
Abstract
Introduction:
Numerous psychiatric disorders are known to be associated with risky sexual behavior (RSB). Depression or substance use is known to be higher in those who are in sex work. Recent literature has also described the association between attention-deficit hyperactivity disorder (ADHD) and RSB. However, the association between ADHD and RSB among women in sex work (WSW) is relatively unknown. In this background, this study was conducted to study the prevalence of ADHD and associated psychiatric correlates among WSW and also to study the prevalence of RSB in this population.
Methodology:
A sample of 96 women who were in sex work and consented to be the part of the study were recruited. They were later administered Adult ADHD Self-Report Scale to screen for adult ADHD symptoms, Wender Utah Rating Scale to retrospectively look into a childhood diagnosis of ADHD, MINI neuropsychiatric interview for DSM 4-TR psychiatric diagnoses, HIV Risk Behavior Scale to study RSB, Beck’s Depression Inventory to quantify depression, and Presumptive Stressful Life Events Scale to quantify the presence of stressful life events.
Results:
The prevalence of Adult ADHD in the sample was 32.20 % (n = 31). Individuals with ADHD had a higher prevalence of RSB (P = .02), comorbid depression (P = .04), presence of stressful life events (P = .001), and a higher prevalence of sexually transmitted infections (P = .03).
Conclusion:
The prevalence of ADHD is high among WSW (32%). Risky sexual behavior in this population could be probably due to higher prevalence of associated psychiatric conditions including depression, higher presence of stressful life events, and ADHD, the association which is less understood. There is a need to replicate these findings in larger samples to study ADHD and its relationship with risky sexual behavior among WSW.
Introduction
Women in sex work (WSW) are defined as those women who provide sexual services for payment in the form of money typically in the previous month. 1 A multitude of psychological and psychiatric factors are associated with women who are involved in sex work. Psychiatric diagnoses such as substance dependence and depression are also associated with WSW. 2 There is also recent evidence on attention-deficit hyperactivity disorder (ADHD) being associated with RSB. Literature has also suggested that ADHD is linked to early onset of experimentation with risky sexual practices. 3 Another study also has suggested that men with childhood ADHD were more likely than men without ADHD to have reported the presence of risky sexual practices such as casual sex, inconsistent condom use, and multiple sex partners. 4 Most studies on ADHD have only studied male participants, with ADHD-related outcomes being poorly studied among WSW. 5
Another study by Pandiyan et al 6 had reported a prevalence of 34% of ADHD among WSW but this study was statistically underpowered. A study by Flory et al 4 on RSB among females reported that persistent presence of impulsiveness with other factors such as disordered attachment and conduct disorder symptoms were associated with RSB in young women. Another Indian study by Kumar et al 7 has previously reported a prevalence of 20% of ADHD symptoms among young men who had a new diagnosis of HIV.
Thus, ADHD is possibly associated with RSB which is a recognized risk factor for sexually transmitted infections (STIs). As there is paucity of literature on the association between ADHD, depression and psychiatric diagnoses, stressful life events, and RSB among WSW, this study was undertaken to study this association.
Aims and Objectives of the Study
To study the prevalence of ADHD and RSB among women involved in sex work who were referred to the outpatient psychiatric clinic of a tertiary care teaching hospital.
To study the association between the above variables and risky sexual behavior.
Materials and Methods
Study Setting and Design
It was a cross-sectional study conducted at a psychiatric outpatient clinic of a tertiary care teaching hospital. Most of the study sample was recruited through nongovernmental organizations (NGOs) providing mental health psychosocial services to WSW. The study sample size was 86. These organizations refer patients to a psychiatric outpatient clinic who have mental health issues of WSW. Ten participants were recruited to the study by chain referral through participants. Thus, a total of 96 eligible participants participated in the study. Institutional ethical committee clearance was obtained for the study. Informed consent was obtained from all participants who enrolled for the study.
Inclusion Criteria
WSW above the age of 18 years who provided informed consent.
Exclusion Criteria
Participants who had terminal medical illness who could not be interviewed for the study.
Methodology
The study subjects were administered the following scales:-
A semi-structured interview was used to obtain sociodemographic data which included details such as age, locality, marital, educational and employment status, and income earned. This also included details of risky sexual behavior and substance use. Medical symptoms of sexually transmitted diseases were assessed with a skin and venereal disease specialist consultation. Investigations such as urine routine, culture, urethral smear, Venereal Disease Research Laboratory, and ELISA-HIV were obtained during the consultation. Adult ADHD Self-Report Scale (ASRS) was used to screen for ADHD symptoms. This scale was developed by the World Health Organization. A shorter version of the same which consists of 6 questions on symptoms of ADHD in the past 6 months based on the DSM-IV-TR criteria was used. Study subjects need to rate each question on a 5-point response scale from “Never” [0] to “Very often.”4,8 A cut-off of 14 for the first 6 items of the screener was used to make a diagnosis of ADHD which was described in a paper by Kessler.
9
Also, study population who scored a total of 9 or more of the shaded boxes were diagnosed to have ADHD symptoms. Wender Utah Rating Scale (WURS) was used to make a retrospective assessment of childhood ADHD. ADHD was diagnosed if a study subject scored a cut-off of 24 or above on the full ASRS scale with a WURS score of 46.
10
HIV Risk Behavior Scale (HRBS)-sexual behavior subsection of HRBS was used to assess for RSB.
11
MINI neuropsychiatric interview was used for assessment of psychiatric diagnoses based on DSM 4-TR criteria.
12
Psychiatric diagnoses such as depression and psychosis may mimic ADHD symptoms. Beck’s Depression inventory 2 which is a self-rated instrument was used to assess the severity of depression.
13
Presumptive Stressful Life Events Scale (PSLES) was used to assess the presence of stressful life events. This scale generates a score based on the presence and type of stressful life event.
14
Basic psychoeducation about safe sex practices, regular follow-up for psychological issues, and compliance to medications, if prescribed, were done. For those individuals with psychological symptoms, a clinical psychology referral was given for psychotherapy.
Statistical analysis was done using SPSS v 19. Chi-square test was used to compare categorical variables such as RSB in ADHD. t Test was used for studying continuous variables such as depression, stressful life events, and risky sexual behavior scores. Pearson’s correlation coefficient was used for various correlations.
Results
The prevalence of ADHD symptoms in the study sample using an ASRS cut-off of 24 or above with a WURS cut-off of 46 or above was 32.2% (n = 31).
Discussion
The prevalence of ADHD symptoms among the study population of WSW was 32.2%. It is described that individuals with ADHD indulge in impulsive behaviors probably due to executive dysfunction of which RSB assumes clinical importance. Depression which is frequently cooccurring with ADHD may in addition contribute to the burden of RSBs. 2 Individuals with ADHD also have comorbid substance use, 15 which adds on to the burden of RSB. This is concordant with the present study finding of higher depression scores and RSB scores (Table 6).
Those with presence of ADHD were younger, had lower years of education, and higher income which was statistically significant (Table 1). This could be explained by the fact that those with ADHD have an earlier sexual debut 3 and thus could take up sex work as a profession yielding higher income than those without ADHD. In addition, the executive function deficits in ADHD as described by Barkeley 16 could contribute to academic underachievement.
Sociodemographic Characteristics of the Study Sample
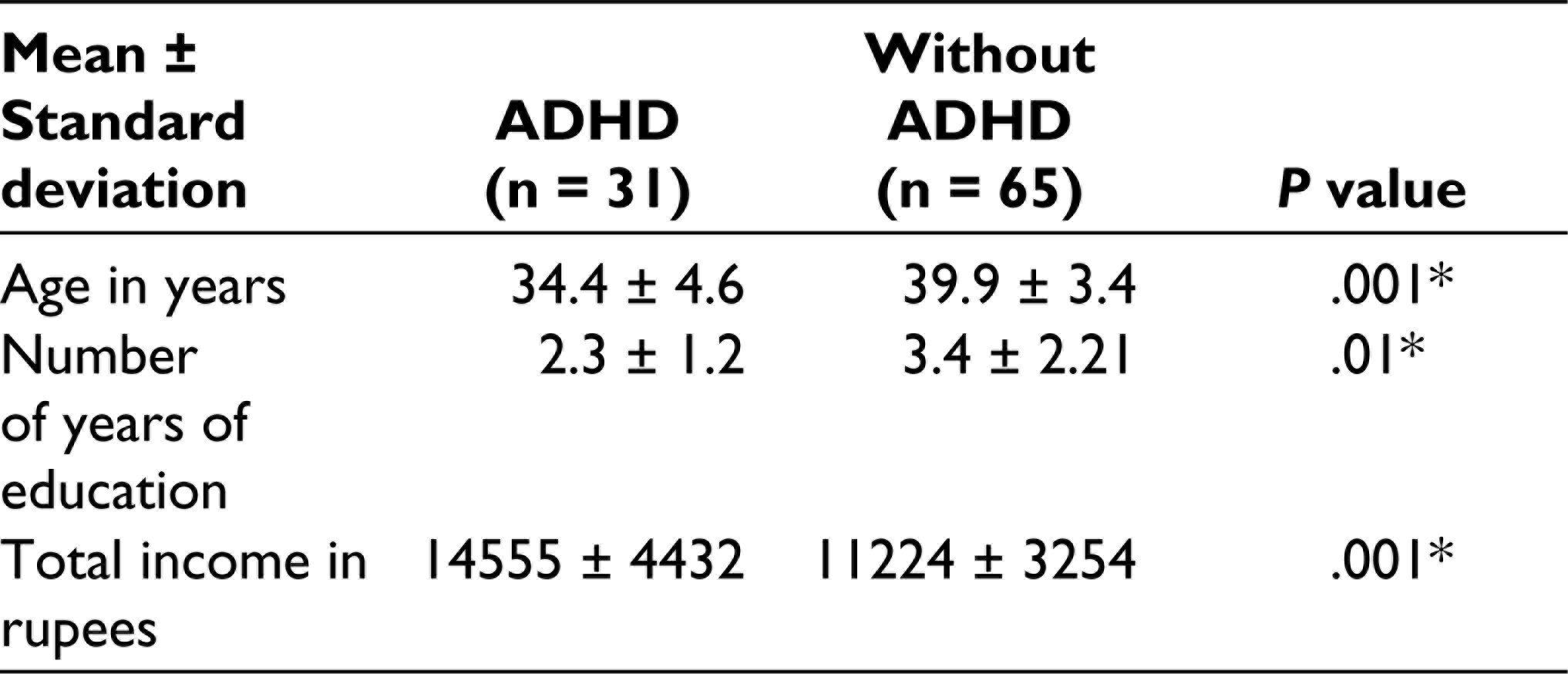
*Those with ADHD were younger, had lesser years of education, and higher income.
As stated earlier, the prevalence of RSB in the study sample was relatively high (32%). Presence of RSBs in the sample included having multiple sex partners, inconsistent use of contraception, higher number of partners, unsafe injection use, and alcohol use prior to sexual activity. On clinical interview, reasons for these unsafe sexual behaviors as stated were that these WSW received more monetary benefit from clients when contraception was not used despite the fact that these women had awareness about safe sexual practices and risk of STIs with unsafe sex. Those with presence of ADHD had less consistent contraceptive use and higher frequency of alcohol use prior to sexual activity which was statistically significant (Table 2). This could possibly be explained by executive function deficits such as lack of behavioral inhibition which leads to impulsiveness, emotional dysregulation, and risk taking behaviors as stated by Barkeley. 16
Comparison of Risky Sexual Behaviors of Those With and Without ADHD
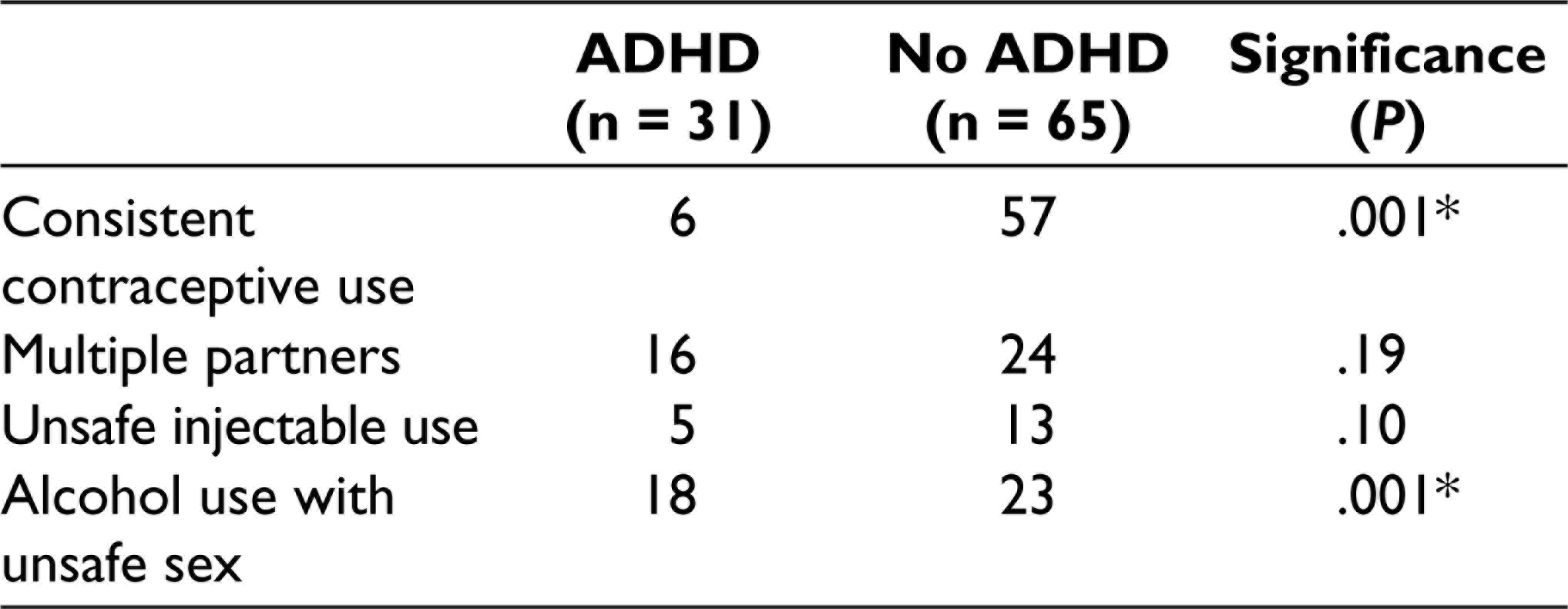
*Those with ADHD had less consistent use of contraception and higher use of alcohol use with unsafe sex than those without ADHD.
Those with ADHD also had a higher prevalence of depression and presence of stressful life events. ADHD-associated comorbidities such as depression 2 and executive functioning deficits 16 could enhance perceived stress which could possibly contribute to higher stressful life events score (Table 3). Thus, it could be speculated that presence of ADHD, in addition to depression and stress, could contribute to RSBs from the findings of the present study (Table 4).
Comparison of Stressful Life Events, Depression, and Risky Sexual Behavior in Those With and Without ADHD
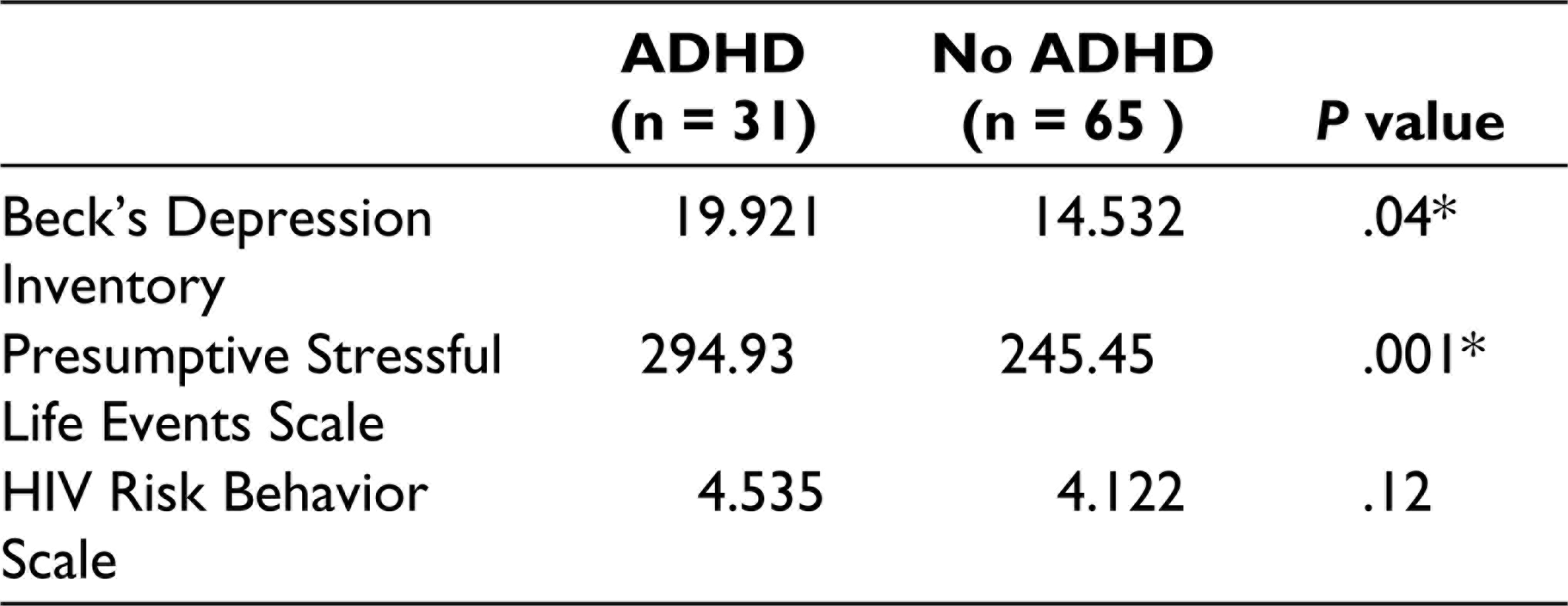
*Those with ADHD had higher depression and stressful life events score than those without ADHD which was statistically significant.
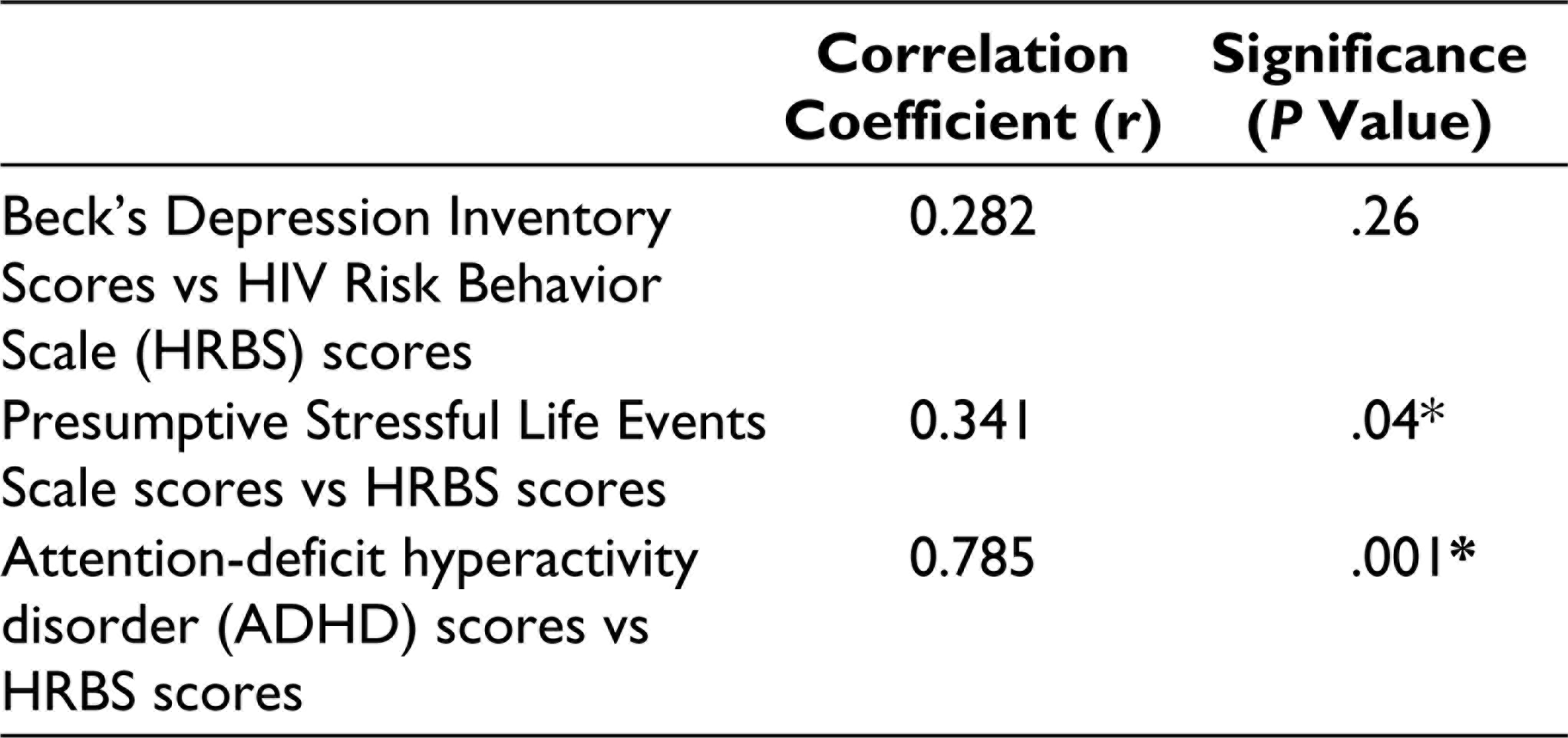
Correlations Between Depression, Stressful Life Events, and ADHD Scores With Risky Sexual Behavior
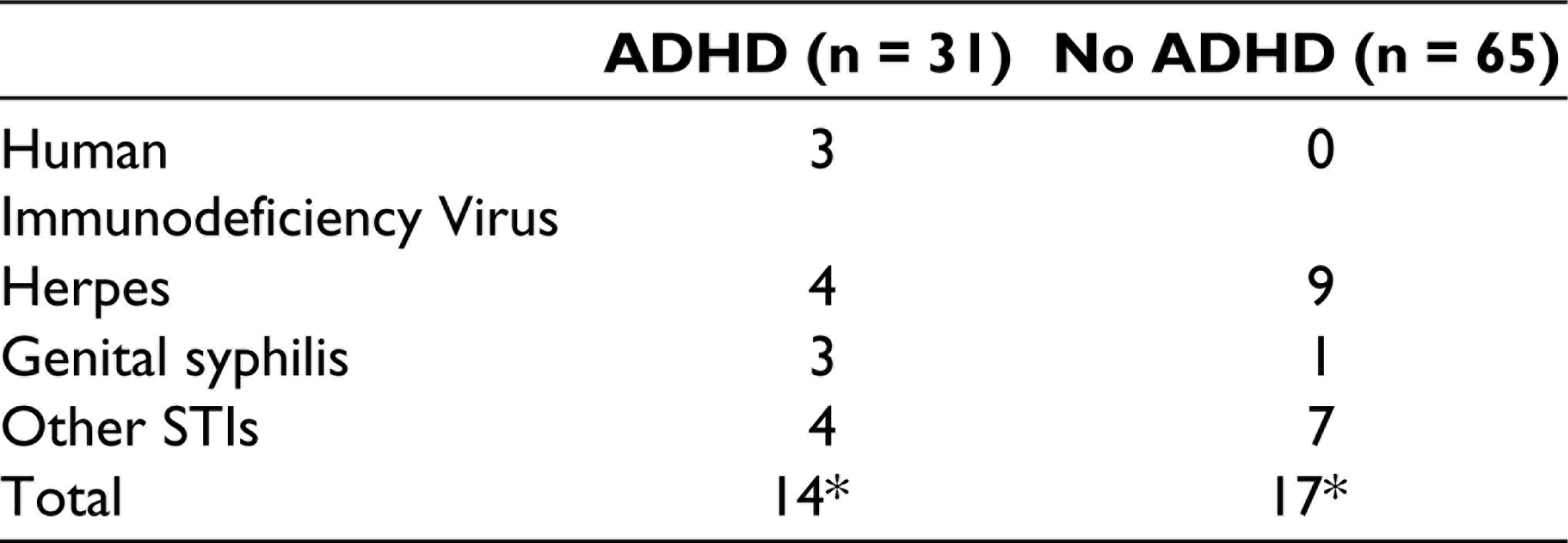
The prevalence of STIs in the sample was 26.04%. Those with presence of ADHD had a higher prevalence of STIs as compared to those without ADHD (P = .03*). Notably, only those with ADHD had presence of HIV infection (Table 5).
Presence of Sexually Transmitted Infections in the Study Sample
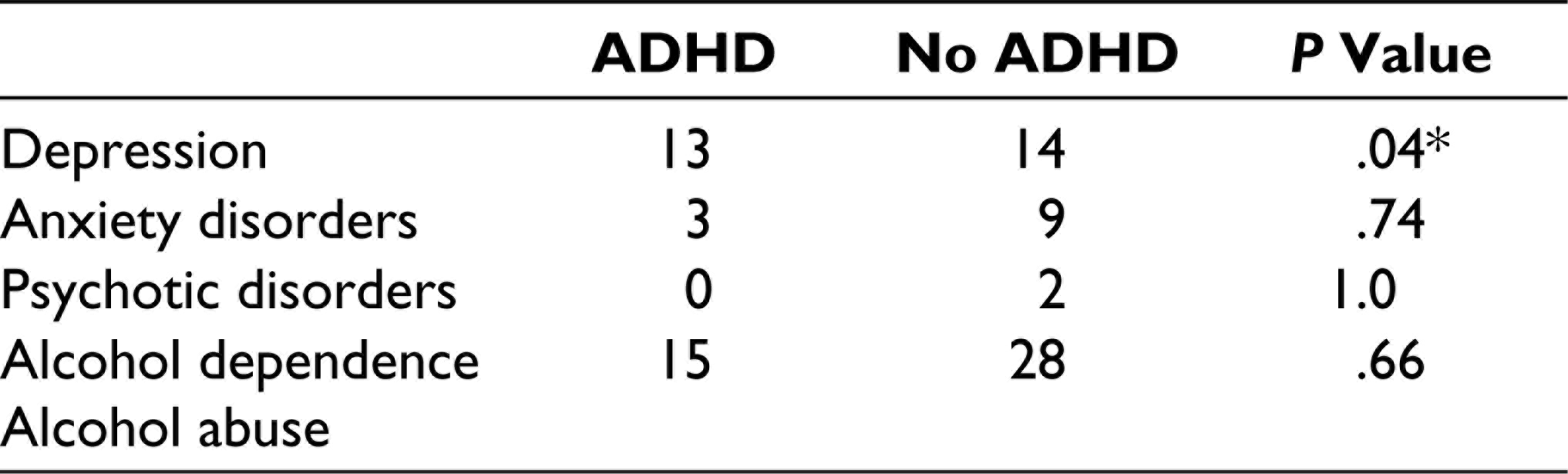
MINIPLUS Scores Among Women in Sex Work
Conclusion
There is a high prevalence of RSB and STIs among WSW. This could be explained by presence of psychiatric diagnoses such as depression, stress, and ADHD, the interaction among which is less frequently understood and studied.
Limitations
The study was statistically underpowered.
It had a cross-sectional study design. Longitudinal studies can establish a better strength of association of the currently hypothesized relationship.
The study population may not be a true representation of the burden of this community as a whole as the subjects studied were referred by NGOs which could indicate a referral bias. The current estimates may actually be an overestimate. There is a need for community-based studies among the same population.
Though ADHD diagnosis was made using ASRS, it is a screening tool. In depth, clinical interviews could have provided a better validity of the diagnosis as many other psychiatric conditions including mood disorders, personality disorders, post-traumatic stress disorder, and psychosis can be ADHD mimics. These conditions need to be ruled out using in depth assessments before confidently making a diagnosis of ADHD in adulthood.
Further Directions
Though there is an association established between ADHD and risky sexual behavior, causality cannot be assumed as there could be multiple psychiatric and psychological factors which could mediate the association between these factors which need to be studied in greater depth. There is a need for longitudinal studies to establish an association between ADHD, RSB, and STIs.
There is also a need for large-scale longitudinal studies looking at ADHD among WSW which could help in understanding this association better for designing management and preventive strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.