
Abstract
Background:
Personality psychopathology, substance abuse, family of origin experiences, and patriarchal attitudes are variables associated with intimate partner violence.
Aim:
This pilot study aimed to explore clinical and personality profiles and psychosocial variables in a small cohort of male perpetrators of intimate partner violence.
Methodology:
20 men from informal settlements presenting to crisis counseling centers in Mumbai were administered the Millon Clinical Mulitiaxial Inventory III, the Revised Conflict Tactics Scale Short Form, and the Attitudes toward Women scale.
Results:
Millon Clinical Mulitiaxial Inventory III profiles and scores on Grossman Facet scales suggest personality psychopathology in the profiles of 95% of the men, and 85% reported anxiety. Less than 20% reported substance abuse. The men reported mutuality of violence in the relationship and espoused moderately liberal attitudes toward women. 55% of them reported violence in the family of origin.
Conclusion:
Our findings are helpful in providing therapeutic pointers for working with male perpetrators of violence.
Introduction
Several psychological and sociological factors have been studied to explain intimate partner violence (IPV). Many studies identified that a significant percentage of abusive men show some personality psychopathology.1-6 The Millon Clinical Multiaxial Inventory (MCMI) has been the most commonly used instrument to study profiles of perpetrators of violence.2,6,7 Depression may increase the propensity to engage in IPV 8 and addiction models propose that violence is related to the use of substances, especially alcohol.8-10 Social learning theories of IPV suggest that men learn IPV through modeling, that is, by watching others abuse women (such as witnessing their fathers beating their mothers) and being abused themselves in their family of origin.8-11,12 Gender theories examine the impact of gender roles in contributing to violence.8,13
There has been limited research in India examining factors predisposing men to be violent to their intimate partners.8-10 We work at a nonprofit organization that runs crisis counseling centers for women survivors of gender-based violence. 14 We use a community-based stepped care model of intervention for women that combines sociological and psychological perspectives. 15 Our experience has shown that working with male perpetrators is crucial. 14 We conducted a descriptive pilot study with a small cohort of men presenting at our centers who were violent toward their female intimate partners.
Method
Research Context
The study was conducted at crisis counseling centers for women survivors of gender-based violence in the informal settlements of Dharavi and Malwani in Mumbai.
Ethical Issues
The study proposal was approved by the Ethicos Independent Ethics Committee before commencement. We acquired written informed consent from the participants.
Participants
20 participants were recruited through purposive sampling from among clients attending the crisis counseling, after a review of case sheets. Physical, psychological, and sexual domestic violence definitions were based on the Protection of Women from Domestic Violence Act. 16 Husbands or male intimate partners of women clients who were the primary perpetrators of violence, and were classified as mid-intervention (had participated in around 6 months of regular intervention), were included in the study. Those with severe mental disorders were excluded.
Instruments
Case notes of clients were reviewed. A structured interview was designed that asked about ages, educational levels, income levels, and employment status. 2 closed questions elicited the family of origin experiences: “Have you ever witnessed your father beating your mother in your family?” and “Do you consider yourself to have been physically abused as a child?”
Clinical and personality factors were assessed using the MCMI III, 17 a 175-item self-report inventory that assesses 24 clinical scales (11 personality disorders, 3 severe personality disorders, 7 clinical syndromes, and 3 severe syndromes). Grossman Facet scales are subscales within each MCMI III construct that allow for a more detailed assessment and were found by Loinaz et al to be of predictive utility in understanding IPV. 7 We used a Hindi translation of the test that is in the process of being standardized. The level of violence was measured using the revised Conflict Tactics Scale—Short Form (CTS 2S) developed by Straus and Douglas. 18 The short form of the Attitudes towards Women Scale (ATWS) of Spence et al 19 was also used, on which a high score suggests egalitarian beliefs, while a low score reveals traditional, sexist beliefs. The instruments were translated into Hindi and back-translated by 3 independent subject and language experts.
Results
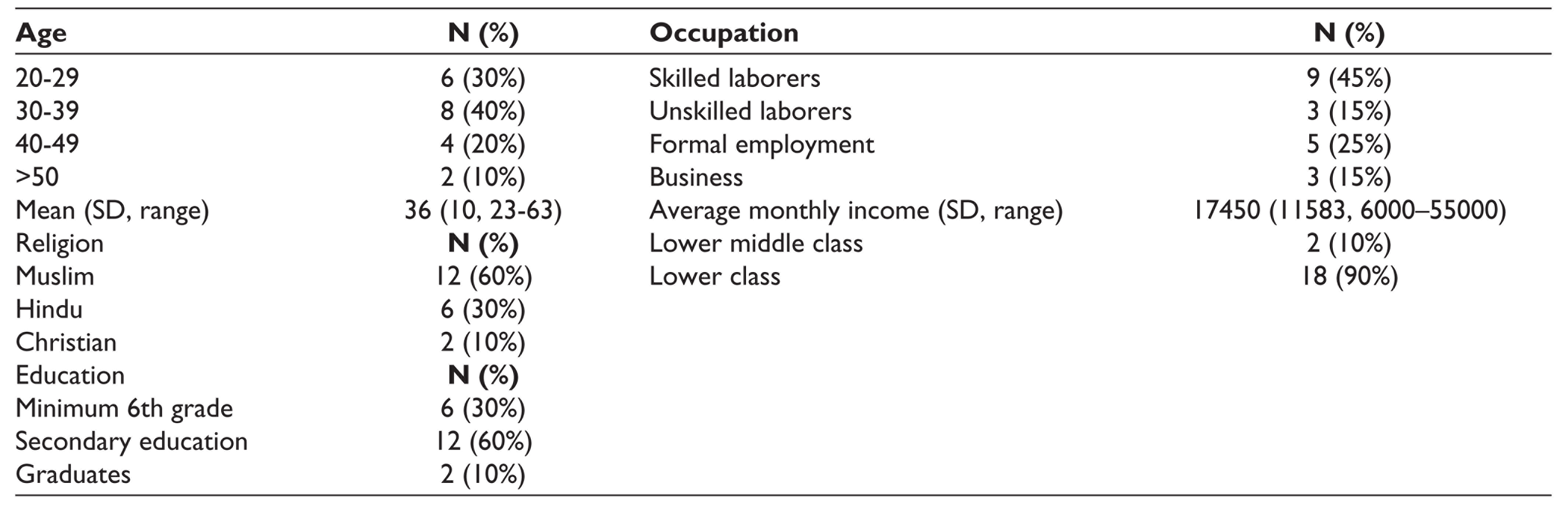
Demographic details of the sample are represented in Table 1.
Demographic Details of Participants
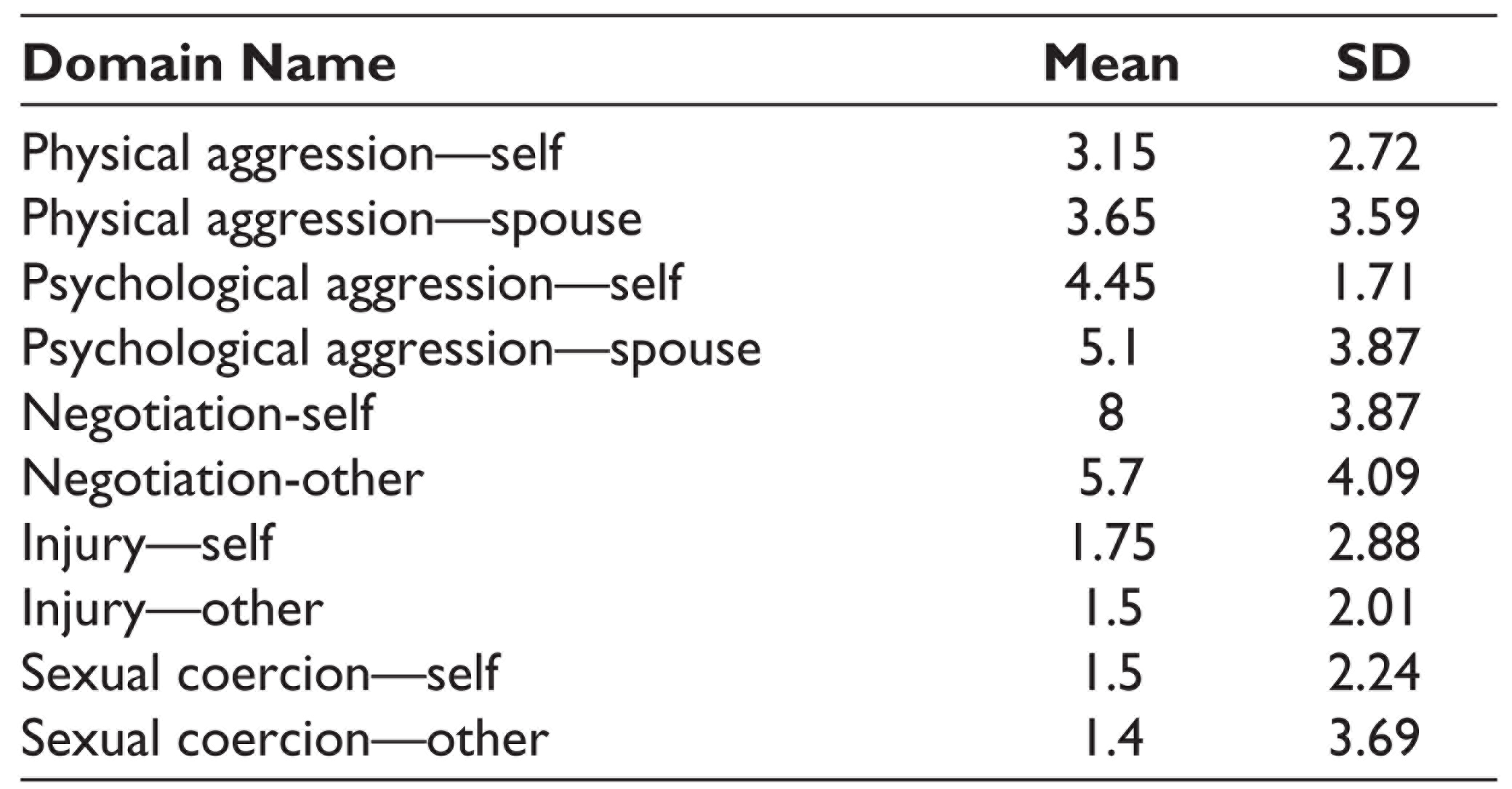
Scores on the Conflict Tactics Scale 2S are shown in Table 2. Men reported that they most frequently used negotiation to resolve conflicts, and that their wives showed higher levels of physical and psychological aggression than themselves.
Means and SDs of Scores on the Conflict Tactics Scale 2S
55% of the participants reported experiencing abuse in their childhood by their family members, and 55% reported witnessing domestic violence in their families of origin.
The mean score on the ATWS was 40.6 (SD = 14.24, range = 16-67).
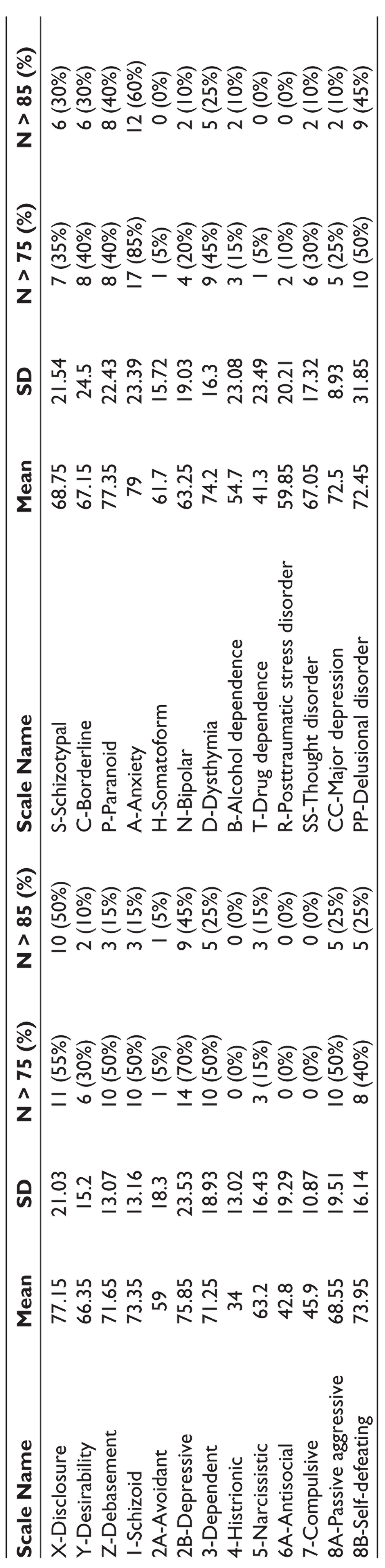
Scores on the main scales of the MCMI III are reported in Table 3. 90% of the profiles were valid and 10% were of questionable validity. Disclosure was high. 95% of the men had at least one scale elevated amongst the Clinical Personality Patterns and Severe Personality Pathology scales, suggesting the presence of personality pathology amongst almost all the samples. Most prominent scores were on paranoid, depressive, self-defeating, schizoid, and dependent personality disorders.
MCMI III Profiles—Means and SDs of BR Scores on Clinical and Personality Scales
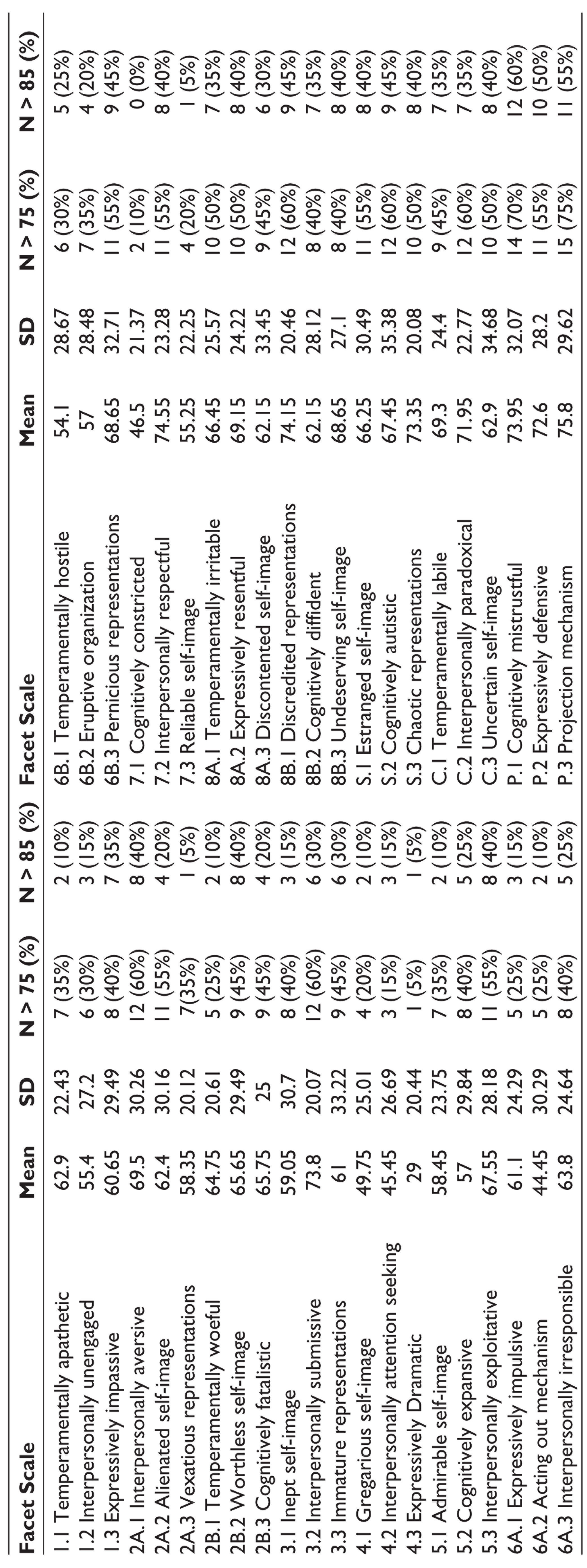
Scores on Grossman Facet scales are shown in Table 4. The most prominent Grossman Facet scales were found to be P.2 Projection Mechanism (disown personal undesirable attributes and projecting them onto others), P.1 Cognitively Mistrustful (hypervigilant, suspicious, convinced that one is being or will be unfairly treated and interpret benign events as evidence for the same), P.3 Expressively Defensive (vigilantly guarded and resistant to external sources of influence and control), 7.2 Interpersonally Respectful (scrupulously adhere to social conventions and propriety), 8B.1 Discredited Representations (object relations consist of failed past relationships), S.3 Chaotic Representation (confused internalized representations of early relationships), 3.2 Interpersonally Submissive (subordinate self to authority figures and fearful of being left to fend for self), and C.2 Interpersonally Paradoxical (fear of abandonment but behave in unpredictable ways eliciting rejection).
MCMI III—Means and SDs of BR Scores of Grossman Facet Scales
Discussion
Conflict Resolution and Violence
CTS 2S scores suggest mutuality of violence in their relationships, and therapeutic interventions may center around working on couple conflict resolution dynamics. However, the men’s self-reports are not consistent with reports of their behavior documented in case files and may represent social desirability, or tendencies toward externalizing responsibility and blame. Therapy can focus on encouraging them, so as to accurately accept responsibility.
Violence in Family of Origin
Just over half of the perpetrators reported experiencing childhood abuse or witnessing domestic violence. Results are consistent with Social Learning Theories8,11,12 and testify to the role modeling provided by fathers for males in the family, that makes IPV seem acceptable as the dominant mode of expressing anger and resolving conflicts. Therapy can focus on processing early trauma and understanding how it affects beliefs, and exposure to healthier role models. However, while Jin et al 8 found this to be the strongest predictor of IPV, about half of the perpetrators in our sample did not report childhood abuse, suggesting that it may not be a necessary precondition.
Attitudes Toward Women
Mean scores for the sample were similar to the normative mean scores of fathers provided by Spence et al. 19 Scores tended slightly more toward liberalism than traditionalism. The findings suggest that gender theories8,13 may not explain violence in entirety and for this cohort-patriarchal beliefs may not be a sufficient condition for IPV in the absence of psychopathology. Although they seemed to consider themselves to be liberal, the violence perpetrated by these men continued to be gendered, suggesting that subtle sexist beliefs may be at work and these may need to be explored further.
MCMI III Profiles
The highest score on the Clinical and Severe Syndrome scales was on anxiety, followed by dysthymia and delusional disorder. However, based on the mental status examination, the latter may represent the rigidity of paranoid beliefs rather than poor ties with reality. Contrary to previous Indian research,8-10 less than 20% of men reported or manifested substance abuse. The need to teach coping styles for anxiety seems to be crucial, as it is possible that IPV may have evolved as a convenient way that men have learnt to deal with their high levels of stress. Pharmacological intervention can thus be considered.
The high percentage of the sample showing traits of personality disorders suggests that personality psychopathology may play a crucial role in the perpetration of interpersonal violence. Less than 20% showed antisocial, borderline, and narcissistic personality traits that have previously been implicated in propensity to IPV. 1 Research suggests that male perpetrators of IPV show a diversity of traits and personality disorders. 20 Most of the men profiled here seem to fall in Hamberger and Hastings’ 6 category of negativistic dependent perpetrators.
The Grossman Facet scale elevations suggest that the strongest tendencies seemed to be a high need for nurture and support and a fear of abandonment, mistrust in relationships (also reported by wives as constant unfounded suspiciousness held by their husbands/partners about their infidelity), manipulative and volatile behaviors, adherence to convention and ideas of propriety (in the Indian context, it may manifest as upholding existing patriarchal family structures), and poorly formed object relations based on problematic childhood experiences.
At a preliminary level based on these specific profiles, suggested therapeutic goals may be working on paranoid patterns, reducing dependence, teaching healthier emotional expression, and exploration of problematic internalized representations of interpersonal relationships.
Limitations of the Study
The study was descriptive and did not seek to draw inferences. Our sample size was small and we used convenience sampling. We may therefore not have been able to capture data representative of all male perpetrators of violence. It remains to be seen whether research with a larger and more representative sample of men may yield typologies of male perpetrators of IPV that are similar to those obtained in research across the world.2-4 We have also not studied specific relevant variables such as religion that may also play a role. Also, interpretations need to be made with caution in the absence on a control group of nonoffending men.
Conclusion
To the best of our knowledge, our study is the first in India to consider in-depth MCMI III profiles and analysis of Grossman Facet scales to understand clinical and personality psychopathology in male perpetrators of IPV. We combined this with an exploration of other clinical and psychosocial factors such as alcohol dependence and clinical disorders, the role of childhood abuse and domestic violence, and patriarchal beliefs. This pilot study offers some suggestions for therapeutic interventions and proposes that any intervention for male perpetrators of violence has to take into account both clinical and psychosocial factors, and can be best facilitated by a team of social workers, clinical psychologists, and psychiatrists.
Footnotes
Acknowledgements
The authors would like to thank the study participants, the team at the Prevention of Violence against Women and Children (PVWC) program,, the funders, and Ethicos Independent Ethics Committee.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Azim Premji Philanthropic Initiatives (APPI).