
Abstract
Psychoanalysis and psychiatric rehabilitation are two vastly different theoretical concepts in psychiatry which can be used in patient’s interest when the resources are scarce. This case was approached with the objective of studying a case and its management using the psychoanalytic approach towards psychosocial rehabilitation in the low resource countries. A 37-year-old female presented with the chief complaint of stress and severe IPR issues with husband resulting in the socio-occupational dysfunction. Via psychoanalysis, the issues were resolved, and couple was rehabilitated in society with restoration of normal functioning. This study puts forward the concept of applying and integrating psychoanalysis as an approach towards rehabilitation.
Case Study
Mrs S, 37/F, MSc, home tutor for 10th and 12th standard, belonging to a Hindu nuclear family of Middle Socioeconomic status of urban background, was brought by her husband, with the complaints of occasional irritability and weeping spells for about 3 years and had increased in last 1 year. Patient’s husband, Mr A, 40/M, MSc, PHD, working in three institutes, Middle Socioeconomic status, Hindu nuclear family, reported that the patient has depression for 6 months. However, on exploration there was no clinical evidence of persistent pervasive low mood, fatiguability, or anhedonia. There were no negative and bleak views about future and no episodes of self-harm. However, due to the presenting complaints, patient had a breech in normal functioning in the terms of personal, social, and occupational dysfunction. In the personal domain, patient was having decreased communication with husband, nil emotional intimacy, and physical intimacy (no sexual dysfunction). In the social domain, decreased communication with neighbors and avoidance of family gatherings and difficulty taking mutual household decisions was present. The patient did not have any occupational dysfunction was able to provide focussed teaching at work. It was envisaged logical to assess patient’s husband along with her. On exploration, patient’s husband in the social domains had decreased communication with wife, sleep disturbed, nil emotional intimacy, and physical intimacy (no sexual dysfunction). In the social domain there was avoidance of family gatherings, difficulty making deep meaningful friendships, difficulty taking mutual household decisions. On the occupational front, patient’s husband had difficulty managing workload. Thus, it was considered to treat the couple as a unit rather than an individual.
Salient Features in Childhood
Patient
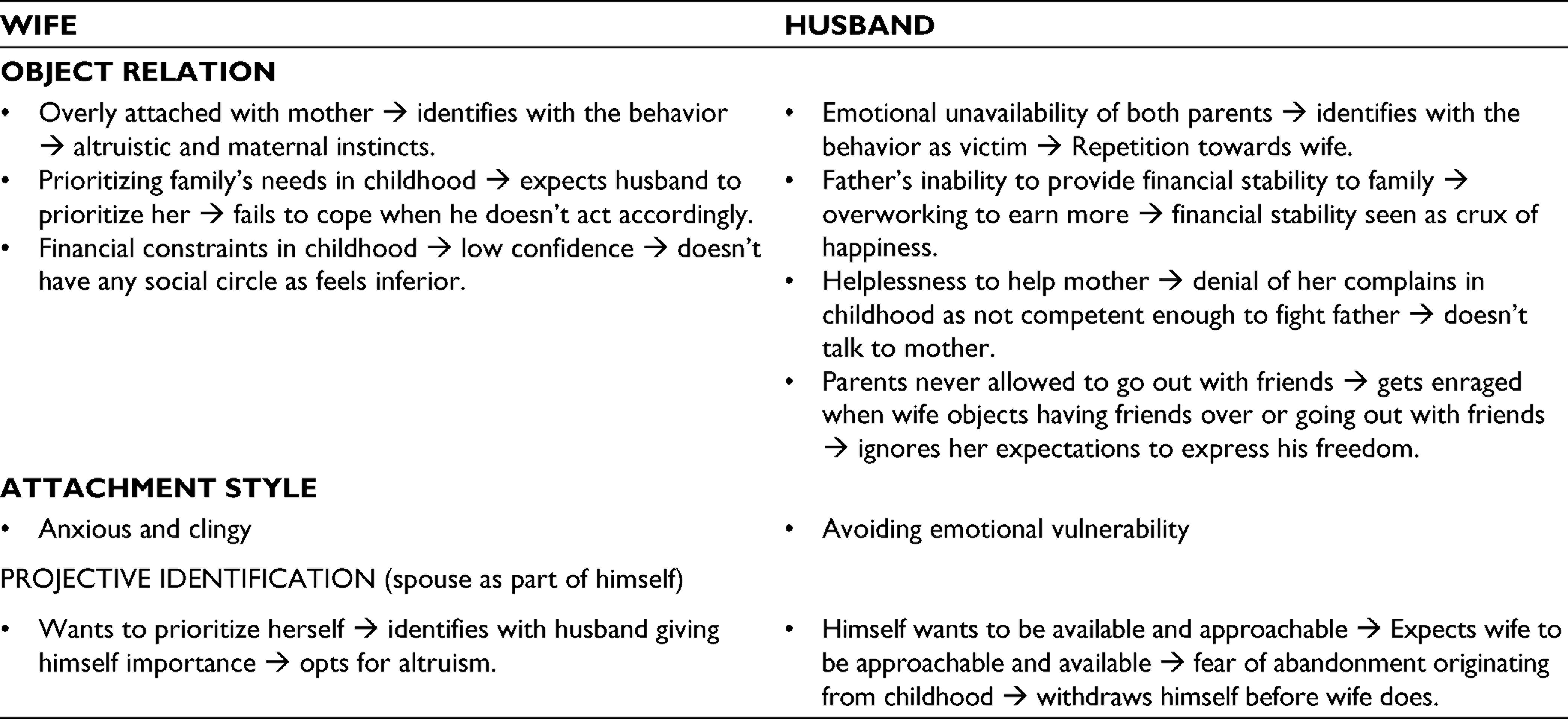
Mrs S was youngest of three siblings and had financial constraints in the family. Having minimal to no friends she was forced to take responsibility at an early stage of life. She had always adopted a sacrificing attitude since childhood, prioritizing everyone else’s happiness and needs. Patient had an over attachment with the mother, and elder brother suffered with opioid dependence.
Patient’s husband
Mr A was grown up in a family with financial constraints, witnessed abuse to mother over financial problems at house, and had experienced childhood abuse (violent father; used to thrash patient and his mother). His parents took all the major life decisions for him and instructed him around not to have friends over or to go out with.
Management
Twice weekly sessions were planned (time duration 45 minutes). Containment and holding (safe space) with technical neutrality (impartial listening) was applied including tracking the change of affect with the context. Interpretations were conveyed using object relations, attachment style, and projective identification. Therapy included working through the patient and husband’s defenses (altruism and suppression in patient and repression, denial, and rationalization in husband). This was followed by ventilation regarding childhood abuse, motivation enhancement in the husband for effective communication with his mother; expectations from husband, frustration of early job in the patient.
Case Analysis of the Couple
Along with that integration of basic couple’s therapy was done that included effective communication, active listening, quality appreciation, conflict resolution, mutual decision making, rekindling exercises, and gratitude expression. Total of 26 sessions were taken, which were a combination of couple as well as individual sessions. At the end of the sessions, wife did not have any complaint of irritability or weeping spells, husband’s communication with spouse and sleep improved, and the couple’s physical and emotional intimacy was restored.
Discussion
Psychoanalysis and psychiatric rehabilitation are seen as two completely different theoretical concepts in psychiatry. It is often forgotten that psychosocial factors are the common link between the two, which impacts the patient’s life in multiple ways. 1 Rarely has this perspective been opted to see how these two schools of thought can be linked in the patient’s interest when resources are scarce.
Usually there is a highlighted difference seen between psychoanalysis and rehabilitation in terms of terminology, clinical practice, and client grievances but the harmony is often forgotten as there is little mutual research evidence, cross-disciplinary research, and few joint journals. It is important to understand that the two disciplines have certain common factors such as the emphasis on subjectivity and importance of relationship patterns and interpersonal context. It is a known fact that subjectivity and psychosocial factors are influenced by social context and in turn affects the insight, coping, response to the illness, and future behavior of the patient.2,3
In this case, at the end of the psychoanalysis, unconscious projective identification was recognized and taken back by both, mutually gratifying intimacy (physical and emotional) was achieved, holding environment created in the sessions was extended to family, capacity to work as a couple in the society restored.
Hence, psychosocial factors that emerged which were hindering their role in the relationship, via psychoanalysis, the issues were resolved, and couple was rehabilitated in society with restoration of normal functioning.
This study puts forward the concept of applying and integrating psychoanalysis as an approach towards rehabilitation, as social and psychological factors of the patient play an important part in his recovery and reintegration into the society. In a resource-constrained country like ours, use of innovative and/or lesser-used non-pharmacological techniques is essential. Additionally, this case adds to the meagre literature existing regarding rehabilitation for the non-severe mental illness population.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.