
Abstract
The diagnostic procedure of gastrointestinal endoscopy serves essential functions in handling gastrointestinal disorders. Classic endoscopic approaches encounter multiple problems because they depend on human operators and yield ambiguous results during lesion detection. The development of artificial intelligence systems has risen as an efficient technology to enhance diagnosis precision and procedural efficiency during endoscopic procedures. The objective of this review is to assess how artificial intelligence (AI) technology influences gastrointestinal (GI) endoscopic procedures for both lesion identification and classification, and malignant polyp identification, as well as clinical intervention operations. The research investigates obstacles that exist alongside AI implementation problems in clinical gastroenterological practices and determines forthcoming guidelines. A thorough literature survey was conducted through accessing databases, including PubMed alongside Scopus as well as ScienceDirect, Elsevier, and Springer. Studies after 2019 were evaluated for the AI performance in GI endoscopic examination. The use of AI in endoscopic visual examinations boosts both the diagnostic accuracy of esophagogastroduodenoscopy and colonoscopy lesions and exceeds traditional analysis methods. AI technology enhances predictions of malignant polyp status, which helps doctors make treatment decisions while lowering the number of unnecessary biopsies. Several obstacles, including technical boundaries and biased data, and regulatory obstacles, together with clinical implementation obstacles, still continue to exist. The advancement of artificial intelligence through GI endoscopy has led to an improvement of diagnostic outcomes and treatment efficiency alongside better clinical choice capabilities. AI will implement its complete role in routine clinical practice, but needs research about current challenges and regulatory adjustments, and technological improvements to boost patient outcomes.
Plain language summary
The objective of this review is to assess how AI technology influences GI endoscopic procedures for both lesion identification and classification and malignant polyp identification as well as clinical intervention operations. The research investigates obstacles that exist alongside AI implementation problems in clinical gastroenterological practices and determines forthcoming guidelines. A thorough literature survey conducted through accessing databases including PubMed alongside Scopus as well as ScienceDirect, Elsevier, and Springer. Studies after 2019 were evaluated for the AI performance in GI endoscopic examination. The use of AI in endoscopic visual examinations boosts both diagnostic accuracy of esophagogastroduodenoscopy and colonoscopy lesions and exceeds traditional analysis methods. AI technology enhances predictions of malignant polyp status which helps doctors make treatment decisions while lowering the number of unnecessary biopsies. Several obstacles including technical boundaries and biased data and regulatory obstacles together with clinical implementation obstacles still continue to exist.
Keywords
Introduction
Medicinal experts use gastrointestinal (GI) endoscopy as a fundamental diagnostic instrument to address different pathologies in the gastrointestinal system. Traditional endoscopic procedures are commonly used, but their adoption faces limitations because of inconsistent diagnosis rates and accuracy that depends on the endoscopic operator. The utilization of artificial intelligence (AI) within GI endoscopies presents itself as an advanced method to boost diagnostic accuracy, together with process operational speed. Machine learning and deep learning algorithms operating under AI have proven their usefulness in both medical imaging and endoscopic applications.1,2 Complex visual data assessment by these technologies leads to improved GI lesion detection and characterization, along with superior accuracy than traditional approaches. 1 AI significantly improves GI endoscopy operations because it conducts instantaneous procedural analysis. The predictive capability of these systems improves both lesion detection and helps doctors foresee histopathological results, which may lower biopsy requirements with their related complications. AI applications for endoscopic quality control assume two key functions: they enforce standard operating procedures and reduce human mistakes in endoscopic procedures. 3
This review examines the existing findings that demonstrate how AI systems improve GI endoscopic examination accuracy as well as operational performance levels. The exploration of this research involves AI-enabled detection and classification of features within esophagogastroduodenoscopy and colonoscopy procedures, and the examination of AI prediction capabilities regarding polyp malignancies and endoscopic intervention guidance, together with AI limitations in clinical gastroenterology and its future potential.
AI-assisted diagnosis and classification of lesions
AI has substantially developed gastrointestinal endoscopy by improving lesion identification and categorization during esophagogastroduodenoscopy (EGD) and colonoscopy examinations.
Esophagogastroduodenoscopy
Recent innovative technologies have produced AI systems to assess both the quality and achieved extent of EGD procedures (shown in Figure 1). Bioengineered systems display advanced capability for real-time gastric site detection, providing endoscopists with assessment capabilities that might evolve into a professional education resource. 4 AI assists in EGD procedures to detect and diagnose early-stage gastrointestinal cancers, together with other upper gastrointestinal lesions. Medical research reveals that AI solutions in EGD aim to detect cancer cells as well as evaluate invasion depths and perform diagnostic predictions regarding tissue pathology, and detect Helicobacter pylori strains. 2 The accuracy of diagnostic results depends on having full visualization during an EGD procedure. AI systems designed for blind spot monitoring serve to enhance the quality assessment of EGD procedures in real time. 5 AI systems enable the enhancement of EGD photodocumentation by providing a thorough upper gastrointestinal tract examination during the procedure. 6 Research on AI-based systems demonstrates their successful capability to perform real-time high-quality photodocumentation during EGD procedures. An AI system exhibited high precision for detecting anatomical points in medical imagery and generated enhanced pictures with superior clarity than human endoscopy results while improving procedural visibility. 7 AI presents effective ways to help medical staff provide computer-assisted diagnosis while performing EGD examination quality checks. A review provided essential information for EGD screening quality assurance by summarizing cutting-edge evidence with limitations and AI potential in EGD quality control assessment. 8

Role of artificial intelligence in esophagogastroduodenoscopy.
AI technologies developed for EGD help physicians identify and classify lesions present in the esophagus, along with stomach and duodenum tissues, and upper GI tract neoplastic lesions. The deep learning systems use digital training with extensive images to detect Barrett’s esophagus and early gastric cancer, and duodenal neoplasms.7,9 Research shows that AI supports EGD procedures in making better lesion detections versus conventional methods, which strengthens diagnosis timeliness and improves treatment results.5,8 The combined results from 23 research studies showed AI detection systems achieved 0.96 area under the curve success rates for identifying gastric neoplastic lesions. The performance figures of AI systems exceeded traditional endoscopist results since they reached an Area Under the Curve (AUC) measurement of 0.87 compared to AI’s superior diagnostic precision at 0.96. Research has validated that AI operates efficiently when detecting different conditions affecting the esophagus. AI detection of Barrett’s esophagus neoplastic lesions attained a diagnosis accuracy level of 0.96 in combination with squamous cell carcinoma diagnosis reaching 0.88 as shown in the same meta-analysis. The diagnostic performance of AI systems using narrow-band imaging (NBI) exceeded the performance of systems using white-light imaging, as demonstrated by AUC results of 0.92 versus 0.83, respectively (shown in Table 1). 10 Although AI models have demonstrated high accuracy in detecting upper GI lesions, the reliance on retrospective or idealized image datasets raises concerns. In practice, poor mucosal visualisation, mucosal inflammation, or motion artifacts may reduce model accuracy. The lack of standard protocols for image acquisition and AI integration further hampers reproducibility in community settings.
Performance of artificial intelligence in esophagogastroduodenoscopy.
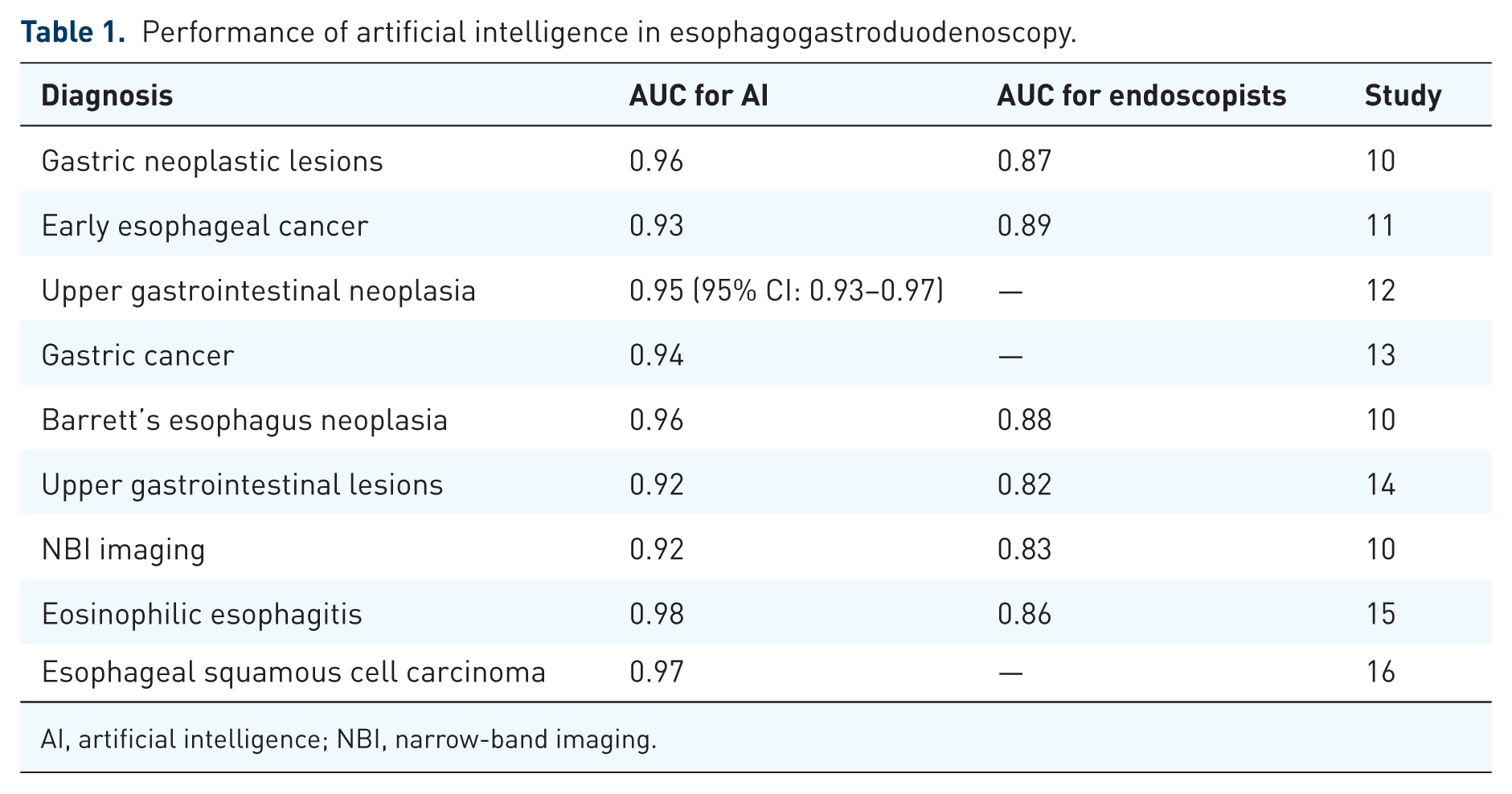
AI, artificial intelligence; NBI, narrow-band imaging.
Colonoscopy
The application of AI technology has improved major aspects of colonoscopy, which resulted in better detection capability for polyps, along with improved characterization abilities and enhanced procedural stability. The combination of AI with colonoscopy enables better examination results through higher adenoma detection rates (ADRs) than non-AI approaches do. A large sample study that included 3059 symptomless patients showed a 39.9% ADR when using AI technology rather than the 32.4% ADR achieved without AI technology. Independent of their expertise, both expert and non-expert endoscopists noted this improvement. 17 AI systems analyze polyp histology in endoscopic procedures by differentiating between cancerous and non-cancerous lesions. The research showed that AI achieved an 82% correct detection rate for identifying neoplastic or non-neoplastic polyps with an 80% accurate identification. 18 AI technology enables the monitoring and quality enhancement of colonoscopy procedures as part of its application. The integration of AI into colonoscopy practices leads to better polyp detection rates by decreasing the amount of missed colorectal neoplasia cases. Research must continue to determine both the financial effectiveness and long-term advantages of AI-assisted colonoscopy in lowering cancer frequencies. 19
Professional use of AI technology continues to increase for colorectal polyp detection and classification purposes during colonoscopy procedures. AI systems function under the names of computer-aided detection (CADe) and computer-aided diagnosis (CADx) to assist with polyp detection during screening procedures.20,21 AI detection systems show a 95% (95% CI: 89–98) rate of successfully detecting colorectal polyps. The AI-assisted classification technique demonstrated 92% sensitivity (95% CI: 88–95) along with 82% specificity (95% CI: 71–89) and an accompanying AUC value of 0.94, which signifies its precision in distinguishing neoplastic from non-neoplastic polyps. The sensitivity level of AI systems for detecting diminutive polyps (⩽5 mm) reaches 95% (95% CI: 94–97) while their specificity reaches 88% (95% CI: 74–95), and both metrics exhibit an AUC of 0.97. The study findings indicate that AI technology succeeds in helping endoscopists identify and remove polyps in real time therefore diminishing their missed detection rates and enhancing patient results. 22 Modern AI systems demonstrate proven capability to raise the essential quality measurement of adenoma detection rate (ADR) during colonoscopy procedures.23,24 This randomized controlled study demonstrated that using an AI system produced a 9% rise in the ADR compared to a normal colonoscopy. Evaluations showed significant progress in detecting polyps smaller than 10 mm because AI successfully spots small lesions that standard procedures tend to miss. 25
Recent advancements also demonstrate AI’s potential to assess quality metrics during colonoscopy. Systems have been developed to automatically evaluate bowel preparation quality, detect key anatomical landmarks such as the appendiceal orifice, and monitor withdrawal stability in real time. Furthermore, surface area measurement tools using AI may improve mucosal visualization assessment, leading to more standardized and complete examinations. These applications extend AI’s value beyond detection and classification into quality assurance and performance benchmarking. While CADe systems have consistently shown increased ADR in RCTs, real-world implementation often underperforms due to workflow disruptions, endoscopist fatigue, and alarm fatigue from false positives. Furthermore, many AI systems are trained on high-quality, well-annotated datasets, which may not reflect the variability and noise seen in actual clinical practice. Studies rarely report how these tools perform across diverse patient populations and hospital types, limiting their generalizability.
Why AI has not fully worked yet
Medical specialists use artificial intelligence to improve both diagnostic results and procedural effectiveness within gastrointestinal endoscopy procedures. Various challenges and restrictions need resolution to maximize artificial intelligence potential in clinical gastroenterology practice (shown in Figure 2). The training success of AI systems depends on proper data annotation, which ensures high-quality data collection. The use of heterogeneous datasets in AI applications becomes problematic because of non-standardized data acquisition and endoscopic equipment, together with imaging protocols. AI application reliability with generalization across different clinical environments depends on standardized data obtaining and annotation rules. The detection and classification of lesions through AI requires algorithm development that differentiates real abnormal findings from procedural artifacts.26–28 The use of AI systems in clinical operations produces substantial moral dilemmas because it affects patient confidentiality, together with medical information protection. Clinical AI systems need extensive access to patient-sensitive information, which creates elevated possibilities of data breaches. So that patients trust healthcare services and regulators can be satisfied, and the implementation of protective data management strategies must coincide with definitive procedures that specify how data should be used. AI systems that operate in healthcare need thorough ethical principle review during development and deployment because they could transfer existing biases present in healthcare data.29,30 Federal authorities remain in the process of developing framework policies to regulate AI-based medical devices. The process to establish agreed-upon validation approaches while pursuing regulatory licensing requires both lengthy periods of time and extensive complexity. Standardized safety and effectiveness tests for AI systems will enable their successful adoption into clinical care routines. Clinical trials consisting of comprehensive performance validation must be conducted, while guidelines ought to be created for tracking and upgrading AI algorithms to preserve their clinical utility and safety aspects.31,32

Challenges to artificial intelligence in clinical gastroenterology practice.
Systems trained using biased datasets will generate outcomes with similar discrimination, which affects minority groups. Developing fair AI systems requires training datasets that represent a diversified range of population and clinical demographics because they enable applicability across all patient groups. 33 AI development requires the implementation of algorithmic strategies that detect as well as reduce biases simultaneously with data source diversity. Inserting AI tools into clinical workflows demands that healthcare providers face major challenges to prevent interruptions during operations. Healthcare professionals need training to operate AI systems successfully, but some staff members do not want to work with new technological platforms. The implementation of friendly interfaces coupled with extensive training programs helps healthcare professionals accept new systems.34,35 AI applications need to match end-user needs and preferences to improve clinical usefulness, combined with usability.
Polyp malignancy prediction
During endoscopic procedures, AI models serve as diagnostic tools to differentiate between polyp types as either neoplasms or non-neoplasms. The AI recognition network demonstrates an evaluation performance of 99.9% sensitivity and 99.4% specificity for detecting colorectal polyps. The following stage of analysis identified neoplastic and non-neoplastic polyps with 82% sensitivity and 80% specificity. Real-time analysis has been proven to cut down on unneeded biopsies along with their related complications. 18 , 36 AI systems help endoscopic professionals determine suitable therapeutic decisions during visual examinations. The assessment function of artificial intelligence enables precise polyp examinations, which produce data to support physicians' procedure selection between submucosal dissection and endoscopic mucosal resection. Furthermore, the guidance enables total removal of harmful lesions together with minimalization of potential dangers. AI provides 88% accurate size estimation for polyps, which helps doctors determine the necessary extent of resection during surgical procedures.18,37 Although CADx systems show high accuracy in distinguishing polyp histology, there remains concern over their clinical use in place of biopsy, especially when models are deployed without well-calibrated confidence thresholds or in heterogeneous settings where training data may not apply.
Future directions
AI in GI endoscopy is set to revolutionize by enhancing the precision of therapeutic interventions and diagnostic protocols. The future of AI in this field encompasses different key areas (shown in Table 2). The analysis capabilities of AI, together with its real-time feedback potential, help speed up endoscopic procedures and minimize the requirement for invasive biopsies and their connected adverse events. 1 AI systems used during endoscopy give instant analysis that helps identify abnormalities quickly, which enhances both diagnoses and procedural operations. Therapeutic endoscopy will benefit from AI integration because it will boost the accuracy of treatments. During endoscopic procedures, AI technology aids doctors to make live decisions for better therapeutic results. Furthermore, artificial intelligence-assisted systems help to advance the gastrointestinal therapeutic modalities, including robotic endoscopic surgeries or artificial intelligence-led laser therapies, and improve patient safety with treatment precision. 38 Future GI endoscopy shows holds good potential because AI operates with robotics tools and advanced imaging systems. Advanced endoscopic systems will be possible through this technology combination, which aims to perform intricate diagnostics alongside therapeutic surgical tasks with superior accuracy,39,40 such as robotic endoscopy enhanced by artificial intelligence could enable minimally invasive procedures with short healing periods and improved precision.
Challenges and solutions for artificial intelligence in GI endoscopy.

AI, artificial intelligence; GI, gastrointestinal.
The education of endoscopists, along with their training, should depend significantly on AI-driven simulation technology. The tools enable medical professionals to train their abilities through different real-world situations, which ultimately results in better clinical outcomes. The system provides personalized feedback along with performance metric evaluations, which allows professionals to continue their learning and advance their skills.40,41 AI technologies for GI endoscopy will transform in the future through the unification of information from multiple sources, including endoscopic images and medical data, and genomic testing results.1,42 Such complete methods enable better medical diagnoses and individualized treatment strategies. AI analysis of endoscopic visuals together with histopathological data strengthens the ability to identify and describe GI lesions.
Conclusion
The integration of artificial intelligence into gastrointestinal endoscopy has shown considerable promise in improving diagnostic accuracy, therapeutic decision-making, and procedural efficiency. AI systems have demonstrated strong performance in classifying and detecting lesions, particularly for conditions like Barrett’s esophagus, colorectal polyps, and early gastric cancer. These technologies offer the potential to support advanced interventions such as ESD and EMR and reduce unnecessary biopsies. However, despite encouraging results from randomized controlled trials and offline studies, real-world implementation has not consistently reproduced these benefits. Variability in clinical settings, workflow integration challenges, and heterogeneous patient populations continue to limit AI’s full impact in practice. Furthermore, current AI models often rely on idealized or retrospective datasets, raising concerns about their safety and generalizability in routine care. To move from proof-of-concept to clinical utility, the field must prioritize prospective, multicenter validation studies, alongside transparent regulatory frameworks and rigorous ethical oversight. Training clinicians, developing explainable AI tools, and standardizing data acquisition will be critical to ensuring effective and safe adoption. While AI holds transformative potential for gastrointestinal endoscopy, realizing its full clinical value will require not only technological innovation but also strategic alignment with the realities of clinical practice, health system readiness, and patient safety.