
Abstract
Abstract
Keywords
Introduction
Adolescence is a precarious period in youths’ sexual development because of the interrelationship between sexual experimentation, cognitive development, and emotional development. Risky sexual practices among youth, which encompass early sexual debut, multiple sexual partners, engaging in unprotected sexual intercourse, and engaging in sex with older partners, are associated with an increased risk of a negative outcome.1- 3 Previous reports have shown that youths’ risky sexual behaviors (RSBs) are significantly related to their vulnerability to develop human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs).4, 5 Such behaviors developed during youth may also influence sexual behavior in adult life, thus increasing the cumulative risk of acquiring and transmitting STIs.6- 8
Attention-deficit/hyperactivity disorder (ADHD), one of the most common psychiatric disorders among children and adolescents, 9 can be a developmental precursor of early onset of risky behaviors which can persist into adulthood (Utah criteria for adult ADHD) 10 as a full clinical picture or as a partial syndrome in 60% of cases. 11
Studies have indicated that ADHD is linked with early sexual debut or failure to use condoms. 12 Also those with childhood ADHD were more likely than those without ADHD to report casual sex and sex with multiple sex partners. 13 This can be attributed to multiple factors such as impulsivity, associated conduct symptoms, and comorbid substance use. 14
Alcohol use is one of the other factors, frequently cited by several studies, that increases the likelihood of RSBs and HIV acquisition. 15 Adults with ADHD are known to be associated with early onset of alcohol dependence, including its severity of use. 16 Comorbid substance use in these adults may propel them to engage in RSBs. 17
High levels of perceived stress have been associated with both alcohol use and risky sexual behaviours.18- 20 Eighteen to twenty adults with ADHD, possibly due to their inherent executive dysfunction, exhibit maladaptive coping styles, hence making them more vulnerable to having high levels of perceived stress, which in turn has been theorized to increase the chances of indulgence in RSBs. 18
Steps Involved in Methodology
Thus, there exists a close link between RSB, ADHD, comorbid substance use and perceived stress. However, there is a significant paucity of data regarding prevalence and correlates of RSB in those with ADHD who have comorbid alcohol use disorder (AUD).
So far, methylphenidate has not been found to be effective in reducing RSB in ADHD. 21 This may be because the existing studies have included a heterogeneous sample of those with ADHD who also had comorbidities such as conduct disorder, antisocial personality disorder and other axis 1 psychiatric comorbidities which may have independently influenced the occurrence of the mentioned variables. Our effort here has been to study the effect of methylphenidate on RSB in a homogeneous population.
Aims and Objectives
The aims and objectives of the study are as follows: To study the association of RSB with severity of ADHD and
alcohol use among adolescents and young adult males with ADHD who
had comorbid AUD. To study the effect of treatment of ADHD using methylphenidate
on RSB among adolescents and young adult males with ADHD who had
comorbid AUD at 3- and 6-months follow-up.
Methodology
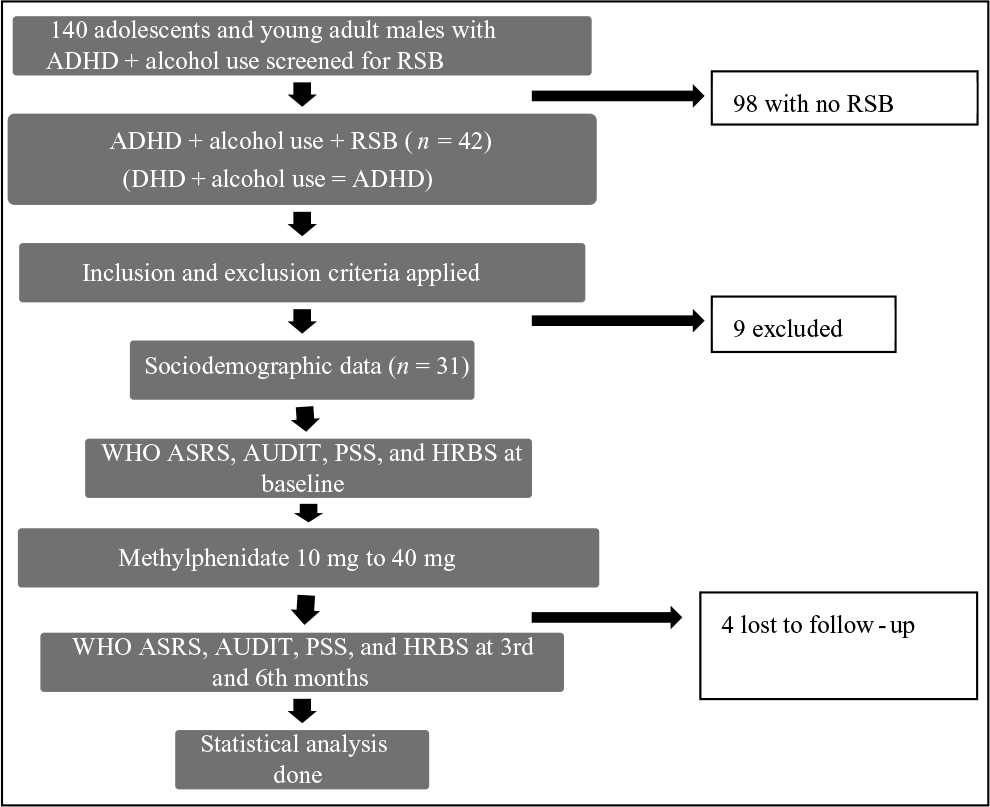
This study is an open label study conducted at the outpatient and inpatient de-addiction unit of a tertiary care hospital from July 2014 to December 2015 after approval from the institutional review board. Written and signed informed consent was obtained from every patient who was enrolled in the study. Adults with ADHD with comorbid AUD were identified based on clinical diagnosis. The present sample of 31 adolescents and young adult males (Figure 1) with ADHD was then screened for RSBs using the sexual behavior section of the HIV risk-taking behavior scale (HRBS) manual.
Males diagnosed with ADHD and who had comorbid AUD and RSB at baseline (indicated by any score greater than 1 on HRBS sexual behavior section), aged between 15 and 25 years, consenting for treatment were included (N = 31) in the study. Those who had substance use (except nicotine) (n = 3), comorbid mood disorder (n = 6), psychosis (n = 0), anxiety disorder (n = 3), and antisocial personality disorder (n = 6) were excluded from the study by using MINI Plus. Patients who were already diagnosed with seizure disorder (n = 1) and congenital heart disease (n = 0) were excluded from the study. Those already on methylphenidate (n = 0) or other psychotropics (except benzodiazepines, naltrexone [n = 4] or acamprosate [n = 6]) which could be used for treating comorbid alcohol dependence syndrome) were excluded from the study in order to get a sample that is treatment naive for ADHD.
The following scales were then administered to them:
All individuals were briefed about ADHD, risky behaviors, alcohol use and the relationship of each of these factors with each other. A clinical psychologist also educated them about the benefits of treating ADHD which included possible reduction in alcohol-use severity and stress. Need for compliance was also stressed upon and supervision by caregiver was advised. All individuals received methylphenidate, starting from a dose of 10 mg (sustained release, once a day) which was titrated based on response and body weight up to a maximum of 40 mg, in increments of 10 mg every week.
WHO ASRS, AUDIT, PSS and HRBS were also measured at the end of 3rd- and 6th-month follow-ups. A total of 4 patients were lost to follow-up (13%) at the end of the 6th month and could not be contacted. Reminders were sent over short messaging service to patients and one caregiver (who was identified initially) weekly regarding medication compliance, which was enquired during follow-up through regular interviews by the clinician.
Statistical analysis: The association of different variables at baseline was performed using correlation analysis. Wilcoxon signed rank test was used to measure differences in variables between baseline and at 3rd- and 6th-month follow-up. Logistic regression was used to measure odds of predicting the decrease in RSB using ADHD, alcohol-use severity and perceived stress.
Results
A total of 140 adolescents and young adult males were screened, among which 31 individuals qualified for the study as they had ADHD with comorbid AUD and RSB. The prevalence of patients with ADHD, comorbid AUD and RSB in this study was 22.14% (n = 31).
Sociodemographic Data (Continuous Variables)
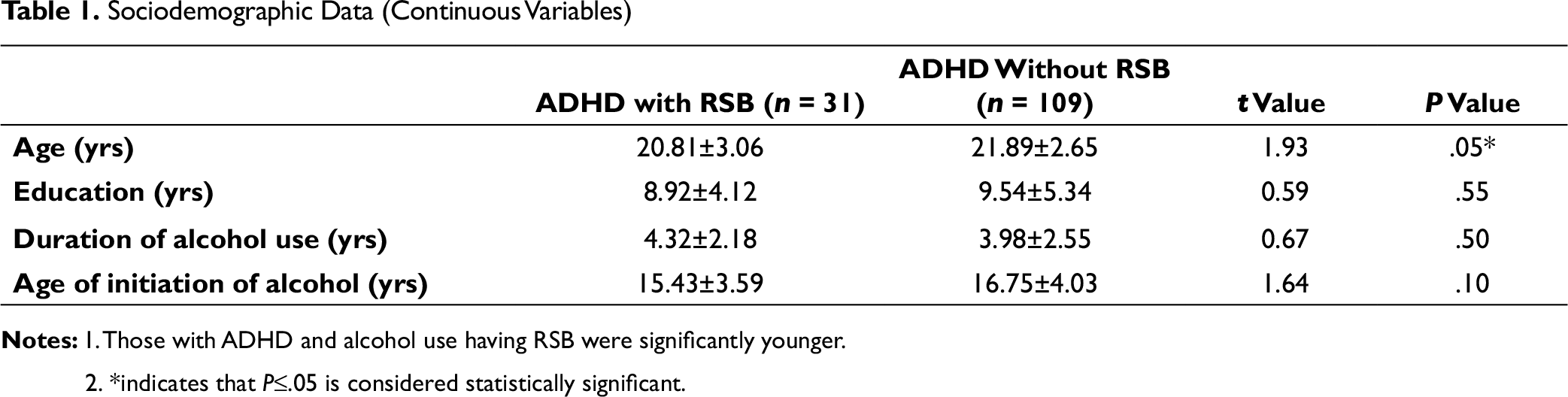
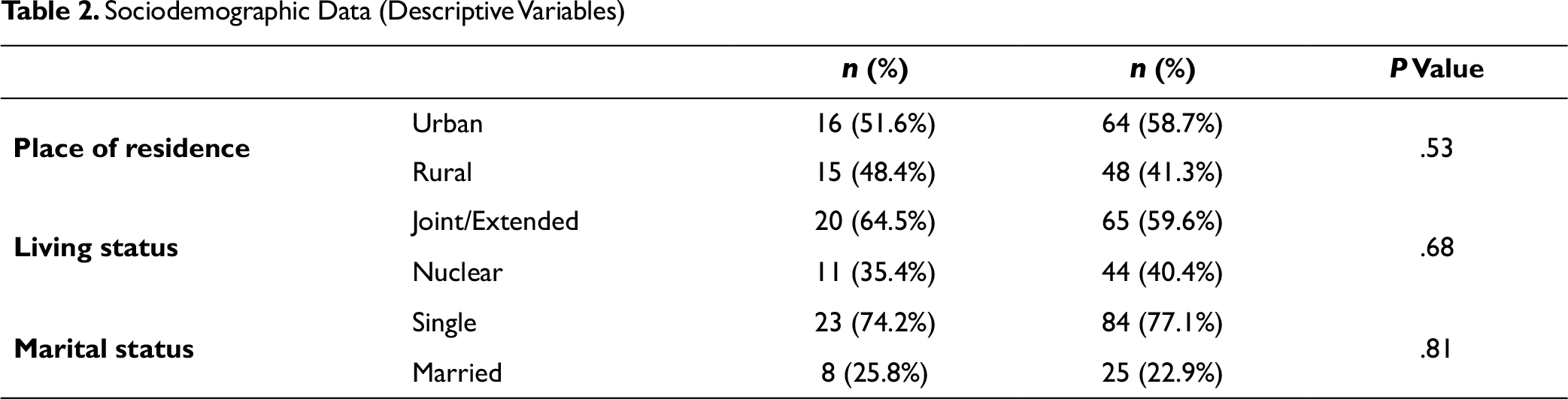
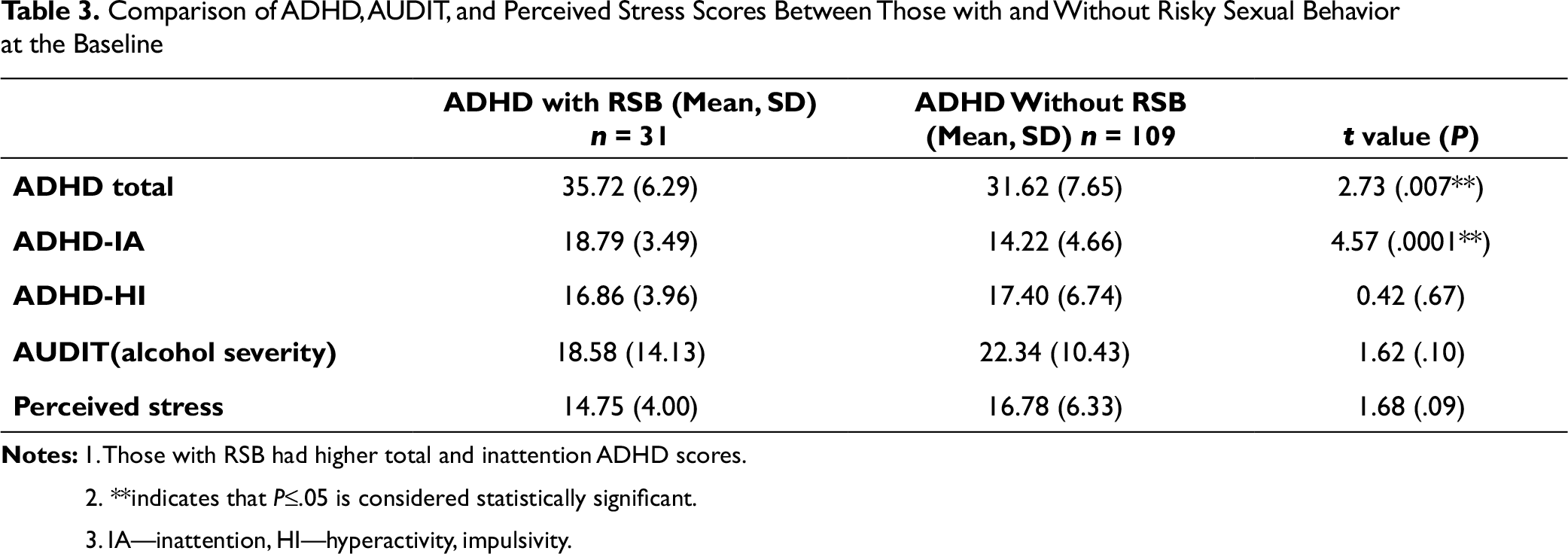
It was observed that study individuals with ADHD and RSB had an earlier age of presentation than those without (refer to Table 1). There were no differences in distribution of the place of residence, living status and marital status among two groups (Table 2). Higher total and inattention ADHD scores were observed among study subjects with RSB (t = 2.73 and 4.57 and with p value = 0.007 and 0.0001). However, the two groups did not differ in ADHD-HI, AUDIT and perceived stress scores (Table 3).
Sociodemographic Data (Descriptive Variables)
Comparison of ADHD, AUDIT, and Perceived Stress Scores Between Those with and Without Risky Sexual Behavior at the Baseline
Correlation Between Variables at the Baseline Using the Spearman Correlation Coefficient in ADHD with RSB Population
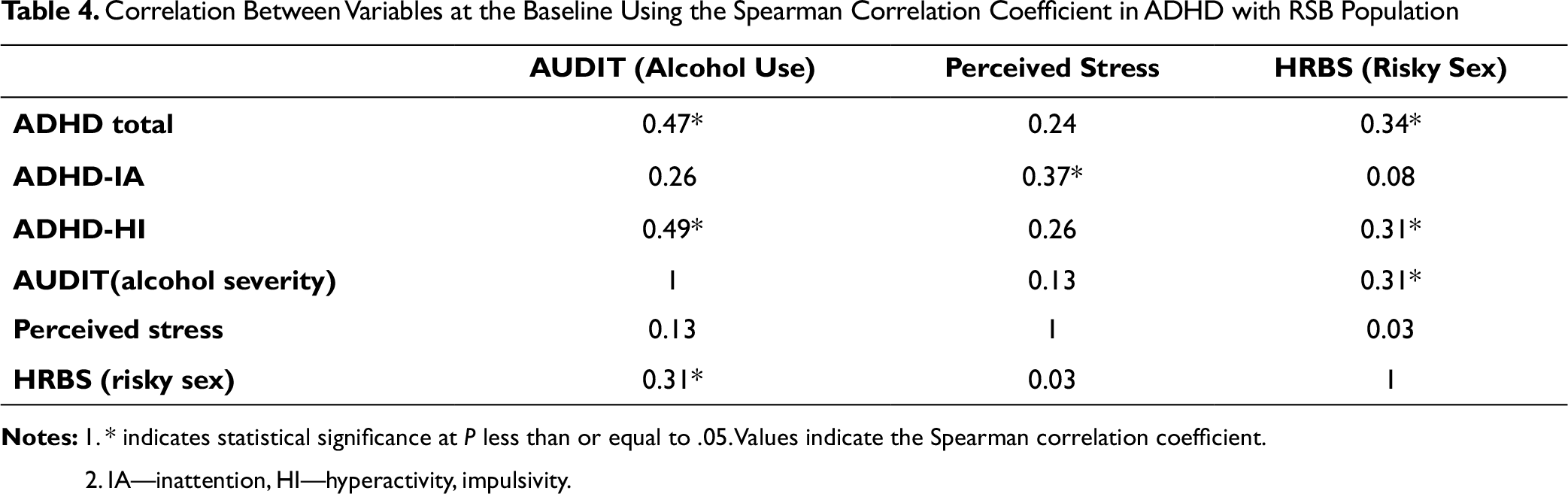
There was a high correlation between ADHD total and AUDIT (r = 0.47), as well as ADHD-HI and AUDIT (r = 0.49). There was moderate correlation between RSB and AUDIT (r = 0.31), ADHD-IA and perceived stress (r = 0.37), ADHD total and HRBS (r = 0.34), ADHD-HI and RSB (r = 0.31), AUDIT and RSB (r = 0.31) (refer to Table 4).
Comparison Analysis at Baseline, 3 Months and 6 Months
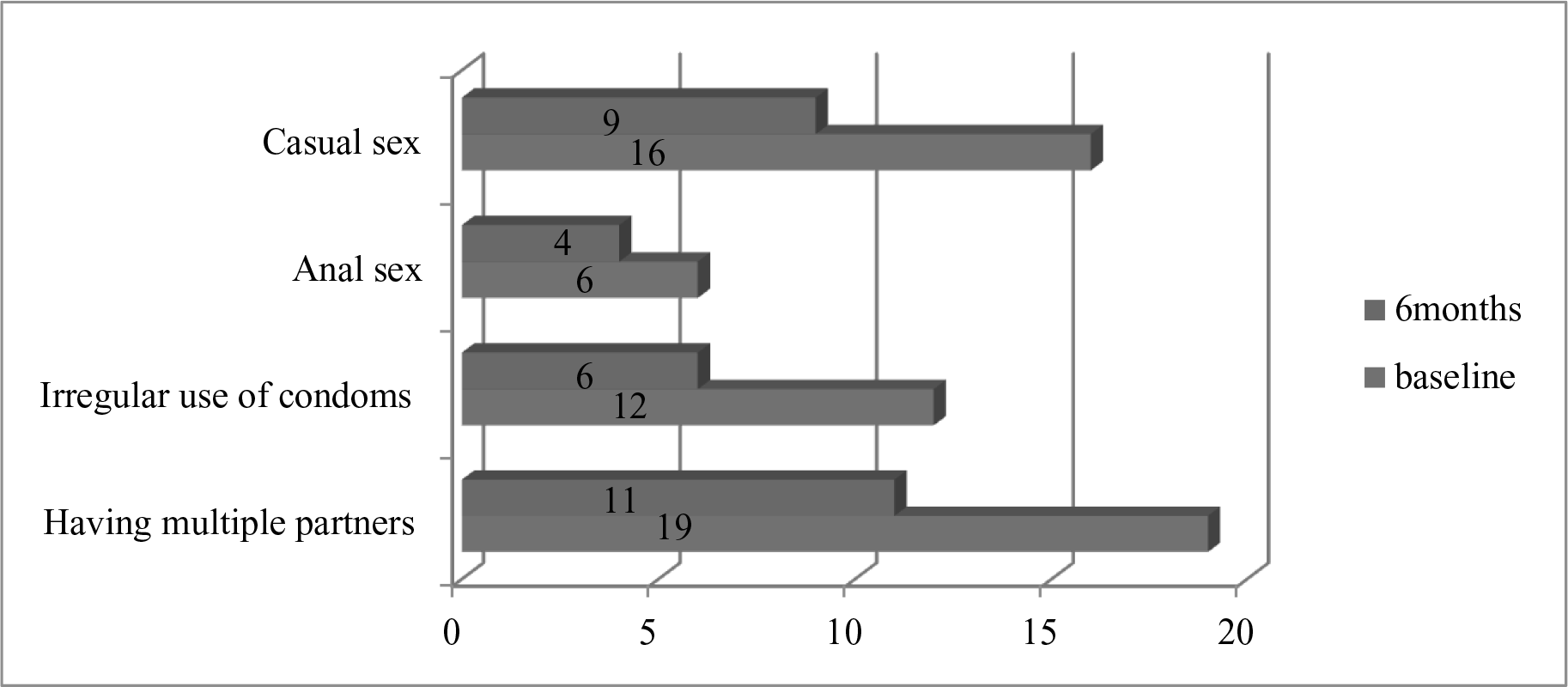
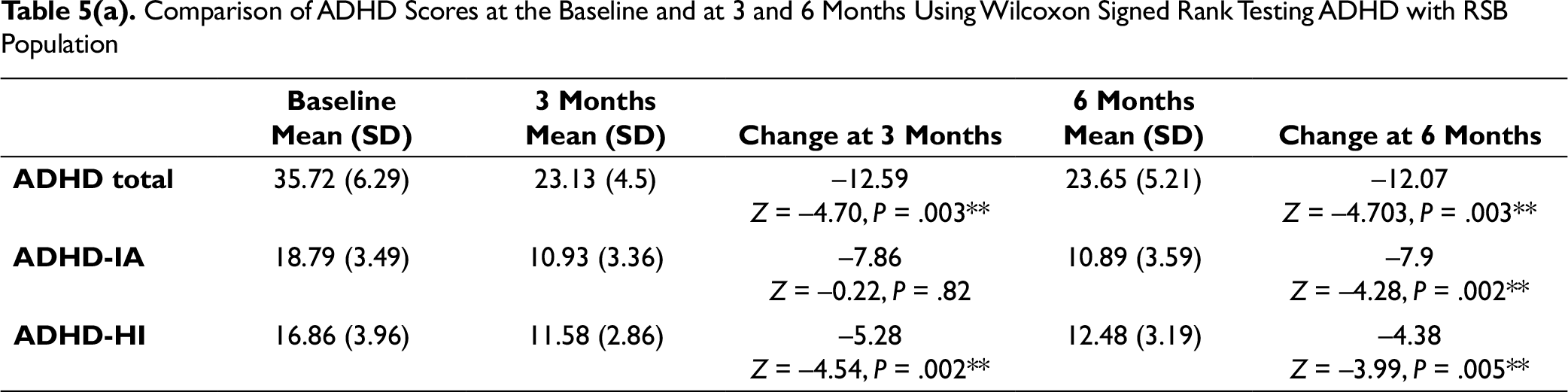
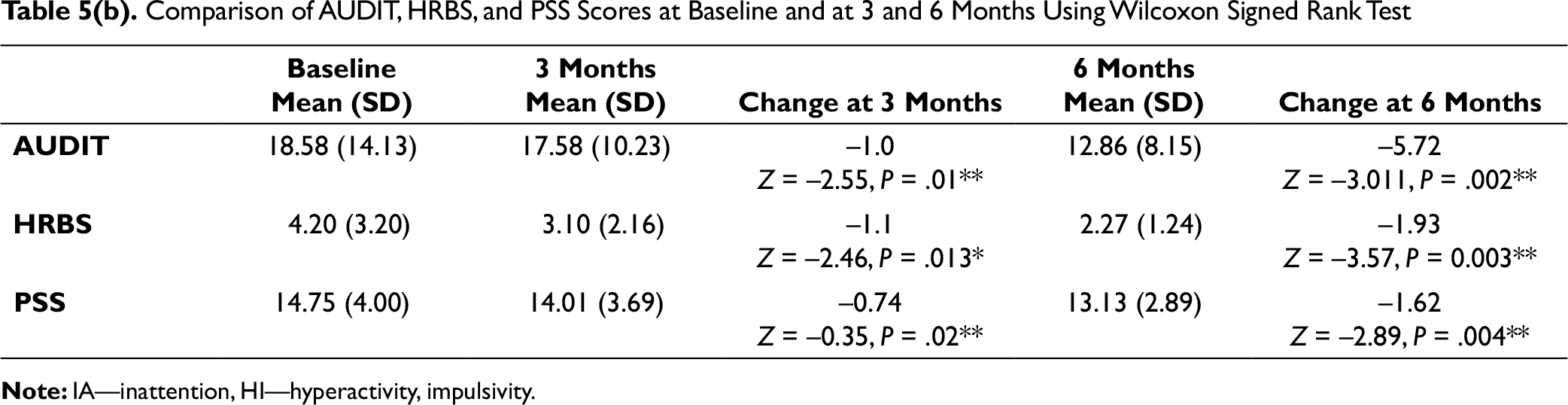
There was a significant improvement in ADHD total and ADHD-HI scores at the end of 3 months and 6 months, with the use of methylphenidate. Also, a similar such improvement was noted in AUDIT, HRBS, and perceived stress scores. ADHD-IA scores saw an improvement at the end of 6 months (refer to Table 5). Most of the risky sexual practices saw a decline at 6 months when compared to baseline (Figure 2).
When logistic regression was done to predict odds of reduction in RSB, it was seen that only ADHD total scores predicted significant reduction [OR =1.26, 95% CI(1.04-1.53) p = 0.01] (refer to Table 6).
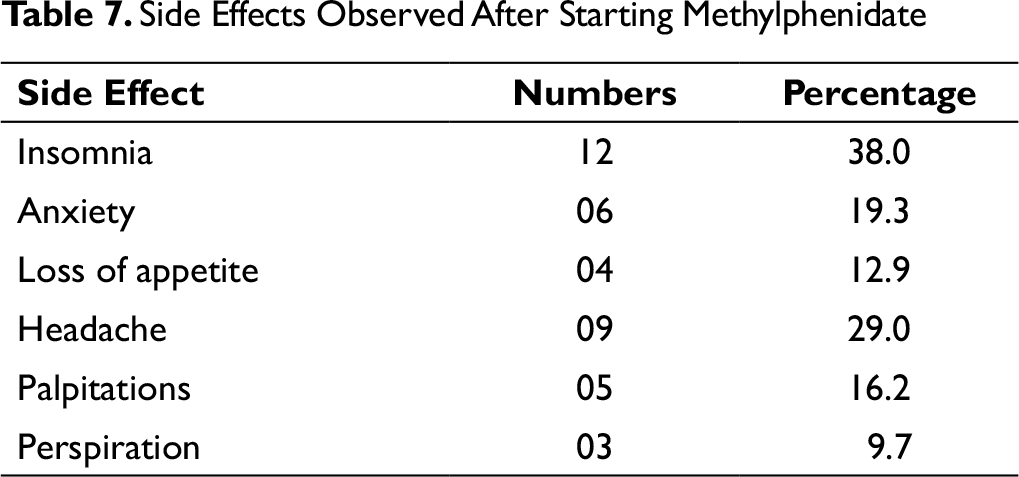
The most common side effect with use of methylphenidate was insomnia (n = 12, 38%) and headache (n = 9, 29%) (see Table 7).
Discussion
Sociodemographic data (refer to Tables 1 and 2): Those with ADHD(+) (ADHD with RSB) were younger than those with ADHD(–) (ADHD without RSB). This difference can be attributed to the higher ADHD scores among those with RSB in this study. The ADHD(+) group had lesser years of education, and earlier initiation of and greater duration of alcohol use which did not reach statistical significance probably due to the low power of the study. Prevalence of patients with ADHD, RSB and comorbid AUD in the study was 22.14% (n = 31). ADHD is known to be associated with early sexual activity, more casual sex, and more sexual partners. 26 Figure 2 depicts the pattern of risky sexual behaviors at baseline and at 6 months. However, there is significant paucity of studies which have determined prevalence of RSB in a cohort of alcohol-use patients with comorbid ADHD.
Baseline Variables and correlations (refer to Tables 3 and 4): The ADHD(+) group had higher ADHD total and inattention scores but not hyperactivity scores. ADHD inattention (ADHD-IA) symptomatology is more strongly related to RSB than ADHD hyperactivity (ADHD-HI) symptoms. Two potential explanations can be offered. First, individuals with ADHD-IA tend to have deficits in executive functioning including planning, cognitive flexibility, self-regulation, and goal-directed behavior 27 which have been associated with greater RSB. 28 Second, it is possible that due to significant overlap between ADHD-HI and ADHD-IA each of these constructs partials out the effects of the other resulting in non-significant effects of one or both constructs.
Alcohol-use severity did not differ between ADHD(+) and ADHD(–). This could possibly be explained by absence of significant difference in ADHD-HI scores between the 2 groups. It is known that ADHD with higher impulsivity scores is a risk factor for alcohol use. 29
Comparison of ADHD Scores at the Baseline and at 3 and 6 Months Using Wilcoxon Signed Rank Testing ADHD with RSB Population
Comparison of AUDIT, HRBS, and PSS Scores at Baseline and at 3 and 6 Months Using Wilcoxon Signed Rank Test
Predicting Odds of Reduction in Risky Sexual Behavior (HRBS Score) with Change in Other Variables Using Logistic Regression
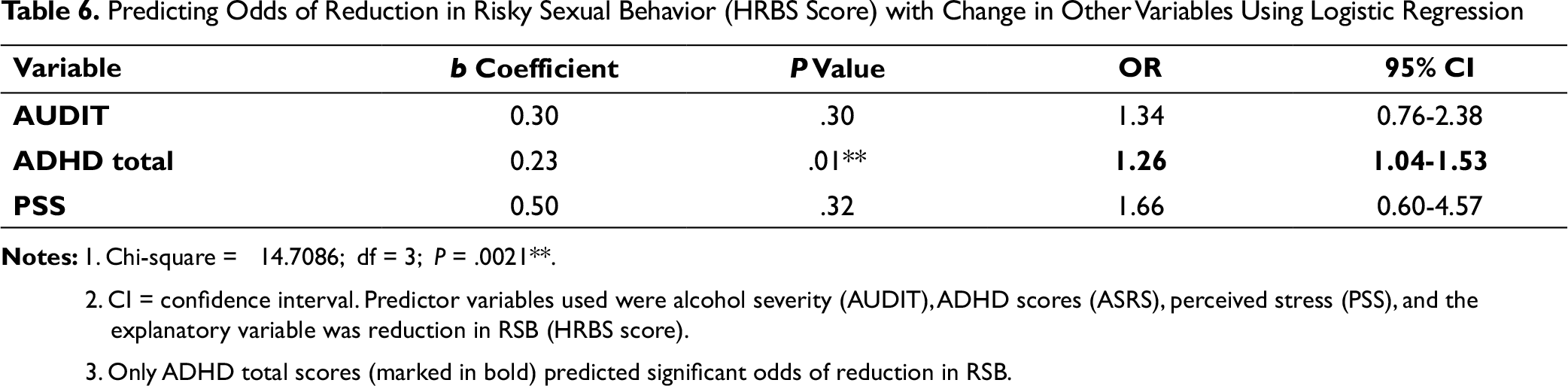
2. CI = confidence interval. Predictor variables used were alcohol severity (AUDIT), ADHD scores (ASRS), perceived stress (PSS), and the explanatory variable was reduction in RSB (HRBS score).
3. Only ADHD total scores (marked in bold) predicted significant odds of reduction in RSB.
Side Effects Observed After Starting Methylphenidate
There is a significant correlation between ADHD total score with severity of alcohol dependence and RSB at baseline. It is well known that ADHD is linked to early sexual debut and RSB.10 ADHD in adults is also known to be associated with early onset of alcohol dependence including its severity.17
Changes in the ADHD scores at 3 months and 6 months (refer to Tables 5(a) and (b)): Except for ADHD total score, ADHD-IA and ADHD-HI showed significant changes at 3 months and 6 months when compared to the baseline.
Changes in other parameters at 3 months and 6 months (refer to Tables 5(a) and (b)): There was significant reduction in alcohol-use severity, RSB, and perceived stress at 3 months and 6 months when compared to the baseline.
When a logistic regression was done to predict odds of reduction in RSB, it was seen that ADHD total scores predicted the reduction but not alcohol-use severity or perceived stress (refer to Table 6).
Stimulant medications like methylphenidate are the most effective medications for treatment of ADHD which alleviate symptoms such as poor attention span, distractibility, hyperactivity, impulsive behavior, and restlessness. 30 They also improve cognitive functions such as spatial working memory, set-shifting, and other precognitive functions. 31 The response rate quoted by studies is 70% to 80%. 32 In the present study, we have also demonstrated a similar benefit of reduction of ADHD symptoms with methylphenidate. The reduction in RSB which is predicted by reduction in ADHD total scores can be explained by improvement of cognitive functioning over time.
Previous studies have failed to show a benefit with methylphenidate on RSB in ADHD. This could be because of a heterogeneous study population which consisted of comorbid conduct disorder, mood disorder, and substance use which may have independently influenced the occurrence of RSB.
Methylphenidate has largely seen to be a safe choice of medication for ADHD. 33 It was well tolerated in our study subjects too. No patient had intolerable side effects. A total of 4 patients (12.9%) dropped out at the end of 6 months of which 2 could not be contacted. The other 2 dropped out mainly due to difficulty in commuting to the hospital.
Merits of the study: The study population consisted of a relatively homogeneous sample of those with ADHD and alcohol use without comorbidities such as mood disorders, psychosis, antisocial personality disorder on which effect of treatment with methylphenidate was studied. The study also used psycho-education so that compliance could be enhanced to ensure low dropout rates.
Pitfalls: The study was statistically underpowered to detect significance. It was an open label study with no blinding and a control group. The effects of drugs and other treatments used for de-addiction among the study sample were not studied. A composite score for quantitatively measuring RSB could have been used for better assessment.
Conclusion and Future Directions
RSB was associated with severity of ADHD and alcohol use. Methylphenidate was not only effective in reducing severity of ADHD but also the severity of comorbid AUD and RSB. Reduction in RSB was predicted by reduction in total ADHD scores.
There is a need for long-term follow-up studies in evaluating comprehensive treatments for ADHD and their effects on reducing commonly occurring comorbidities and psychological issues in ADHD such as RSB, substance use, and risky driving.
Author Contributions
Author 1—conceptualization of study, data analysis. Author 2—coordination of data collection and writing the manuscript. Authors 3 and 4—data collection and proof writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.