
Abstract
Abstract
Introduction
Sexual behavior encompasses all activities which gratify an individual’s sexual needs. Sexual behaviors have been studied in the context of sexual practices, sexual relationships, reproductive health, sexually transmitted infections (STIs), and contraception. While sexual behavior and expression of sexuality are normal phenomena, the context in which sexual behavior is expressed may make the behavior abnormal or risky. While literature has studied variety of risky behaviors, there is speculation about the definition of “high-risk sexual behavior (HRSB).” Risky sexual behavior (which may be equated with the term “high risk sexual behavior”) has been defined by researchers as sexual activities which expose the person to risk of contracting STIs including human immunodeficiency virus (HIV), thus affecting their health. The focus of researchers in this context has mainly been on unprotected sexual intercourse and involvement in sexual activities with multiple sexual partners.1, 2
Substance-use disorders have often been associated with HRSB. For example, certain authors have pointed out that after consumption of alcohol, an individual may indulge into various kinds of risky behaviors, such as involvement with multiple sexual partners and forgetting to use a condom while having sexual intercourse or simply using it in an incorrect manner. Alcohol may itself promote a social environment where one is more likely to indulge in unprotected sexual intercourse. 3 It has also been seen that such behaviors often co-occur with various other deviant behaviors.4, 5
Various theoretical models have been employed to explain the association between alcohol use and HRSB, namely, alcohol myopia theory (AMT), expectancy theory, and cognitive escape theory (CET). Given by Steele and Joseph, 6 AMT states that after consuming alcohol, an individual focuses on cues which are more rewarding than those which seem distal. So the instigating thoughts for having sex are given precedence over inhibiting thoughts of adverse consequences of risky sex. So individuals who fear having sexual intercourse may get instigated to be involved in risky sex. 7 Given by McKirnan and colleagues, 8 CET states the there is an escape between the desire to have sexual intercourse and the desire to avoid contracting HIV. It has been argued that avoidance of risk poses cognitive restraint on the individual and alcohol or substance helps one escape from that restraint. It has been highlighted by various authors that those individuals who are high on effortful restraint and anxious about contracting HIV are at higher risk of practicing unprotected or anal intercourse. 9 Expectancy theory, proposed by Dermen and Cooper, 10 posits that an individual expects the experience of sexual intercourse to be enhanced and sexual inhibitions to be lowered. This makes the sexual intercourse under the influence of substance to be more likely to happen and be riskier. In research, it has been seen that men engaging in risky sexual behavior more commonly expected enhancement of sexual pleasure under influence of substance than those who did not engage in risky sexual behavior.11, 12
Various hypotheses have also been formulated discussing the association between substance-use disorders in general and risky sexual behavior. The relation between risky sexual behavior and substance use has been hypothesized in either direction. So substance use may either precede risky sexual behavior or occur subsequent to it. The former is exemplified by alcohol intake causing disinhibition and leading to HRSB like unsafe sexual intercourse. 13 The latter, on the other hand, is explained by the act of using substances as a means to enhance the pleasure associated with sex. 14 Certain authors have found early sexual intercourse as predictors of experimenting with cocaine. 15 Another alternative hypothesis laid down by some authors is regarding common factor determining both substance use and HRSB, for example, common personality factors (impulsivity and sensation-seeking) or familial factors (family discords, abuse, neglect).14, 16
The term “high-risk sexual behavior” finds a place in a number of articles in literature. Authors have discussed about the percentage of substance users practicing risky sexual behavior and their knowledge about risky sex. However, much of the literature does not give a basis on how HRSB be defined. High-risk behaviors vary in the context of culture, age, sex, and various other factors, and hence it becomes difficult to define them.17, 18 Another challenge faced in defining and measuring HRSB is the silence of this behavior. Individuals are not forthcoming with this information and clinicians are many times hesitant in asking about it. During research, people may give socially appropriate responses thus giving spurious data. With understanding the discussed theories, it is clear that substance-use behavior and risky sexual behavior are strongly interlinked. As defined in various theories, it seems apparent that the risks associated with HRSB would be contraction of STIs (including HIV), unintended pregnancies, or abortion. Some studies consider early initiation of sex/sexual promiscuity as a form of HRSB, while some include having sexual intercourse with an individual who injects drugs under the domain of HRSB. 19 There is need to operationalize and define discretely different behaviors which may be counted as HRSBs, which will help the clinicians to focus on the high-risk groups for various interventions and researchers to “measure” HRSB. This paper aims to look at the evidence of association between HRSB and substance use, the issues in defining HRSB in the context of substance use, and providing a tentative definition of HRSB.
What Does the Literature Tell Us?
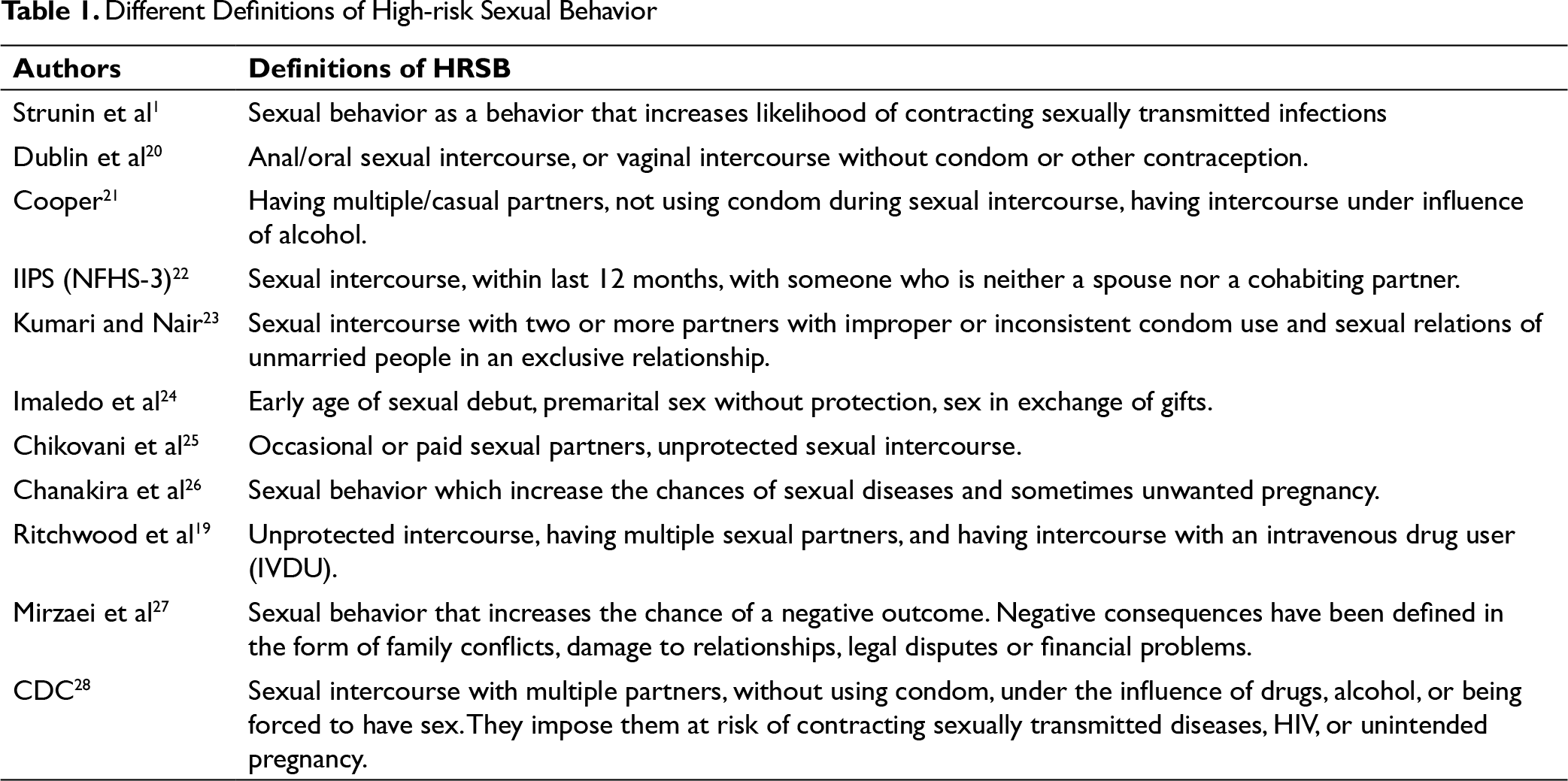
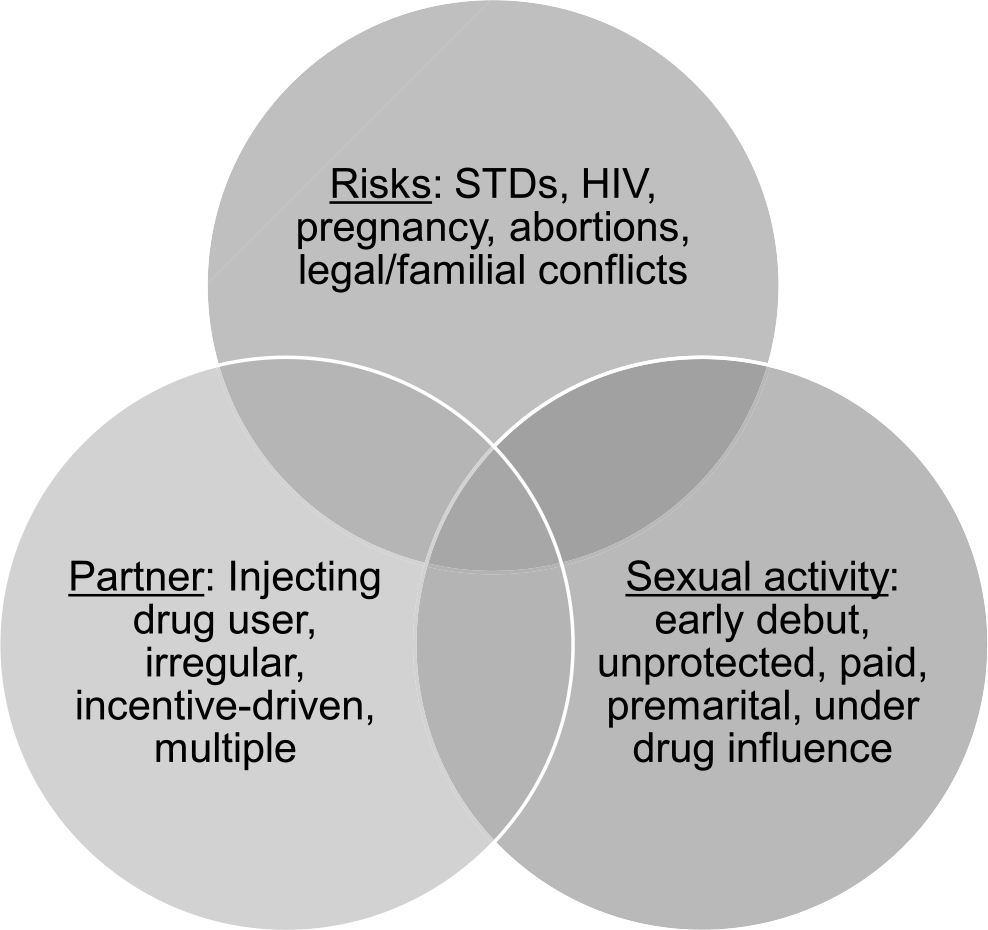
A meta-analysis of 87 studies done to measure the association between substance use and risky sexual behavior defined the latter (or HRSB) as “any behavior that increases one’s likelihood of Sexually Transmitted Infection (STI), including having unprotected intercourse, having multiple sexual partners, and having intercourse with an intravenous drug user (IVDU).”19 This definition is an expansion of the earlier definition which defined risky sexual behavior as a behavior that only increases the likelihood of contracting STIs. 1 However, it is still incomplete as it does not mention the early age of initiation of sexual activity or having sexual intercourse under the effect of substances, which have often been considered as HRSBs in a number of studies. The definition of HRSB has varied according to the variables of interest in the study; for example, Dublin and colleagues 20 defined HRSB in the context of HIV-discordant couples. They, hence, defined the behavior as anal/oral intercourse, or vaginal intercourse without condom or other contraception. It appears that the risk was quantified with respect to the probability of transmitting HIV. Various factors which have been considered by different authors to define HRSB include early age of debut, unprotected intercourse, irregular/multiple/paid sexual partners, concomitant substance use, and associated risks of infection, pregnancies, or even risks of familial conflicts, or conflicts with the law (Figure 1). Table 1 depicts different definitions of HRSB (or risky sexual behavior) in various studies or articles.
Different Definitions of High-risk Sexual Behavior
Factors that Have Defined High-risk Sexual Behavior
According to the WHO data, 29 globally more than one million people worldwide are suffering from STIs, and around 60% of those affected are young individuals. One of the important risk factors as highlighted in the report is injecting drug use. WHO recommends targeting the high-risk population, which includes injecting drug users among others, for preventive measures.
According to the National Family Health Survey (NFHS) 4 in India, the prevalence of HIV in women (aged 15-49 years) with one–lifetime sexual partner was 0.27%, and in those with 5-9–lifetime sexual partners, it was 2.85%. 30 Similarly, in men (aged 15-49 years) with one–lifetime sexual partner, it was 0.5% and increased to 1.6% in those with 5-9–lifetime sexual partners. This suggests that having multiple sexual partners increased chances of having HIV. The prevalence of HIV in males who had paid sex was found to be 0.55%, and in those who did not have paid sex, it was 0.30%. In those who used condoms, it was 0.34%, and in those who did not, it was 0.73%. These figures show us the significant increase in the prevalence of HIV based on one’s sexual practices. Such practices are known to be influenced under intoxicating effects of various psychoactive substances. 3
A study was done by Cook and colleagues 31 on 240 sexually active adolescents, recruited from clinics as well as community. They showed that herpes simplex virus-2 infections were more prevalent in females with an alcohol-use disorder (19%) as compared to females not diagnosed with alcohol-use disorder (10%; adjusted odds ratio = 8.1). A systematic review of published studies to find association between problematic alcohol use and STIs reported positive evidence in 8 out of 11 studies. 32 There is also evidence in literature regarding the association between drug use and HIV. 33 Majority of the evidence comes from studies done on people who inject drugs (PWID) and share their needles/paraphernalia. Literature on finding association between non-injecting drug use and sexually transmitted diseases is sparse, but not absent.34, 35
Another study was conducted by the National Institute of Mental Health and Neurosciences, Bangalore, to screen sexually transmitted diseases in patients admitted in their de-addiction services. They screened 361 patients. Majority patients were diagnosed with alcohol-use disorder (n = 319; 88%). Around 22 (6%) were diagnosed with opioid-use disorder. The rest of them were diagnosed with cannabinoid/sedative/multiple substance-use disorder. Only 11 patients had ever used substance via injecting route, of which 7 were current injectors. At least one STI was diagnosed in 25% and 15.4% of alcohol- and opioid-use disorder patients, respectively. The authors explained reasons for higher STIs in substance-using populations, one of the reasons being poor judgment under the effect of substance. Another explanation is the need to sell sex or exchange sex for food, shelter or safety, as one might be living in an environment which is risky or because one might be out of work. Authors have also proposed that substance use may hamper an individual’s skills to negotiate with their partners for safer sexual practices and may also lead to unstable sexual partners, and eventually risky sexual behavior, thus increasing the risk of contracting STIs. 36
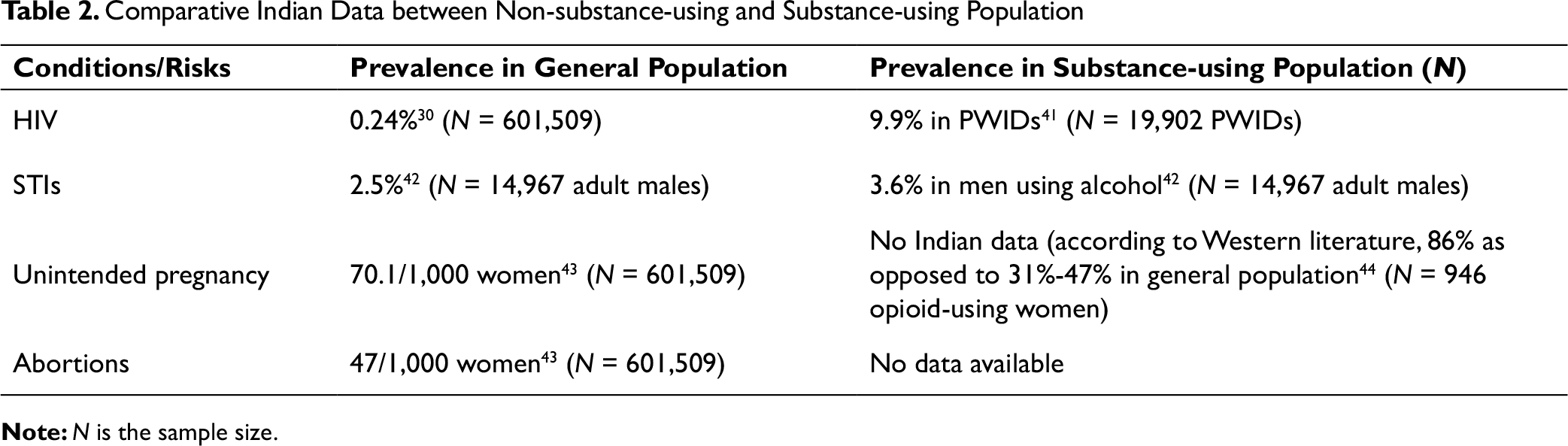
The risk of contracting STIs, including HIV/AIDS, has been highlighted as a risk associated with HRSB. It is important to focus on HIV in India as India has one of the largest number of HIV-infected population worldwide and the second largest population in the world. It has been projected that with growing population, India might become the epicenter of HIV/AIDS. Every factor contributing to its spread should be studied, quantified, and managed.37- 39 However, the weightage given to various other risks associated with HRSB gets limited attention in literature, for example, adolescent pregnancies, unwanted pregnancies, and repeated abortions (as can be seen in comparative Indian data provided in Table 2). There is a need to address these too.
Comparative Indian Data between Non-substance-using and Substance-using Population
A study was done in the West, taking 77 females using substances (excluding problematic alcohol use). Of these women, 41 were sexually active, out of which around 66% (37.5% of the total sample) reported having been indulged in sexual activity in the last 4 weeks where they perceived risk of becoming pregnant unintentionally. Approximately, one-third of the total females got themselves tested or treated for chlamydia or gonorrhea or genital herpes or genital warts, in the previous one year. Lifetime percentage for the same was 87% (N = 67). 40
Table 2 shows comparative data of some of the large surveys conducted in India, of various consequences of high-risk behaviors in general population and substance-using population. It is evident from comparing the data that the rates of sexually transmitted diseases, HIV, unintended pregnancies are significantly higher in substance-using population as compared to general population. This is indicative of the fact that high-risk behavior is much more strongly associated with substance-using population than general population.
Discussion
It is evident from the literature that a concrete and uniform definition of HRSB is yet to be settled upon, especially in context of substance use. While it has been highlighted that HRSB is more strongly associated with substance-use disorder, there is lack of data, especially from India, about the prevalence of HRSB (and its consequences) amongst this group. There are a number of issues in defining HRSB in the context of substance use, namely, variations across culture, ages, and even gender. A behavior may be counted as normative for an adolescent but is considered abnormal and risky if exhibited by an adult. Secondly, there is “hesitation” on the part of “patients” in reporting about such behaviors in clinics, and “social appropriateness” on the part of “study subjects” while it is assessed as a part of a research. Till date, the surveillance data regarding prevalence of STIs and HIV is sparse as there is associated stigma, leading to hesitation of, and discrimination against, patients with STIs and HIV. Moreover, there are limited diagnostic facilities and only recent recognition of STIs as a major public health problem. 45
However, we need to define HRSB for the sake of clarity and in the interest of community/public health, because we are living in the era of rapid spread of STIs and HIV. Once clearly defined, we can target the population, and the behaviors in venereology and de-addiction clinics. So a tentative definition of “HRSB” would be “a behavior of initiation of sexual activity at an early age, engaging in unprotected or unnatural (anal/oral) sexual intercourse (or inconsistent condom use), having sexual intercourse with multiple partners (protected/unprotected), engaging in irregular or paid or incentive-driven sex, or sexual intercourse with injecting drug user or under the influence (especially intoxication) of psychoactive substances, which may result in sexually transmitted infections (including HIV/AIDS), unintended/early pregnancies (or abortions), or interpersonal or legal conflicts.”
With respect to high prevalence of HRSB in the context of substance use, some authors have made certain recommendations. First, sexual health assessment should be done as a part of routine clinical assessment for outpatients attending the clinics for treatment of their substance-use disorder. Second recommendation is at the level of training addiction specialists in the field of sexual health. Third, patients who are reported to be practicing HRSB should be encouraged to undergo voluntary HIV as well as other STIs testing. 36
With respect to the current literature, more studies are warranted in women substance users with regards to the rates of unintended pregnancies and abortions. There is a need to understand clinician’s comfort and knowledge in assessing and managing risky sexual behavior and STIs. Future studies should focus on measuring the prevalence across communities as well as clinical settings.
Conclusion
A concrete definition of HRSB with respect to substance use is lacking in the current literature. Behaviors which may be considered as HRSBs are as follows: unprotected intercourse, intercourse under influence of substances, intercourse with persons with injecting drug use, multiple sexual partners, early age of initiation of sexual intercourse, and intercourse with female sex workers/paid sex/casual sex. The ill effects of HRSB are STIs, HIV, unintended pregnancy, early pregnancy, and abortions. Literature shows high incidence of all the ill effects of HRSB in patients who are using substances as compared to general population. Further research is warranted to obtain a definition which has greater precision and clinical utility, and which can be integrated in preventive and promotive pursuits.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.