
Abstract
Masturbatory behaviors occur as a part of psychosexual development in young children, but if such behaviors exceed resulting in discomfort and disability, it is known as gratification disorder. Children with such genital self-stimulatory behaviors are infrequently seen and diagnosed in Asian outpatient settings, possibly due to prevalent stigma. We report the cases of 3 children of 3, 4, and 8 - year-old with the diagnosis of gratification disorder based on comprehensive history-taking, general physical examination, and neurological examination along with videotape recording of the event. Investigations such as electroencephalogram (EEG), urinary microscopic examination, and culture were also conducted in each case. Clinical history, examination, and investigations such as EEG and urinary examination were reviewed. Behavior therapy and psychoeducation were successful in alleviating the disorder and allaying parental fears of taboo in all these cases. There was significant improvement in self-genital stimulatory behavior in all 3 cases at 3 months follow-up.
Keywords
Introduction
Masturbatory behavior is a universal aspect of psychosexual development. It is a normal and adaptive behavior which occurs as a part of genital exploration. Such masturbatory behaviors have been reported in 90% to 94% of males and 50% to 60% of females at some point in their lives with age of onset being typically in age of 3 months to 3 years and a second peak of incidence in adolescence. 1 These gratification behaviors in excess leading to discomfort and disability are referred to as gratification disorder which rarely occurs in children. 2
Although childhood masturbation had been discerned as early as 1909 by Still, 3 the understanding of these behaviors is fairly limited. A myriad of different behavior patterns can present as gratification behaviors. As a result, infantile masturbation, known as benign idiopathic infantile dyskinesia, is frequently misconstrued as epilepsy,4,5 abdominal pain,6,7 and paroxysmal dystonia or dyskinesia. 8 Case reports have also shown that multiple unjustifiable investigations such as gastrointestinal radiography, 4 pyelography, and cystoscopy-vaginoscopy-proctoscopy under general anesthesia were conducted in these children. 6 Therefore, the acknowledgement of the clinical manifestations of gratification disorder can prevent misdiagnosis, unnecessary investigations, and treatment.
Though such self-genital stimulatory behaviors have been reported in Western literature, there are few reports illustrating clinical manifestations, course, and treatment of children with such masturbatory behaviors especially in developing countries. This could be explained by the infrequent outpatient presentations involving such behavior as a result of stigma along with lack of adequate sexual education and lack of channels for communication regarding the same in Asian society. Thus, the objective of this case series is to depict clinical profile, treatment, and long-term follow-up of gratification disorder to improve the recognition of such masturbatory behaviors in children and its treatment patterns with their efficacy.
Representative Case Reports
Three children had presented to child psychiatry outpatient department in Kanti Children Hospital in the year 2020 to 2021 for assessment of self-genital stimulatory behaviors. All of these cases were evaluated independently by the authors which included comprehensive history taking, general physical examination, and neurological examination along with videotape recording of the event. Investigations such as electroencephalogram (EEG), urinary microscopic examination, and culture were also conducted in each cases.
Case 1
A 3-year-old girl, first born out of nonconsanguineous marriage with uneventful birth normal developmental milestones, had presented with a history of 2 episodes of odd movements of the body with first episode at the age of 18 months for duration 6 months and second episode with onset being 6 months back. She was referred by dermatologist and pediatrician in acknowledgement of the parental worries of taboo associated with such behavior. All of these episodes were abrupt on onset and involved the child being in standing position with repetitive to and fro rubbing of genitalia against hard surface such as the seat of chairs or tables edges. These episodes were associated with grunting sounds and flushing of the face at the peak of the episodes. She was observed to be responsive to call and conscious during each episodes. These episodes were frequent when child was left alone, unattended, and terminated by distractions followed by the child returning to her play activities. These episodes occurred regardless of the presence of people and diurnal variation. Such episodes were never present during sleep. The frequency and duration of these episodes progressed from 2 to 3 episodes/day for 3 to 4 min to 20 episodes/day for 5 to 6 min over 4 to 6 months. Both the first and second episodes were preceded by diagnosis of urinary tract infection (UTI). She was treated with 1 week course of antibiotics which resulted in improvement in urinary symptoms but the self-genital stimulatory behavior persisted. History of sexual abuse was denied by mother. There was no family history of similar complaints or seizure disorder. No injuries were found on examination of genitalia. She had normal general and neurological examination with no significant findings in EEG.
Psychoeducation was provided to the parents and 5 sessions of behavior therapy with positive and negative reinforcement techniques were conducted over a period of 3 months. During the regular follow-up period of 3 months, there was significant improvement in self-stimulatory behaviors.
Case 2
A 4-year-old female child, nursery grade student, was brought to the outpatient department by her mother with complaints of abnormal body movements of 2 years duration with abrupt onset. The spells consisted of the child lying in the prone position with repetitive rocking of her body and genitals against the floor followed by pleasurable feelings in the child. During these episodes, she had periods of heavy breathing without loss of consciousness. All these episodes were associated with thrusting movement of hips. Throughout these episodes, the child was responsive to the call of her parents. Such episodes used to occur commonly while playing alone or watching television irrespective of the content of the show. However, these episodes used to never occur while the child was asleep. Such episodes were terminated on being reprimanded by her parents or on gentle restraints ensued by the child being tired for 5 to 6 min. The spells used to occur 1 to 2 times/week each of duration 10 to 15 min which gradually increased to 4 to 5 times/week each of duration 30 to 40 min over a period of one and a half years. Sexual abuse and seizure disorder were also ruled out on interviewing her parents. Her birth, developmental, and family history was unremarkable. During these period of 2 years, multiple pediatric and dermatological evaluations were done with normal findings on systemic, genital, and neurological examination. Investigations such as EEG, urinary microscopic examination, and culture were done with normal findings.
Psychoeducation and reassurance was provided to the parents regarding the nature and course of such masturbatory behaviors in children. Issues regarding the stigma of such self-genital stimulatory behaviors were also addressed. Four sessions of behavioral therapy including redirecting the child in other activities were conducted over a follow-up period of 3 months with significant reduction in symptoms.
Case 3
An 8-year-old girl was referred by a pediatrician for spells of repetitive hip thrusting movements. She was a term child born without complications with normal developmental history. She is a grade 1 student with such spells beginning 1 year back after observation of her female friend involving in the similar act in school. Such events occurred commonly during sitting or standing position in both home and school settings regardless of the presence of people. These episodes were described as rhythmic pelvic thrusting movements along with backarching and stroking her genitals against a hard surface such as edges of the beds or chairs. This was associated with a dazed, distant facial expression with the child being conscious and responsive to the calls of her parents. All these episodes had an abrupt onset and ceased with distraction by the parents. All these events were ensued by a pleasant feeling for the child. The progression of such spells increased from 3 to 4 episodes/week of duration 5 to 10 min to 5 to 6 episodes/week of duration 15 to 20 min during a period of 1 year. There was history of UTI after 6 months of the onset of the event with urinary routine examination revealing plenty red blood cells per high power field, 2 to 3 pus cells per high power field, and calcium oxalate crystals in urine. Antibiotic was prescribed for 1 week with improvement in urinary symptoms. There was no known history of sexual abuse and such spells did not occur during sleep. Family history was significant for her grandfather with anxiety disorder. Genitalia examination revealed clear, white, and odorless vaginal discharge with no excoriations. Both general physical and neurological examination were found to be normal. EEG, urinary routine examination, and culture done during the time of assessment was normal.
Parents were reassured, psychoeducation was provided, and 3 sessions of behavioral therapy with distraction techniques were done resulting in cessation of such episodes over a period of 2 months. There was no relapse of episodes during the 3 months follow-up. Summary of the three cases is described in Table 1.
Summary of the Three Cases
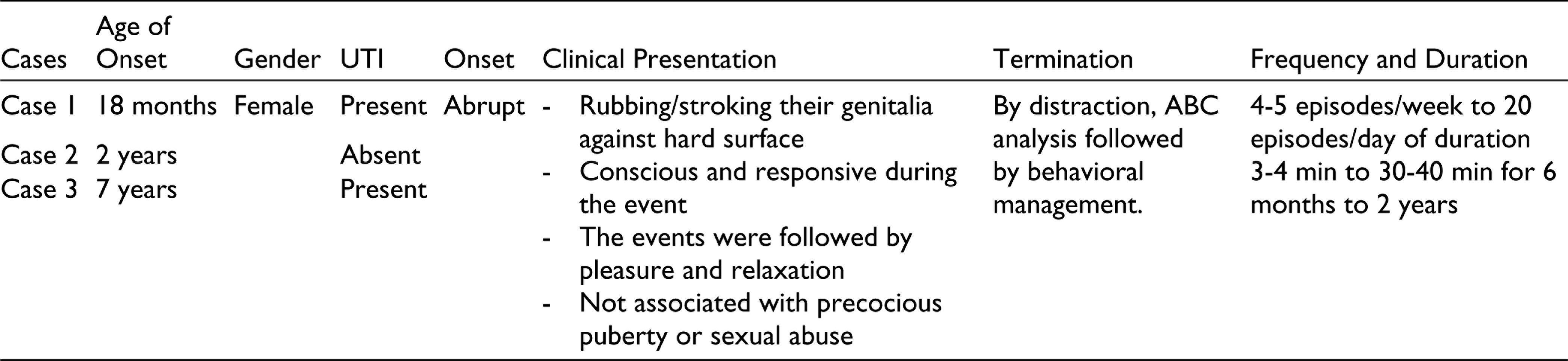
Abbreviations. UTI, Urinary tract infection.
Summary of Behavior Therapy for Three Cases
Behavior therapy was used for the management of the cases; (a) Psychoeducation and normalization: parent counseling was conducted, highlighting that masturbatory behavior in children is common. This is a normal phenomenon among children of both sexes 1 and does not harm the child in anyway 2 ; (b) Parents reported that they made critical comments (including scolding, threatening, and shaming) as an attempt to stop the masturbatory behavior. ABC model (functional analysis) was explained to them in order to help them understand how this behavior increased the child’s behavior rather than decreasing it. Scolding, threatening, and shaming the child could result in positive reinforcement of such behavior (i.e., scolding might increase the masturbatory behavior). 15 Method to manage these behaviors were discussed, “to engage the child in other play activities which could redirect their attention from masturbatory activities (i.e., distraction techniques).” They can gently explain to the child the importance of avoiding such behaviors especially in public places, then subsequently even in privacy as well, 5 (c) Session with the child: for cases 1 and 2, play and distraction activities were modeled, activity schedules were made with the child and their parents in the therapy sessions. The focus for management for the third case was (a) rapport building, ABC analysis of the problem, her understanding about the problems, (b) first level responses: allowing the child to ventilate, acknowledge, validate, universalize, and empathize with her concerns, (c) Sex education: information about masturbation. She was explained that individuals who masturbate are normal, but should follow the rule of privacy, 1 that is, masturbation in public is an unacceptable behavior.
Discussion
The term “gratification” is derived from Latin which refers to the pleasurable state on fulfillment of desires. 9 These gratification behaviors can occur as a part of normal psychosexual development in children which involves exploration of their sexuality and pleasurable sensations associated with it. There are several postulated contributory factors to these self-genital stimulatory behaviors which include environmental factors such as under stimulation, self-tension, excitement, and biological factors such as involvement of dopaminergic mesocorticolimbic circuitry and decrement in estradiol.10,11
As for the sociodemographic profile, this case series reported age of onset to be ranging from 18 months to 7 years with all cases being females. Majority of the case series and review also reported the age of onset to be between 3 months and 3 years.10,12,13 This could be explained by their inquisitiveness regarding genitals and gratification along with immature understanding of social restrictions. This is similar to the reports in some literatures showing that the masturbatory behaviors in children were more common in females.12-14 Nonetheless, it can be presumed to be due to the studies being conducted in low magnitude and sociocultural factors of masturbation being considered as normal in males resulting in low referral rates of males.
Furthermore, 2 of the 3 cases were diagnosed and treated as UTI which was similar to another review reporting UTI diagnosis in 2 among 19 children with gratification phenomenon. 13 Additionally, it can be observed that UTI could have a dual role of both contributing factors and consequences in gratification behaviors in these 2 cases. The rationale behind this could be due to the learned behavior in response to the perineal irritation caused by UTI. Likewise, the repetitive frictional behaviors of the genitals against hard surface could result in susceptibility to UTI. This also highlights the importance of vaginal pruritus in multiple medical conditions such as vaginitis, diaper rash, or eczema to be taken into consideration as differential diagnosis for self-sexual stimulatory behaviors.
These case reports also draw the focus on the significance of behavioral modeling as a predisposing factor in causation of gratification behaviors as seen in case 3. This eventually implicates the influence of early childhood exposure to sexual materials and acts in development of masturbatory behaviors in children. Hence, history of child sexual abuse and exposure to sexually explicit media and materials requires to be elicited during evaluation of gratification disorder. Moreover, the dazed appearance along with pelvic thrusting movements during such event of gratification episodes resulted in the consideration of seizure disorder in differential diagnosis with EEG done in all 3 cases. This was similar to the reports of misdiagnosis of self-genital stimulatory behaviors as epilepsy in children in various case reports and reviews.13,15,16 The findings such as no alteration of consciousness, termination with distraction, normal physical and neurological examination, and investigations can assist in the avoidance of mistaken diagnosis of gratification phenomena as epilepsy.
As for the treatment part, the consideration of masturbatory behaviors in children as taboo played a significant role in the reason for referral. This has been mentioned in another case report in Nigeria with disastrous consequences of female genital mutilation with the aim of decreasing the female child’s libido. 17 Therefore, this implies the need for normalization of the gratification phenomena in children as a part of their psychosexual development.
Regarding treatment approaches, the efficacy of the treatment approach of behavioral management along with positive and negative reinforcement and distraction was shown to be effective in all these 3 cases. This was similar to the reported benefits of behavioral therapy in other case reports.2,15 Furthermore, in cases of gratification disorder unresponsive to behavioral management, various psychopharmacological agents such as selective serotonin reuptake inhibitors (escitalopram) and antipsychotics (risperidone, aripiprazole) were recommended in other literatures.18–20 The mechanism of action of these medications was reported to be decrement in dopamine in mesolimbic system through D2 and 5-HT2 receptors. No pharmacotherapeutic intervention was done in the abovementioned cases since all the cases responded significantly to behavioral therapy.
The follow-up visits in this case series also indicated earlier improvement with behavioral therapy in older children than in younger children. The reason for this could be due to the eventual cognitive development and better understanding of social restrictions in children as they grow. However, the 3-month follow-up was short term for evaluation of relapse of such episodes. Nevertheless, based on these findings, behavioral treatment along with psychoeducation can be considered as a first-line management for gratification disorder.
Conclusion
Gratification phenomena is a normal phenomenon of psychosexual development in children. Factors such as modelling and perineal irritation require to be regarded as both predisposing factors and consequences of gratification behaviors. Reassurance, addressing the issues of stigma, and behavioral treatment can help in reducing the masturbatory behavior and spare children along with parents from unnecessary investigations and medications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.