
Abstract
There have been several myths and misconceptions about the dichotomous understanding of sex and gender. While sex is biologically determined, gender and gender identity depend on childhood experiences, upbringing, social expectations, beliefs, family environment, and peer interactions and is socially constructed. Gender dysphoria (GD) is the extreme distress experienced by an individual because of a mismatch between their gender identity and the sex assigned at birth. GD has been an ambiguous category in psychiatry, initially termed as “gender identity disorder” till Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) considered removal of the term “disorder” to reduce the stigma associated. The critical element in GD is “clinically significant distress” that differentiates it from gender nonconformity. Individuals with GD identify themselves as transgender and frequently are victims of coercive social norms, discrimination, and stigma. This leads to delay in expression of distress, psychiatric mismanagement, and high comorbidity of depression, anxiety, post-traumatic stress, self-harm, and suicidality. Though management involves a holistic multidisciplinary approach including psychotherapy, social support, and gender-reassignment treatments (medical/surgical), there has been considerable debate and ambiguity related to the same. With this background, the article critics the understanding of GD, focuses on the WPATH SOC-7 treatment guidelines, and highlights the role of mental health professionals for better care.
Introduction: Concepts of Sex and Gender
There is no gender identity behind the expressions of gender… identity is performatively constituted by the very “expressions” that are said to be its results.
—Judith Butler 1
The words “sex” and “gender” are used interchangeably by those who do not see the underlying complexity gender holds. Until a few decades ago, sex and gender were synonymous, and it was assumed an assigned male to be masculine and vice versa. But not later than later part of the 20th century that clinicians observed increasing levels of those dissatisfied with their assigned sex, cross-dressing, and preferences for various activities assigned to the opposite gender with increase in the number of children and adolescents who question conventional gender expectations and seek recognition. 2 This intrigued researchers to study this further. Then came the concept of nonbinary gender. In this article, we discuss about gender alone and not about orientation (the sexual desire toward same and/or opposite gender).
The word “sex” refers to the genetic makeup, that is, XX—female sex, XY—male sex, and is usually assigned at birth after examining the external genitalia. Sex is determined by chromosome, hormones, external genitalia, and other physiological characters. Sex is an ascribed status that one is born with and makes a person a male or a female. 3 An anomalous development of the genitalia results in intersex, that is, a person born with both male and female, internal, or external organs. These come under the category of disorders of sexual development (DSD). 4 Some common syndromes that are classified as DSD are Turner syndrome, Klinefelter syndrome, Swyer syndrome, and more than 30 other conditions under this category.
The concept of gender was recognized as an offshoot of sociological theories and feminist movements. Gender cannot be measured, it is not dichotomous but a scalar and men and women both can fall on the same points of the scale. 5 Gender is defined as an achieved status as opposed to sex that is an ascribed status, and is constructed through psychological, social, and cultural means. 6 Sex is biologically determined and stable across one’s lifetime and across cultures whereas gender is dynamic and psychosocially developed and culturally shaped. 6 Gender is categorized as cis-male/female, trans-male/female, queer, agender, and others. The understanding that males are masculine and vice versa has become universal assumption as “normal” and not being so as “abnormal,” and we describe this along with concepts of gender identity and gender roles in detail in the next section of the article. The concept of gender is ever changing since and the time when we will embrace it as a choice is much farther from where the current understanding stands. And with this, we only see the “tip of the iceberg”—problem of equating gender and sex. How something so different can be synonymous!
Social Construction of Gender
Gender lore surrounds us from the time we are born. It is present in all conversations, discourse, humor, and conflicts we witness. The whole concept of gender is being discussed and reviewed in different lenses because we live in a society that has set norms and expectations. 7 The social constructionist model of gender, sex, and sexuality originated around 1970s as an offshoot of feminist and sociological theories. 8 Unger 9 defined “those characteristics and traits socio-culturally considered appropriate to males and females,” and gave the terms masculinity and femininity. Through understanding these theories, gender is considered a “status” or a “role,” which when achieved is seen as a virtue and falling short of meeting the needs of the role as an abnormality. Social constructionist theorists observed that the status of gender is achieved usually in early childhood. A few theorists like West, Zimmerman, and Fenstermaker also supported the process “doing” of gender. 6 West and Zimmerman 6 described the process as, “Doing gender involves a complex set of socially guided perceptual, interactional, and micropolitical activities that cast particular pursuits as expressions of masculine and feminine ‘nature’.” They also observed gender to be performed in social interactions which are then assessed based on the socially acceptable concepts in their cultural setting. Judith Butler in lines with “doing” introduced the concept of gender performativity. 1 Gender performativity means that a person has ways they talk, walk, and do activities (also known as deeds) and these deeds are gendered and differentiate men from women. The person does not perform these deeds, but the deeds imply what the person is.
The World Health Organization defines gender roles as “socially constructed roles, behaviors, activities and attributes that a given society considers appropriate for men and women.” 10 It is conceptualized as the functional position achieved as a part of “doing gender.” They are also social constructs that can vary with culture, time, and context. 11
Gender identity is a term used for the perceived sense of maleness and/or femaleness of a person. 12 It can be same as the assigned sex or different—opposite (transgender), both (bigender), or neither (agender), or various combinations of the above. It is difficult to understand how the perception of oneself, which is biopsychological, can also be socially constructed and influenced by culture. It is just like in all other spheres we understand that no “nature” exists without a social context, and no societal system exists without nature. 13 The gender identity of a person elicits certain behaviors which may or may not be accepted by the society as normal for the assigned sex, and this is what is experienced by a person of transgender identity as falling short of attaining a “status” which has implications on their mental and social well-being.
Just as we understand gender roles and gender identity, it is very important to understand the consequences of such strictly defined social constructs. Here, arises the vital question as to why people are not judged by their choice of music, movies, or sport interests as choices and why based on gender identity? We understand that every person can have a different choice, but gender is assumed to be a socially defined status that is normative and must be met. The beginning of which is seen from birth where the stereotype girls with pink, and boys with blue clothes, room décor, and everything they use also represents their gender. Subsequently, girls are given dolls, cookery games, while boys are given cars, bikes, racing games, and so on. Similarly, at every stage the clothes they wear, mannerisms, activities, and opportunities are defined primarily by their sex (not gender). Hence, when the gender expression of one is different from that of the socially expected “normal,” there is difficulty in assimilating that fact for the family and near ones leading to shock, denial, and conflicts to the extent of disowning a person. Socially constructed and normative gender roles add on to the theory of essentialism 14 and bolsters it. 6 As gender can be done, there also came theories of undoing 15 which are not extensively studies, but the concept of redoing is understood to some extent. Theorists have looked at how gender is a socially constructed phenomena, but not at how this rigid division upholds sexism and maintains gender inequality which forms the basis for feminist and transgender movements. The concept of unveiling or exploring gender is far from where we stand now.
It is of utmost importance to note the difference between those with gender dysphoria (GD) and transgenders. When an individuals’ gender identity is not the same as their assigned gender is, gender incongruence and the extreme feeling of distress due to this is known as GD. Those with GD are distressed by their assigned sex, secondary sexual characteristics, and social gender roles and experience distress at various levels. 16 Transgender is an umbrella term that encompasses those with distress, desire, or are in phase of transition to the other gender.
History, Origin, and Features of GD
Transsexualism has been present since the advent of human civilization and in mythological stories across cultures. In Indian mythology, Mohini (Lord Vishnu’s avatar), Ardhanarishwara (an amalgamation of Lord Shiva and Parvati), in Greek Mythology Hermaphroditus (a two-sexed child), and so many others have been described extensively. Shikhandi (known to be a transgender) is a central role in the Indian epic Mahabharata, known for the role in battling and defeating the legendary warrior Bhishma. The mythological concepts and their connotations are beyond the scope of this article.
Historically, the concept of people who wanted to become/live like a person of the other sex was viewed as pathological, and first described by Kraft Ebbing in 1886 as “metamorphosis sexualis paranoia.” 9 Similarly, in the 19th century, psychiatrists and medical fraternity often confused transsexuals with homosexuality, and described them as “man trapped in a woman’s body” and vice versa. A strong binary division was noted. In 1923, Magnus Hirschfield was the first to distinguish between homosexuals (those who desired partners of same sex) from transgenders (those who identified with the opposite gender). 12 However, there were discussions and debates but no consensus over these ideologies. The first documented case that underwent sex reconstruction surgery was Jorgensen, later came to be known as Christine (a transfemale). Following this, the medical fraternity gradually came to understand this better and later terms like gender identity, cross-over, gender expression, and gender roles came into popular use. There was high resistance from the side of varied health professionals to adapt to a then-new concept of a new gender. It was only in the 21st century that the concept gained clarity and medical, social, legal, and ethical needs of this population have come to light and are being supported.
The term “gender dysphoria” first came into the diagnostic systems in DSM-III, 17 where it was called “Gender Identity disorder (GID)” with three specifiers—transsexualism, GID in childhood, and atypical GID. In DSM III-TR, they added another specifier namely GID in adolescence or adulthood. The discussions revolved around the need to understand if GID was present in childhood would persist in adulthood. This theory remained inconclusive, noting children do change their gender identity, or understand about sexual orientation which become clear during adolescence or young adulthood. In DSM IV and DSM IV-TR, it was reclassified as GID in children and adolescents under the parental category of sexual and gender identity disorders. In DSM 5, 18 GID was replaced by “gender dysphoria” with specific categories of GD in children, GD in adolescents and adults, and was separated from other sexual disorders and paraphilias. The term “disorder” was removed as it was associated with stigma and marginalization. GD is the distress an individual undergoes based on a mismatch between their gender identity and assigned sex at birth. They commonly identify themselves as transgenders. Based on the American Psychiatric Association, GD is associated with “clinically significant distress” and hence different from gender nonconformity. 19 The causes can be multifactorial ranging from genetic, environmental, and sociocultural factors, the detailed discussion of which is beyond the scope of this article.
International Classification of diseases (ICD) version 8 was the first to have the diagnosis of transvestitism, the terminology though not very clear, by most is understood to be transsexualism. In ICD-9, the term transvestism replaced the previous terminology and had a specific exclusion for transsexualism. In ICD-10, a clear place for classification of transgenders was given as GID (F64) under the parental category—disorders of adult behaviors and personality which included transsexualism, dual-role transvestism, GID of childhood, other GIDs, and GID unspecified.
It is very hard to report the exact prevalence of transgender individuals in the population. Most studies are based on the number of people who approach for medical interventions. It should be borne in mind that a large number might not want medical interventions and would hence be excluded from the prevalence studies. The most recent epidemiological study and review about transsexualism reports prevalence ranging from 1:11,900 to 1:45,000 for male-to-female (MTF) persons and 1:30,400 to 1:200,000 for female-to-male (FTM) persons, 20 with an increasing number of patients seeking assistance in the recent years. 21 As in DSM-5, the prevalence of GD is 0.005% to 0.014% for adult natal males and 0.002% to 0.003% for adult natal females. 22
With reference to DSM-5, GD is further classified based on the age of onset as GD in children and GD in adolescents and adults. GD in children is usually suspected when there is strong desire/insistence to be of the other gender, resistance to wear clothes of assigned gender also seen as cross-dressing, strong preference for toys, games and activities of the opposite gender, taking up roles of opposite gender in fantasy play, and strong preference of playmates of opposite gender.18,23 GD in adolescents and adults manifests as strong incongruence between the assigned and affirmed gender, increased distress to development of primary and secondary sexual characters of assigned gender (wish even to get rid of them), strong desire to have primary and secondary sexual characteristics of affirmed gender, and strong desire to be treated as per their affirmed gender. 24 One should also bear in mind to specify if it is due to any DSD or if the person is in post-transition phase. Significant impairment in socio-occupational functioning can be observed. Sexual orientation has not been consistently linked to GD. However, transwomen who have late-onset GD are usually sexually attracted to women and possibly identify themselves as lesbians. This happens vice versa with their male counterparts. Also, individuals with male sex at birth who have late-onset GD may engage in cross-dressing for sexual excitement which needs differentiation from true transvestism in which there is no “distress” with the biological sex. 25
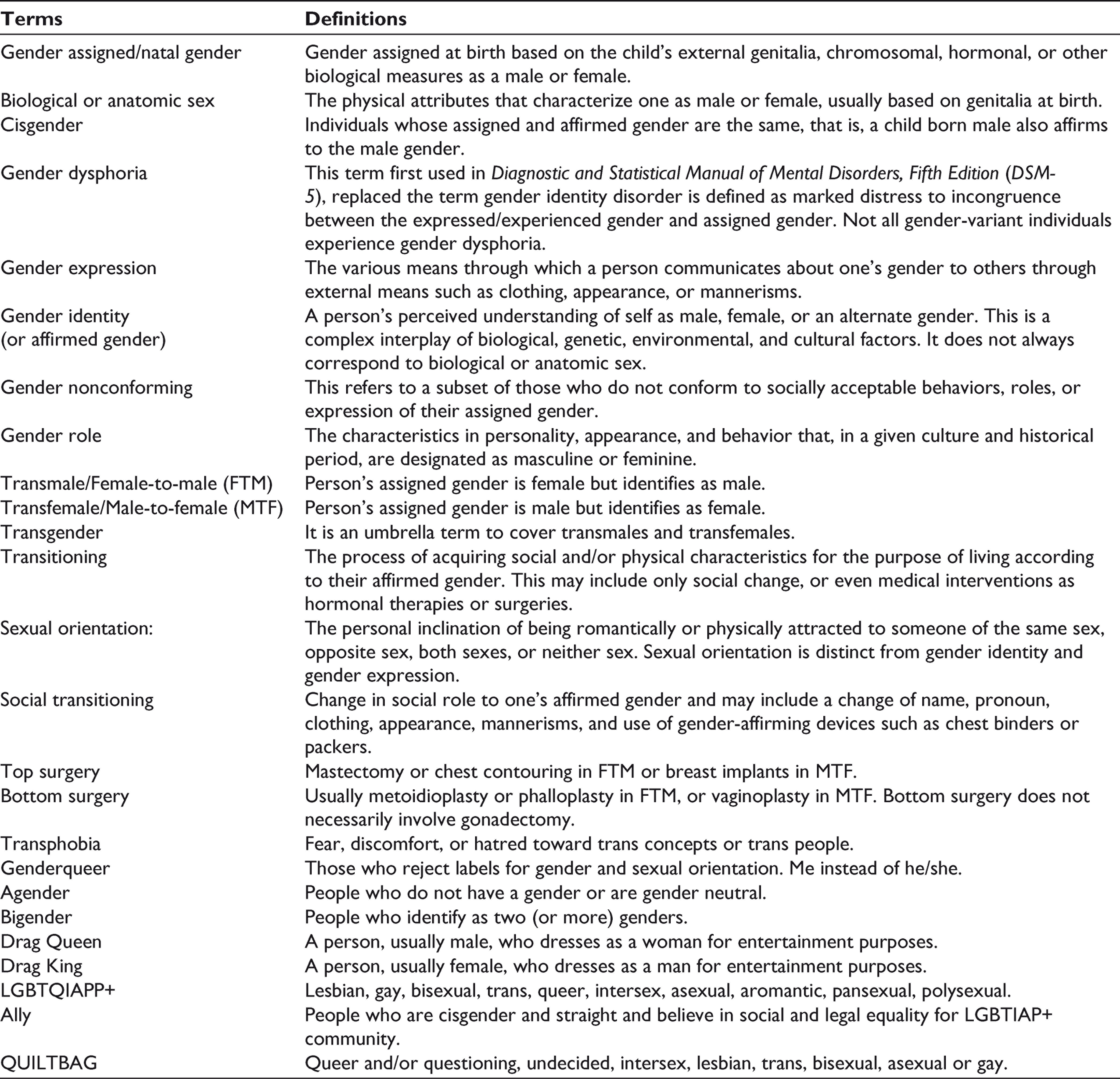
Public understanding about GD continues to be dismal and various myths and false beliefs exist in society regarding this condition, which are highlighted in Box 1. Various commonly used terms related to gender minorities and GD are defined in Table 1 for better clarity.
Common Myths Associated with Gender Dysphoria
Gender dysphoria and homosexuality are the same.
Children cannot take a stance on gender identity as they cannot understand.
It is a phase and will pass.
Children grow out of the dysphoria with age.
Gender identity is fixed and inflexible.
Gender dysphoria is a “fantasy.”
People develop gender dysphoria to gain attention.
Young individuals with this condition are “damaged” for life.
All those with gender dysphoria will require medical transition.
Gender dysphoria is a mental illness.
Gender dysphoria only happens in certain groups, ethnicities, and cultures.
Gender dysphoria inevitably needs sex-reassignment treatment and can be “cured” by the same.
Common Terminologies Related to Gender Minorities and Gender Dysphoria
People who experience GD have increased distress in understanding their gender expression and are having a constant internal conflict in identifying themselves within the stereotyped, binary male or female roles in the society which cause cultural stigmatization. This leads to interpersonal difficulties with family, peers, friends, rejection from society, symptoms of depression and anxiety, eating disorders, substance-use disorders, a negative sense of well-being and poor self-esteem, loneliness, and an increased risk of self-harm and suicidality.26,27 Children with early onset GD can suffer from significant distress with their own genitalia, strong preference for playmates of the opposite sex, social isolation, peer rejection, and poor coping with stress. 28 The common myth that people “grow out of it” after childhood is further damaging and can lead to self-stigma, delay in diagnosis, mismanagement, and concealment of symptoms.
Psychosocial Dimensions in People Living With Transgender Identities
One of the most important psychological issues faced by those with GD and/or transgenders is of a disparity between the experience of self and expectation of the society which is distressing. 29 This disparity leads to low self-esteem, guilt, and anxiety. In India, transgenders are usually referred to as “Hijras.” They experience stigma because of labelling “gender policing” from family and society they live in and face trauma of being misgendered. 8 Feeling stuck between needs of oneself and the social demands creates confusion and is a high risk for developing anxiety, depression, and other mental illnesses. In addition, self-harm, suicidal ideations, eating disorders, 30 autism spectrum disorder, or autistic traits31,32 have been studied. There are multiple dimensions in which individuals with LGBTQI identities face discrimination, prejudice, and social stigma. A detailed review of all these factors is beyond the scope of this article. Here, we only provide a brief overview of these social challenges.
The transgender population is segregated from the “normal” population and is also segregated from lesbian gay and bisexual (LGB) community, making them a minority within a minority. The Minority Stress Model explains the experience of stigma leading to high prevalence of psychiatric comorbidities. 33 This model further extended to identify a high rate of victimization, discrimination, exposure to transphobia, and internalized stigma as predictors of psychopathology.34,35
At a macro level, there are systemic challenges they face and it leads to exclusion/isolation, unemployment, difficulty participating in social, and cultural events, which is distressing and further negatively impacts their quality of life. 29
A very important psychological challenge is on the end of health care professionals, who tend to have little understanding of GD and the impact it has on an individual person. We inherently are tuned to distinguish between males and females and do not ask, “What is your gender?” It is rather a simple question that could make a help seeker comfortable, feel understood, and enable further access to health care. This would further facilitate cooperation for assessment—clinical history, appropriate and focused examination, and necessary investigations. Increasing awareness, sensitivity, and our own understanding is imminent in this era.
Understanding further, the gender-based discrimination, sexual stigma, gender stereotypes and gender-based inequalities compounded by inadequate understanding and misinformation, and preexisting social vulnerabilities lead to “othering” and minority stress. This is further complicated by the current COVID-19 pandemic situation. 36 In a recent review, Banerjee and Nair 36 have highlighted these psychosocial challenges of the transgender individuals during the ongoing pandemic both using the “minority stress” hypothesis as well as the health-stigma-discrimination framework. Othering based on gender minority and social stereotypes are related to the minority stress and discrimination, which in turn have multifaceted adverse consequences during the COVID-19 crisis and uncertainty. It can be conceptualized that individuals who have GD also have issues with their social identities and can possibly face similar challenges during any form of persistent crisis.
Ambiguity in Management of GD: Revisiting the WPATH Standards of Care (SOC)
The concept of GD has rapidly transformed into the understanding we have today. The various ethical, legal, and human rights perspectives have to be considered before framing treatment guidelines. The current guidelines World Professional Association for Transgender Health—Standards of Care Version 7 37 is predominantly in use. To bring out a first point, the SOC-7 was released in 2011, that is, 9 years from now. In such a rapidly changing research area, the relevance and changes over 9 years are currently almost not adapted or investigated. There is a dearth in research in this area as well, and access to care is better in the West as compared to the Eastern world. The SOC-7 speaks about depathologizing GD but insists on mentioning the diagnosis on the referral letter for interventions. A need for having a diagnosis to access care has been debated by many. 38 The conceptualization of gender nonconformity as nondistressing and distress in GD to be related to stigma and “minority stress” is confusing to people trying to understand the guidelines.
There have been some major changes like removing the informed consent model, using depathologizing terminology (except in reference to intersex section), cultural sensitivity, removal of the term real-life experience which now is living a gender role in congruence with gender identity. But, the duration of 12 months, continued care under the support of a mental health professional (MHP), seems to give more power to the MHP than the transindividual and increase the distress experienced, which might be a concern. Also, there is no logical explanation for why the time duration is 12 months, not more or less (as above). The plausible explanation is that hormonal therapy and surgical procedures are partially or completely irreversible, respectively. Although the guidelines have been modified for the better as compared to the previous versions, it still lacks adequate scientific evidence.
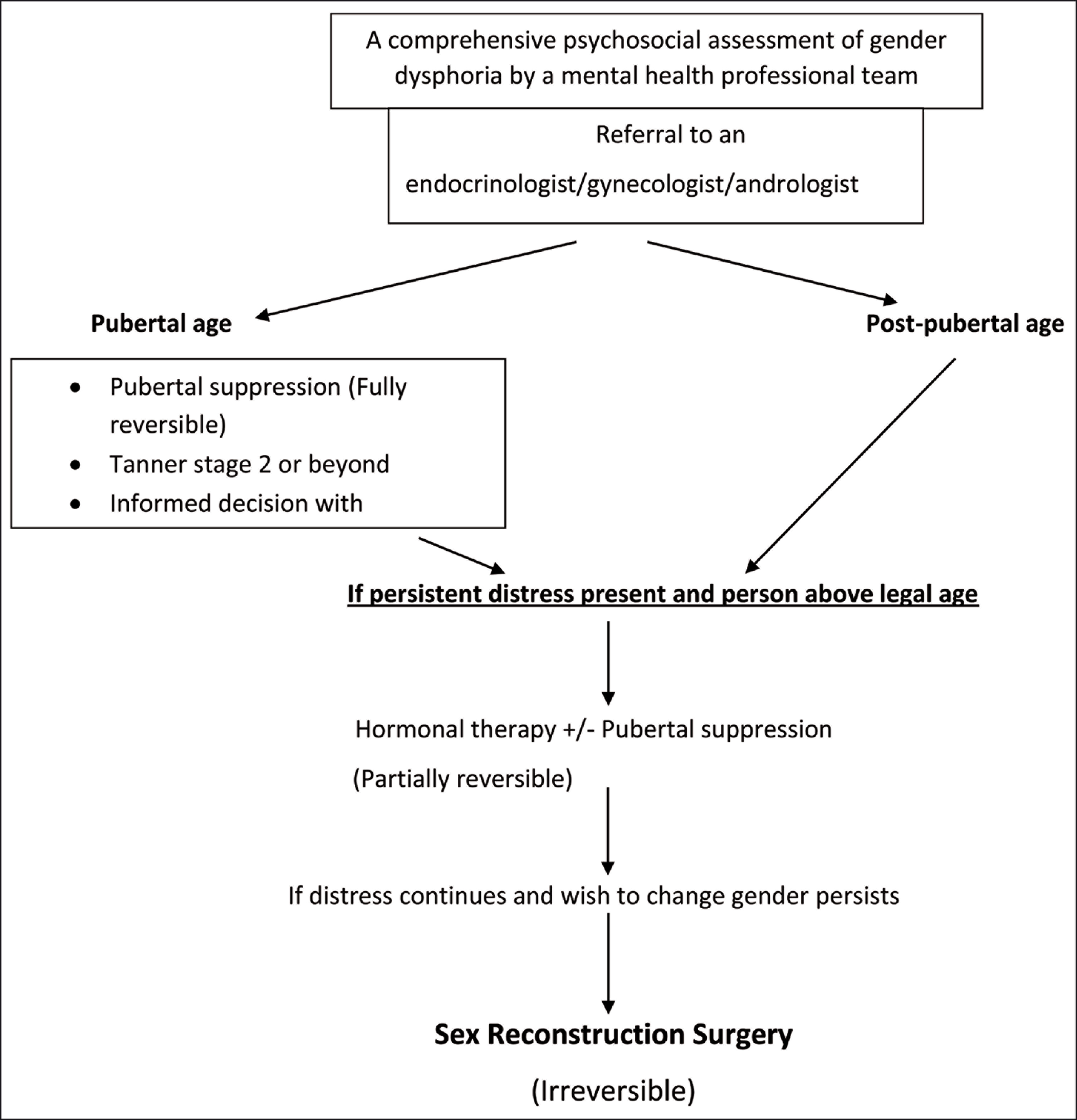
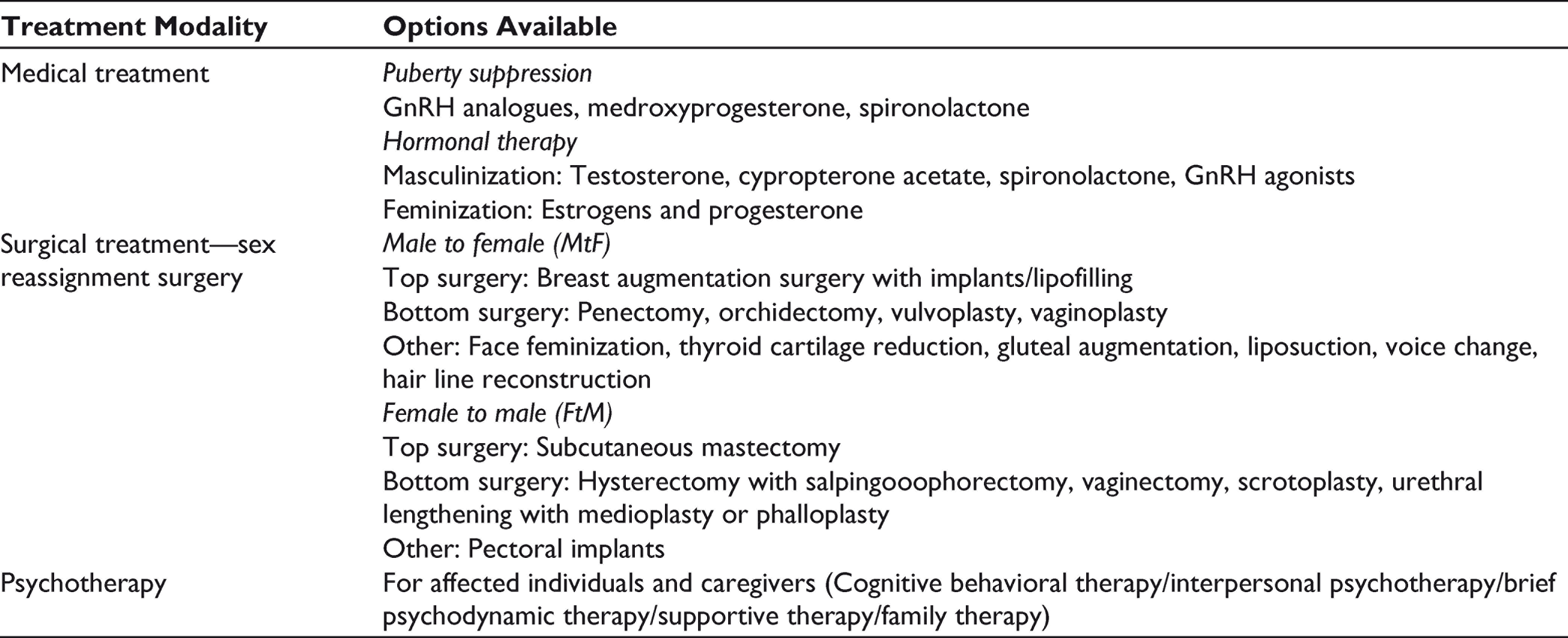
There are no other prerequisite criteria to undergo psychotherapy. There is a need to be diagnosed with GD, ability to make an informed decision for hormonal therapy. For surgical procedures, the top surgery requires referral from one MHP. Bottom surgery requires referral from two MHPs after living in a gender role congruent to gender identity. 19 Any preexisting physical or mental condition should be treated and be under good control before initiating hormonal or surgical therapy. The role of MHP is given prior to, during, and after any therapy and sometimes a continued process. It is very important for everyone to understand that GD will not require medical intervention, and among those who require medical intervention not all will undergo surgical procedures. Gender identity is unique while some might be happy with a voice change, or breast augmentation, while some might opt for complete surgical transition. This should be individualized on a case-to-case basis to fit the needs of the person. Besides, it is vital to appreciate that the management of GD is not all about psychoeducation and sex-reassignment treatment. The perceived consequences of gender change, social acceptability, and living with the changed gender identity are more important concerns which influence the quality of life and decide the prognosis of management. Hence, continued and comprehensive psychosocial support along with periodic are necessary for reintegration into the society and reestablishment of a new identity. Figure 1 provides an overview of the treatment regimen. Table 2 provides the various medical and surgical treatments that are available for the management of GD.
Evidence-Based Treatment Options Available for Gender Dysphoria
Crucial Role of the MHPs
The role of a MHP (psychiatrist, psychologist, psychiatric social worker, and others) as a part of the multidisciplinary team is required at all stages in the care of GD. Some of them have been discussed briefly below. The prime approach is to be open, nonjudgmental, and acceptant toward the person. The MHP needs to be thorough with the clinical skills of active listening, empathy and knowledge of psychosexual medicine be able to come to a diagnosis (as it stands today, and not as a form of pathologizing) of GD. The MHP also needs to be able to screen for any comorbid psychiatric conditions, psychosocial vulnerabilities to be able to identify high-risk factors for self-harm and suicide. It is better to ascertain that the GD has been persistent and not a product of psychosis, mood disorder, or obsessive-compulsive disorder. The assessment in people who have not explored their gender identity would take longer, where the MHP should assist the person in exploring their gender identity. 37 The role of MHP is also imminent in coming out, discussing with family, and discussing various treatment and fertility options. 38 There is an important point to be noted that the exploration, social transition, and psychotherapy or pharmacological treatment all go at the pace the person is comfortable with. Cognitive behavioral therapy, interpersonal therapy, brief psychodynamic therapy, supportive therapy, and family/couple therapy have been shown to be effective in the holistic management of GD; however, continuity of care, compliance, and retention in therapy is the challenge. 19 Family therapy and psychoeducation have shown specific benefits in gender-related distress tolerance, informed decision-making for the management decisions, and acceptance of changed gender identity and gender roles after sex-reassignment treatments. 25 The discussion may also touch upon expectations, what are possible outcomes, assess readiness as well. The social and legal perspectives, involving family and near ones to increase support system, should also be looked at. 27 The support should be continued even after gender reassignment or hormonal therapy to assess for any post-treatment dissatisfaction or trouble with adjustment. The continuation of psychosocial care in coordination with the treating physicians of related specialties (endocrinologist, surgeon and others) and other mental health care professionals (psychologist, mental health counsellors, psychiatric social worker, and others) is of utmost importance to help reintegration of the person into the society and in developing and establishing their identity. The MHP should also be aware of the certification process for hormonal and surgical treatments as the person can undergo procedures only upon being certified. 23 Various subspecialties within MHPs have specific roles in this regard. While the psychiatrists can help in screening and early diagnosis of GD, clinical psychologists can formulate the psychotherapeutic plan and engagement of individuals and their families in therapy. Psychiatric social workers have a role to play in community care, awareness, family psychoeducation, and longitudinal follow-up in individuals of GD to improve their quality of live. These responsibilities are often overlapping and a coordinated team effort among MHPs is necessary to debunk medical misinformation related to GD, involve primary healthcare workers in the care, and integrate psychosocial management in the overall WPATH SOC guidelines.23,27,38
Conclusion
Transgender is not a choice, but a state of the body and the mind. Just as we understand varied personalities, gender is also an expression of one’s self. Social constructional models seem very reductionist and tend to further increase discrimination. Gender is a very complex biopsychosocial phenomenon, and its fluidity, changeability, and variations are unravelling, and there are many more than where we stand to understand now. The times have come to understand that gender does not define a person, but a person defines their gender. The debate of medicalizing or pathologizing gender is to be reviewed, if not medicalized it would lead to problems of insurance and health care, which could burn pockets and further increase distress. A movement with medical, legal, ethical, humanistic, and psychological threads holding it is a hard to hold position. There will always be differing views, but the aim should rather be to provide adequate, accessible, and affordable care to those at varied levels or intensities as required, to improve the quality of life of transgender population. Further, there is a need for in-depth qualitative ethnographic and interpretative phenomenological studies to understand the lived experience of people with GD. Research needs to focus simultaneously on studies with good rigor for parenting, interventional, and treatment-related challenges and interventional efficacies. The social stereotypes need to be challenged with a collective responsibility from the individual, community, media, and administration. Only then can be look beyond the “medical model” of GD and improve their psychosocial outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.