the suggestions for the way forward would be to carry out focused research on individual CBS, conduct research to establish the original cultural integrity of the previously described syndromes, and develop questionnaires and interview schedules/manual using open-ended questions and symptom checklists.15 To conclude, more emphasis should be placed on the need for proper cultural consideration of every disorder rather than specific syndromes in the current classification system.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
1.
WigNN. Problems of mental health in India. J Clin Soc Psychiatry. 1960;17:48–53.
2.
MumfordDB. The ’Dhat syndrome’: a culturally determined symptom of depression?Acta Psychiatr Scand. 1996;94(3): 163-167. doi: 10.1111/j.1600-0447.1996.tb09842.x.
3.
RajkumarRP, BharadwajB. Dhat syndrome: evidence for a depressive spectrum subtype. Asian J Psychiatry. 2014;9:57-60. doi: 10.1016/j.ajp.2014.01.007.
4.
SameerM. Is ‘pure’ Dhat syndrome a stable diagnostic entity? a naturalistic long term follow up study from a tertiary care centre. J Clin Diagn Res. 2015. doi: 10.7860/JCDR/2015/13399.6275.
5.
SharanP, KeeleyJ. Cultural perspectives related to International Classification Of Diseases-11. Indian J Soc Psychiatry. 2018; 34(5):1. doi: 10.4103/ijsp.ijsp_45_18.
6.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. American Psychiatric Association; 2013.
7.
KaiserBN, Jo WeaverL. Culture-bound syndromes, idioms of distress, and cultural concepts of distress: new directions for an old concept in psychological anthropology. Transcult Psychiatry. 2019;56(4):589-598. doi: 10.1177/1363461519862708.
8.
GuarnacciaPJ. Research on culture-bound syndromes: new directions. Am J Psychiatry. 1999;156(9):1322–1327.
9.
MezzichJE, BerganzaMA, RuiperezMA. Culture in DSM-IV, ICD-10, and evolving diagnostic systems. Psychiatr Clin North Am. 2001;24(3):407-419. doi: 10.1016/s0193-953x(05)70237-9.
10.
PaniaguaFA. ICD-10 versus DSM-5 on cultural issues. SAGE Open. 2018;8(1). doi: 10.1177/2158244018756165.
11.
WigNNAn overview of cross-cultural and national issues in psychiatric classification. In: MezzichJ. E., HondaY. & KastrupM. C. (eds.), Psychiatric diagnosis: A world perspective. Springer; 1994:3–10.
12.
HughesCCThe CBSs and psychiatric diagnosis. In: MechJ., KleinmanA, FabregaH., & ParronD. (eds.), Culture and psychiatric diagnosis: A DSM-IV perspective. American Psychiatric Association; 1996:49–62.
13.
LittlewoodRCultural comments on culture bound syndromes. In: MezzichA., KleinmanH., Fabrega, (eds.), Culture and psychiatric diagnosis: A DSM–IV perspective. American Psychiatric Association; 1996:309–312.
14.
PerezS, JunodA, PilardM. Culture-bound syndromes: pertinence as a diagnostic category. Med Trop Rev Corps Sante Colon. 2000;60(1):75–82.
15.
TsengW-S. From peculiar psychiatric disorders through culture-bound syndromes to culture-related specific syndromes. Transcult Psychiatry. 2006;43(4):554-576. doi: 10.1177/1363461506070781.
16.
BalharaYPS. Culture-bound syndrome: has it found its right niche?Indian J Psychol Med. 2011;33(2):210-215. doi: 10.4103/0253-7176.92055.
17.
CooperR. Are culture-bound syndromes as real as universally-occurring disorders?Stud Hist Philos Sci Part C Stud Hist Philos Biol Biomed Sci. 2010;41(4):325-332. doi: 10.1016/j.shpsc.2010.10.003.
18.
MaranoL. Windigo psychosis: the anatomy of an emic–etic confusion. Curr Anthropol. 1982;23(4):385-412. doi: 10.1086/202868.
19.
BleaseC. Scientific progress and the prospects for culture-bound syndromes. Stud Hist Philos Sci Part C Stud Hist Philos Biol Biomed Sci. 2010;41(4):333-339. doi: 10.1016/j.shpsc.2010.10.013.
20.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). 4th ed-Text Revised. American Psychiatric Association; 2000.
21.
VentriglioA, AyonrindeO, BhugraD. Relevance of culture-bound syndromes in the 21st century. Psychiatry Clin Neurosci. 2016;70(1):3-6. doi: 10.1111/pcn.12359.
22.
BalharaYPS, GoelR. Culture bound syndromes: need to relook, relabel and include?Asian J Psychiatry. 2011;4(1):75. doi: 10.1016/j.ajp.2011.01.007.
23.
JacobKS. DSM-5 and culture: the need to move towards a shared model of care within a more equal patient–physician partnership. Asian J Psychiatry. 2014;7:89-91. doi: 10.1016/j.ajp.2013.11.012.
24.
KeshavanMS. Culture bound syndromes: disease entities or simply concepts of distress?Asian J Psychiatry. 2014;12:1-2. doi: 10.1016/j.ajp.2014.11.003.
25.
NathK, BhattacharyaA, SinhaP, PraharajSK. Devaki syndrome: a culture-bound psychological reaction in Indian Hindu women in response to repeated pregnancy loss?Asian J Psychiatry. 2015;13:13-15. doi: 10.1016/j.ajp.2014.12.007.
26.
World Health Organisation. ICD-10 classification of mental and behavioural disorders. WHO. https://icd.who.int/browse10/2010/en#/F50-F59
27.
WHO. ICD-11—Mortality and Morbidity Statistics. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281. Accessed November2, 2019.