
Abstract

Sexual health is a broad term that encompasses many aspects of sexuality. The World Health Organization (WHO) defines sexual health as,
a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled.
1
All individuals, including those with intellectual disability (ID), have the right to express and enjoy their sexual needs without being abused or exploited. However, in India there is a culture of silence surrounding this aspect of health that leads to what appears like denial of these needs. This has deleterious long-term consequences including a reduction in the likelihood of detecting child sexual abuse. Therefore, sexuality education starting early in life plays an extremely important role not only to inculcate healthy sexual practices but also to promote self-protection and prevent exploitation. It also ensures a better quality of life. Early Childhood Sexuality Education Task Force formulated guidelines for sexuality issues meant for children from birth to 5 years to inculcate right attitudes, values, and behaviors. 2
Education about sexuality is done as a part of life skills training in schools. It also happens in natural environment during conversations with parents and friends. Unfortunately, children with ID do not have adequate opportunities to learn from due to restricted upbringing, lack of resources, and mere denial of needs. In fact, there are perceived notions such as individuals with ID are asexual, 3 and sexuality is something to be feared or controlled. Individuals with ID are sexually active and express their sexual needs in diverse ways just as all other adults. Cognitive limitations should not become barriers to enjoying one’s basic rights. As sexuality and exerting sexual rights are critical for individuals with ID, it is recommended that proactive sex education, shared decision-making, and the implementation of sexual health care plans are addressed in the individual support plan. 4 While children with ID have the right to education about sexuality, parents and caregivers are often confronted with the dilemma of what to tell and how to initiate a meaningful discourse. They are also left with very few options especially in the Indian context where the topic is associated with stigma and taboo.
Sexual Needs of Children With ID
Sexual development is a dynamic and complex process, where biological and social factors interfere with each other. Sexual development and needs vary depending on the severity of ID, underlying cause for ID, and early social experiences. While some children may develop at the same pace as their peers, delay in adolescent sexual development is common and precocious puberty is rare. 5 Moreover, only some features of puberty may be affected depending on various biological factors such as genetic, morphological, constitutional, biochemical, and physiological conditions. 6 Expectations of individuals with ID regarding sexuality and its manifestation differ significantly depending on the level of their ID. 7 Psychosocial-sexual behavior of children with mild ID is similar to their peers—they explore, adapt, and control sexual impulses and urges, and respond to verbal mode of education. Development of secondary sexual features may be delayed in those with moderate ID; they function more at a reward and basic reinforcement level and may require behavior modification strategies based on operant conditioning and social learning for teaching to be effective. Children with severe-profound ID possess very poor control of sexual impulses, lack adaptive psychosocial-sexual behavior, function by having basic needs met, require significant caregiver support, and behavior modification techniques may be effective. 8
Parents’ Perspectives and Attitudes Toward Sexuality
Parents, guardians, and other caregivers functioning in a parenting role shall henceforth be referred to as parents. Parents are the first sex educators. 8 They serve as primary source for imparting values and educating youth about sexuality. Conversations with parents can become the yardsticks against which adolescents evaluate other information about sexuality and serve as a buffer against early sexual activity. But parents often feel inadequately prepared to educate their children on the subject of sexuality. Generally, they tend to have an abstinence-focused approach focusing on the negative aspects rather than positive aspects such as pleasure, love, and healthy relationships. 9 This holds true to parents of children with ID as well. In fact, for children with ID, sexuality is often pathologized or limited to hygiene and self-protection, 10 more so in the Indian context.
According to a study conducted in Mumbai, the common perceptions of parents were that puberty is expected but sexual behavior is unexpected, and there is a hope for cure. Their reaction to puberty onset varied with the gender of the child. Onset of puberty was perceived as an enabling factor for marriage among parents of female child. Marriage and childbirth were viewed as possible cure for ID by some parents. The common parental concerns expressed were early onset of puberty, safety, perception of child’s action by others, and concerns about the child’s family life, which also varied with the gender of the child, type of disability, and the socioeconomic background of the family. 11
Parents can create opportunities for their children to network and form meaningful personal relationships. 12 Working with parents to overcome parental overprotection and social isolation is critical. Providing opportunities for dialogue and sexuality focused education to them may facilitate more effective management of sexual health concerns in adolescents.13-15
“What, Why, and How” Model: A Prospective Illustrated Model for Parent-Mediated Sexuality Education for Children With ID
As an individual with ID would need additional support to explore sexuality and relationships; sexuality education needs to be an integral part of parenting/caregiving. It is important that it is delivered in a way that a child with ID can understand. It need not wait till adolescence. Explaining complex topics to young children by mere use of words may not be developmentally appropriate, which is even more relevant in children with ID. Depending on the nature and needs of an individual child and task being taught, techniques such as chaining, backward chaining, shaping, modelling, and so on, are employed. Use of art or play as a medium is not only appealing but also simplifies both the content and context. Visual medium has been used in evidence-based practices. For example, Picture Exchange Communication System (PECS) based on applied behavioral principles is primarily visual. It not only improves functional communication in children with speech delay 16 but also helps in teaching socialization and modifying behaviors in neurodevelopmental disorders such as autism. 17 We broadly discuss various means of using visual medium to educate children with ID about sexuality. While we provide a framework for the same, it is also up to the parents to explore and modify methods to meet an individual child’s needs. One can also consider professional help if a person needs further training and support.
General Principles
The interactions should be kept developmentally appropriate. As much as there is a need to have a discourse to normalize sexuality, there is also a need to titrate discussions by not divulging too many details. How much information one can give depends on the child’s curiosity and readiness and parental beliefs. Therefore, one must strike a balance between being evasive and divulging excess information. It is always helpful to address a child’s doubts by first clarifying the question and giving a simple answer. Day-to-day contexts such as a relative’s marriage, friend’s pregnancy, how to conduct oneself at a bus-stop or a restaurant, and so on, can be used to discuss and share information. Also, parents need to model appropriate behavior by asserting their own privacy. 8 Adequate stimulation is immensely important. A lack of stimulation can in itself produce behavioral problems including sexually inappropriate/maladaptive behaviors including self-stimulation. Therefore, adequate engagement of children as per an individual child’s interests and abilities cannot be understated in this subgroup of population. Challenging behaviors when present may have to be addressed first before teaching acceptable behaviors.
Broad Constructs of Parent-Mediated Sexuality Education
To address the felt needs of caregivers and unmet needs of children, we propose a model to explain the “What, Why, and How” of five constructs viz. understanding human body parts, hygiene and self-care, privacy, social skills and handling feelings, and safety (Figure 1).
The Five Broad Constructs—“What, Why, and How Model”

Children have the right to know about their own bodies. Children can feel comfortable with their bodies. Babies, young toddlers, and preschoolers are curious about their bodies and tend to explore their genitalia as naturally as they explore their noses and ears. One must remember to refrain oneself from using slang words or other names and use scientific names such as “penis,” “scrotum,” “testicles,” “vulva,” and “vagina.” This will instill a sense of comfort to use these terms freely. If a child does not know about this from one’s own parents, they will learn from other sources that may or may not be reliable. Children need to be aware of how their bodies look and feel, so they can report to trusted adults when they perceive any change or experience any problem.
Teaching Human Body Parts: (A) Anatomical Body Parts; (B) Parents Using Dolls to Teach Body Parts; and (C) Pictorial Depiction of a Peg-Board

To prevent infections. To help a child become self-sufficient and self-reliant in future.
Visual Schedules: (A) Brushing; (B) Menstrual Hygiene; and (C) Bathing

Children with ID lack the ability to differentiate between public and private spaces/behaviors. They find it difficult to comprehend the “do’s and don’ts” of masturbation unless explicitly taught. They are at risk for inadvertently being charged with an offence. One may have got a message that any sexual expression is unacceptable.
Flashcards for Public and Private Spaces: (A) Public Places and (B) Private Places

Children with ID are social and like to have friends but may find it difficult to communicate their feelings with others. One may lack the ability to understand a situation or body language of others.
Flashcards for Emotions: (A) Smileys and (B) Faces

Every child has the right to feel safe. To prevent exploitation. Children with ID are at a higher risk of being exploited. They may be dependent on others for their activities of daily living, which puts them in a vulnerable situation. They often lack the ability to protest or assert themselves. Sexual abuse is less likely to be reported due to their limited ability to comprehend and communicate.
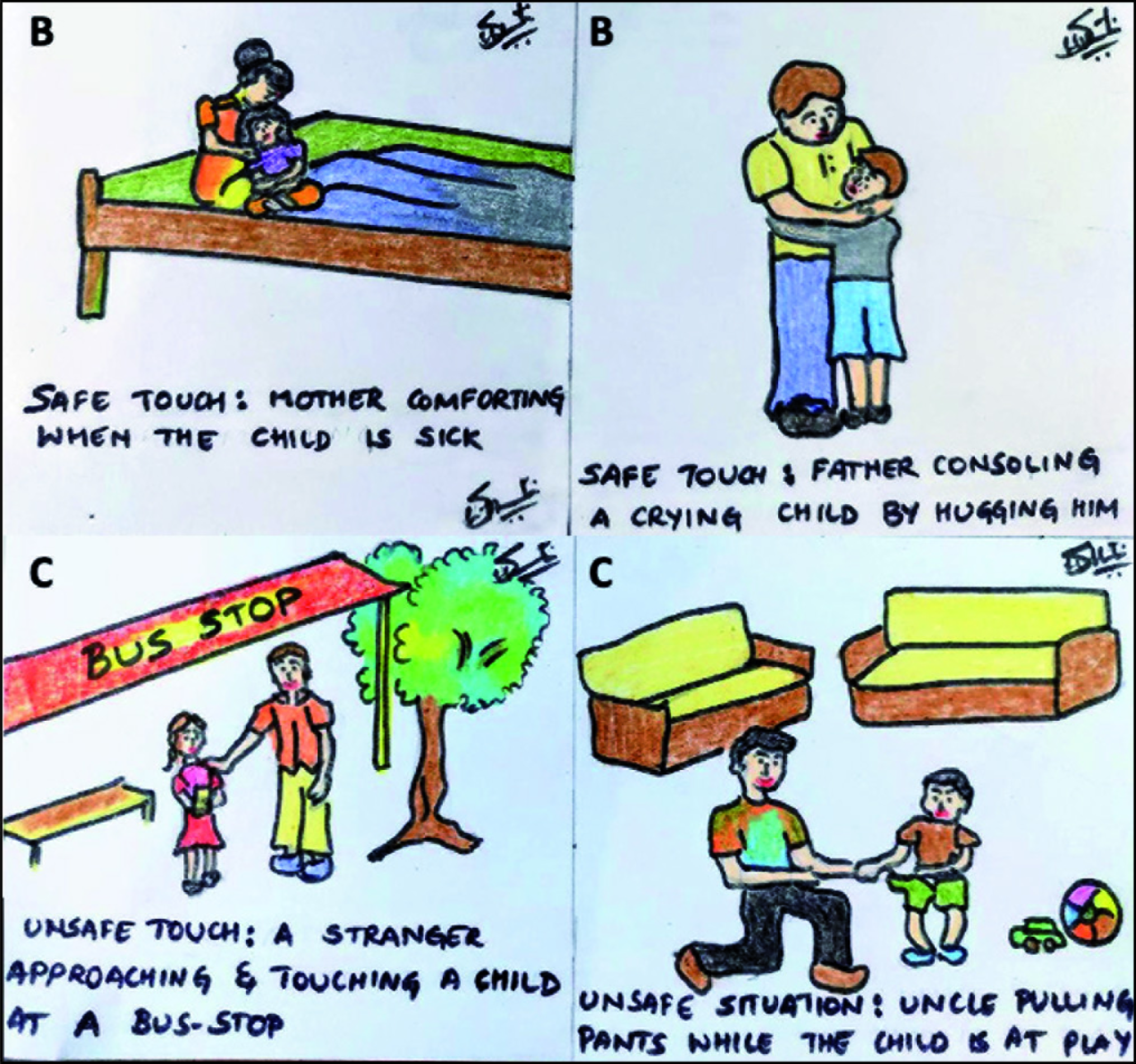
Flashcards for Unsafe Touch

Flashcards for Safe and Unsafe Situations: (B) Safe and (C) Unsafe
Conclusion
There is a need to enable young people with ID to make informed decisions about expression of their sexuality and forming interpersonal relationships. A person-centered and collaborative approach wherein families are fully involved will ensure development of positive sexual identities and reduce risk of sexual harm. Educating parents about sexual health needs should be given as much importance as educating them about self-help-skills and adaptive functioning. Emphasis should be laid on starting as early as possible when they start teaching children about body parts and toilet training, so that eventually it will ensure smooth transition during adolescence. This approach works as a preventive and promotive strategy rather than a reactive one. It also makes it less stressful for parents during adolescence and gives clinicians an opportunity to focus on other comorbidity (if any). Therefore, assessment of sexual development should come naturally to the treating team along with evaluation of other domains such as cognitive, speech and language, motor, and emotional. This will serve as the first step toward reducing stigma surrounding the topic. More importantly, it will help to identify underlying issues and ensure appropriate development. Hence, there is a need to promote contextually relevant sexuality education.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.