
Abstract
Abstract
Sexual dysfunction is commonly associated with the use of substances, in both men and women. This area requires prominent attention, particularly as the use of substances is often with the expectancy of improving an underlying sexual dysfunction or with a positive expectancy of enhancing sexual function.
The chronic use of substances has a negative impact on sexual function and causes various kinds of sexual dysfunction in both men and women. In this narrative review, we look at the effect of various substances of abuse on sexual functioning and discuss management strategies in such situations.
Introduction
Sexual dysfunction is described as any disruption of normal sexual activity in an individual or couple. Such dysfunction could occur in any of the phases of the normal sexual cycle (physical pleasure, desire, preference, arousal, or orgasm). In large epidemiological studies in the United States, more than 40% of women and 30% men were reported to have some form of sexual dysfunction. 1 Corresponding figures in European countries are 34% among women and 15% among men. 2 Older studies in developing countries suggest a rather high prevalence of erectile dysfunction among men presenting to primary care (57.4% in Nigeria, 63.6% in Egypt, and 80.8% in Pakistan). A more recent general population study from India reports a 14% prevalence of sexual dysfunction among women and 21.2% among men. 3
Common risk factors associated with sexual dysfunction include the individual’s general health state, the presence of non-communicable diseases such as diabetes mellitus, cardiovascular diseases, genitourinary diseases, psychiatric/psychological disorders, and chronic diseases. 4 The association between substance use and sexual dysfunction has been increasingly recognised. 5
Substance use disorders are a global problem and contribute to preventable mortality and morbidity. The estimated global prevalence of heavy episodic alcohol use among the adult population was 18.4% in 2015. Similarly, the prevalence of tobacco smoking, cannabis use, and opioid use was 15.2%, 3.8%, and 0.37%, respectively. 6 The morbidity measured in terms of disability-adjusted life-years (DALYs) was highest for tobacco smoking followed by alcohol use and illicit drug use.
In India, substance use disorders have a weighted prevalence of 22.4%, with tobacco use disorders (20.89%) and alcohol use disorders (4.64%) leading the numbers, according to the latest National Mental Health Survey of India. 7
A discussion about sexual function and dysfunction is important in the context of substance use as substances such as alcohol, opioids, and cannabis are often used with the expectancy of enhancing sexual functioning. This may be because of the depressant, anti-anxiety, and disinhibitory effects of some of these substances, especially during early use and in lower quantities. However, many studies have shown that chronic use of substances has a negative impact on sexual function and causes some or other form of sexual dysfunction in both men and women.
In this narrative review, we attempt to look at the effect of various substances of abuse on sexual functioning and discuss management strategies in such situations.
The Normal Sexual Cycle and Sexual Dysfunction
The human sexual response cycle can be divided into 4 phases: excitement (desire and arousal), plateau, orgasm, and resolution. 8 There is a transition from one phase to another in the presence of an erotic stimulus. The phases are influenced by the complex interplay of endocrine and nervous (central and autonomic) systems. Sexual dysfunction can occur in any of these phases. Common sexual dysfunctions include hypoactive sexual desire disorder, erectile disorder, premature (early) ejaculation, delayed ejaculation in men, and female sexual interest/arousal disorder, female orgasmic disorder, genito-pelvic pain/penetration disorder in women. Substance/medication-induced sexual dysfunction, other specified sexual dysfunction, and unspecified sexual dysfunction form the remaining categories of sexual dysfunction. 9 Different substances of abuse can affect any of these stages to cause sexual dysfunction.
Use of Specific Substances and Related Sexual Dysfunction
In this section, we discuss the sexual dysfunction associated with the use of specific substances.
Alcohol
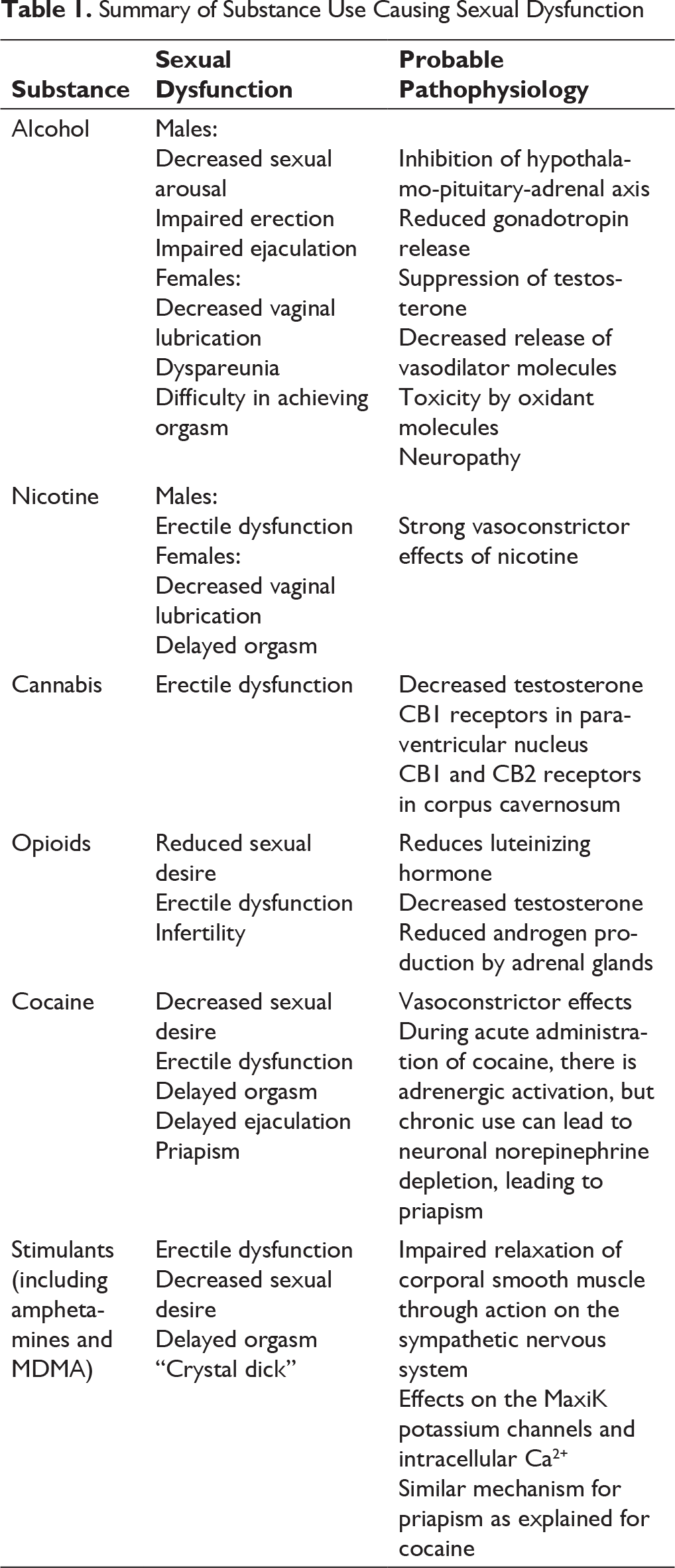
Alcohol causes central nervous system depression and also leads to disinhibition. It has been used as an aphrodisiac over the ages to elevate sexual desire and functioning. However, many studies have indicated the range of deleterious effects of alcohol on sexual functioning. In men, it causes little to a mild increase in sexual arousal. However, when taken in higher doses, it decreases sexual arousal, impairs erection, and decreases the individual’s ability to ejaculate. Long-term use of alcohol, through its effects on various organ systems, causes almost all types of sexual dysfunction in males. 10 Through its inhibitory effect on the hypothalamo-pituitary-adrenal axis, it reduces gonadotropin release leading to hypogonadism. It also causes suppression of testosterone leading to erectile dysfunction. The decreased testosterone may be due to reduced gonadotropins or suppression of testicular secretion of testosterone caused by the direct effect of alcohol. Other mechanisms that may be involved in testosterone suppression include the decreased release of vasodilator molecules like nitric oxide and the toxic effects of the oxidants produced during the metabolism of alcohol. Erectile dysfunction may result from alcohol-induced neuropathy or because of the cardiovascular complications caused by chronic use of alcohol.
In women, alcohol intake in lower quantity may cause increased subjective arousal and pleasure. In higher quantities, however, it decreases sexual arousal. In chronic users of alcohol, there may be decreased vaginal lubrication, dyspareunia, and difficulty in achieving orgasm.
Though many studies have shown that these changes in sexual function are reversible on abstinence, this may not be universally true.
Use of alcohol has also been found to be associated with risky sexual behavior in the studies on disease transmission in the context of human immunodeficiency virus (HIV). 11
Nicotine
The effects of smoking on sexual function are long known, especially in men. Smoking causes erectile dysfunction, with impairment of both initiation and maintenance of erection. This is due to the strong vasoconstrictor effects of nicotine. Nicotine is also believed to reduce other vasoactive substances such as endothelium-derived relaxing factor and nitric oxide. Although the effects of smoking on sexual function in women are not well studied, some studies report of decreased vaginal lubrication and delayed orgasm caused by the vascular effects of nicotine. 12 Such effects of tobacco on sexual function can be seen even in the users of smokeless tobacco as well as in users of isolated nicotine. 13
The sexual dysfunction due to nicotine seems to increase with increased quantity of use. Prolonged abstinence can reverse some of these changes.
Cannabis
Historically considered as an aphrodisiac, present evidence regarding the effects of cannabis on sexual function is conflicting. The use of cannabis may lead to subjective feelings of improved sexual pleasure and satisfaction. Chronic use of cannabis may lead to decreased testosterone. Animal studies involving the endocannabinoid system have shown inhibitory effects of cannabis on erectile function. 14 This may be due to the central effects of cannabinoid 1 receptors in the paraventricular nucleus of the hypothalamus or due to the peripheral effects of cannabinoid 1 and cannabinoid 2 receptors located in the corpus cavernosum.
Opioids
Opioid use in the initial stage causes delayed ejaculation in men and improvement in vaginismus in women, leading to a perception of improved sexual function. However, chronic use of opioids such as morphine and heroin reduces the release of luteinizing hormone further leading to decreased testosterone and estradiol with an increase in free sex hormone binding globulin causing hypogonadism. 15 This is associated with reduced sexual desire, erectile dysfunction, and infertility. Chronic opioid use is also associated with reduced androgen production by the adrenal glands (dehydroepiandrosterone—DHEA, dehydroepiandrosterone sulfate—DHEAS, and androstenedione). Similar effects on sexual function are also seen with long-term opioid substitution therapy, more with the use of methadone than with buprenorphine.
Cocaine
Cocaine is a stimulant of the central and peripheral nervous system which inhibits the uptake of dopamine and norepinephrine. Initial use may induce sexual arousal and improve erectile function. However, prolonged use of cocaine decreases sexual desire and erectile function and causes delayed orgasm/ejaculation. This effect is noted to be worse when cocaine is used along with other psychoactive substances, including alcohol.
Amphetamines
Amphetamines are stimulants that act by blocking the reuptake of dopamine and norepinephrine. They are believed to be potent aphrodisiacs and, in small doses, can increase sexual desire and cause a delay in orgasm. This may be because of decreased inhibition, increased confidence, and a heightened sense of energy. These effects are especially well known with methamphetamine. Prolonged use of methamphetamine, however, may lead to difficulty in achieving a full erection, decreased sexual desire, and anorgasmia. 16 This can lead to a condition referred to as “crystal dick” with a strong sexual drive and inadequate penile erections.
MDMA
Methylenedioxymethamphetamine (MDMA), popularly known as “ecstacy” or “love drug” causes improved sexual experience. However, chronic use leads to impaired erection and delayed orgasm. 17
Nitrite Inhalants
Summary of Substance Use Causing Sexual Dysfunction
Assessment
Sexual dysfunction in the context of substance use is not only caused due to the direct effects of the substances but is also influenced by psychosocial and cultural contexts, comorbid psychiatric and medical illnesses, as well as treatment-emergent side effects. The information regarding sexual problems may not be shared voluntarily and sometimes the patient may be unaware of the same. It takes a careful and detailed sexual history to elicit various aspects of sexual dysfunction. This should be done while making sure that the patient is comfortable and ensuring confidentiality.
The clinician should inquire into various aspects of the patient’s presenting complaints, including the specific symptoms, onset, duration and progression of the symptoms, symptom severity, any related exacerbating or relieving factors. The impact of current symptoms on the patient’s life as well as on the attitude towards treatment, any interpersonal issues with the partner caused by current problems, as well as any treatment sought or self-medication should be explored. Past sexual history including first sexual contact, knowledge about sexual functioning as well as the history of sexual abuse will also add important information to the assessment and management plan. A history of high-risk sexual behavior is an inevitable part of sexual history.
Approach to Management
It is important to have a relationship-centered approach rather than a disease-centered one during the management of sexual dysfunction in the context of substance use disorders. 20 Various interventions for sexual dysfunction are as follows
Feedback About the Relationship Between Substance Use and Sexual Dysfunction
The first step in the management of sexual dysfunction is a personalized explanation of the relationship between the use of substances and consequent sexual dysfunction. Even in the presence of other possible physical or emotional contributory causes for the sexual dysfunction, it is useful to explain to the individual, in a motivational interviewing approach, the benefits of substance use cessation on sexual functioning, the further complications of continuing substance use, and to negotiate a substance-free period in order to make a proper assessment and management plan for the dysfunction.
Assessment of Other Causes for Sexual Dysfunction
It is important to look for any organic causes of sexual dysfunction during assessment. 21 This would include, apart from a detailed history, a thorough general physical and systemic examination. The laboratory investigations including hormonal profile can be considered in addition to the routine investigations (hemogram, blood glucose levels, liver function tests, lipid profile, thyroid function tests). A consultation with a specialist may be warranted in the presence of any positive findings during history, examination, or laboratory tests.
Psychosocial Management
After the assessment, interventions need to be tailored according to the patient’s needs. Educating the patient and partner about the risks of substance use and its effects on sexual function is very important. This includes providing knowledge about the anatomy and physiology of normal sexual function, sexual response cycle, and addressing their doubts and myths about sexual function. Therapy may include improving communication patterns between the couple, improving awareness, and sensate focus therapy.
Various approaches such as Master and Johnson’s approach, PLISSIT model, Kaplan’s approach, and sensitization-desensitization model can be used according to patient’s individual presentation and requirements.
Sexual dysfunction can be an important factor towards changing motivation and emphasizing abstinence from substance use. It should be integrated into motivational enhancement therapy whenever possible. It is also important to look at sexual dysfunction as a maintaining factor for relapse and address the same.
Pharmacological Management
In men, phosphodiesterase 5 inhibitors are found to be beneficial for the erectile dysfunction and can be used on an as-needed basis without serious long-term side effects. Alternatively, intracavernosal injections and non-pharmacological modalities like vacuum devices are also available. The utility of testosterone replacement for erectile dysfunction or sexual desire is limited. Whenever prescribed, it can be given under supervision or as transdermal preparations to avoid inappropriate use.
Selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine and paroxetine are beneficial for premature ejaculation. Other preparations include the use of local anesthetic like lignocaine and techniques like Master and Johnson squeeze technique.
In women, systemic testosterone can be considered for hypoactive sexual desire. However, it is associated with side effects such as hirsutism, hoarseness of voice, alopecia, and a potential increase in cardiovascular diseases which limits the utility of testosterone treatment. Topical estrogens can improve the vaginal lubrication and genital arousal.
Conclusions
The use of certain substances may be related to the user’s positive sexual expectancies from such use. However, it is evident that all substances used for their mind-altering properties have a variety of adverse consequences on different phases of the sexual cycle. Awareness of sexual dysfunction is an important preventive approach to discourage substance misuse. Any detailed assessment of a person with substance use needs to include an assessment of sexual dysfunction. Educating and negotiating a substance-free state to allow a proper assessment of sexual dysfunction as well as potential reversibility, a thorough assessment of other possible underlying causes, and combined psychosocial and pharmacological interventions are suggested for persons with substance use disorders and sexual dysfunction. Addressing sexual dysfunction needs to be an integral component of relapse prevention.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors for this article.