
Abstract
Background:
The faecal immunochemical test (FIT) is an immunoassay used to detect human blood in the stool. The role of FIT as a screening tool for small bowel pathology remains unclear.
Objectives:
This study aimed to investigate the role of FIT in predicting small bowel pathology in patients with iron deficiency anaemia (IDA).
Design:
This was a single tertiary centre prospective study. The inclusion criterion was adults (⩾18 years and <80 years) with IDA who were referred to secondary care for endoscopic investigations.
Methods:
All patients had a FIT test done in primary care. Eligible patients were invited to have a small bowel capsule endoscopy (SBCE) prior to endoscopy. Patients with subsequent upper or lower gastrointestinal tract malignancy were excluded from the study. IDA was defined as a Hb < 131 g/L for men and <110 g/L for women with ferritin <30 µg/L and/or iron levels <11 µmol/L. A further 100 patients with recurrent/refractory IDA who did not have a FIT test done and had an SBCE were used as the control group.
Results:
In total 179 patients were included in the final analysis with a median age of 64.5 years (interquartile range (IQR 51–75)); haemoglobin 101 (IQR 90–111) and ferritin 11(7–20). In the prospective FIT group of 79 patients, there were 35 (44%) patients with significant findings on SBCE which was classed as contributing to IDA. These findings included angioectasia in n = 21 (26.6%) patients which was the most common finding. The other findings included erosions and ulcers = 5 (7.6%); inflammatory strictures = 3 (3.8%); active Crohn’s n = 1 (1.3%); visible blood with no clear source n = 3 (3.8%) and bleeding angioectasia n = 1 (1.3%). A positive FIT (>10) had a sensitivity, specificity, positive predictive value and negative predictive value of 34.29%, 54.55%, 37.5% and 51.08%, respectively. In the control group (n = 100), 37% of the patients had significant pathology on SBCE. On logistic regression, age (OR 1.06; 95% CI: 1.03–1.11) was the only factor related to the probability of having a positive finding on SBCE.
Conclusion:
Over a third of the patients with IDA have significant findings on SBCE. However, in this study, we did not find that FIT conferred any additional benefit in the detection of small bowel pathology.
Introduction
The faecal immunochemical test (FIT) is an immunoassay used to detect human blood in the stool. 1 It has largely replaced the traditional faecal occult blood tests (FOBTs) due to higher sensitivity for colorectal cancer as well as advanced neoplasia.2–5 It is also thought to be more specific for distal gastrointestinal bleeding and the results are not affected by the use of non-steroidal anti-inflammatory drugs (NSAID) and oral anticoagulation.1,3,6 Overall, the acceptability of FIT is higher compared to traditional FOBT.7,8 Currently, FIT is used for colorectal cancer (CRC) screening and also for risk-stratifying patients with IDA in England.9,10 We also know that in up to 60% of the individuals with a positive FIT, no significant colorectal lesion is identified. This raises the possibility of the lesions being located in the small bowel.11–13 Currently, the role of FIT as a screening tool for small bowel pathology in patients with iron deficiency anaemia (IDA) remains unclear.
IDA is a common clinical problem and it occurs in 2%–5% of men and postmenopausal women in the developed world.14–17 Although most studies for anaemia include only patients with recurrent/refractory IDA, it has been shown that potentially significant small bowel pathology is identified in up to 60% of the cases.14,18
Capsule endoscopy is an accepted first-line modality for investigating the small bowel, particularly in the setting of obscure GI bleeding. 19 It is minimally invasive and very well tolerated. In a metanalysis, small bowel capsule endoscopy (SBCE) was superior to push enteroscopy as well as small bowel barium radiography for diagnosing clinically significant pathology in patients with obscure GI bleeding. 20 Currently, there are no biomarkers available that could be used to triage these patients who are being referred for an SBCE.
This study aimed to investigate the role of FIT in predicting small bowel pathology in patients with iron deficiency anaemia (IDA) and negative bidirectional endoscopy.
Methods
Study design and patient selection
This was a single tertiary centre prospective study conducted in Sheffield, United Kingdom. The inclusion criterion was adults (⩾18 years and <80 years) with the presence of IDA who were referred for endoscopic evaluation (oesophagogastroduodenoscopy + colonoscopy) based on national guidelines. 14 Prospective patients were recruited from January 2022 to January 2024. Patients identified with IDA in primary care are advised to have a FIT test done before being referred to secondary care. This is routine practice for risk stratification of the referrals. All patients recruited into the study had IDA and a FIT test done in primary care. SBCE was performed prior to their endoscopic investigations in the prospective group. Patients with subsequent upper or lower gastrointestinal tract malignancy were excluded from the study as this was considered to be the most likely cause of IDA. IDA was defined as a Hb < 131 g/L for men and <110 g/L for women with ferritin < 30 µg/L and/ or iron levels <11 µmol/L. A control group of 100 adult patients (⩾18 years and <80 years) who had a SBCE for IDA (who did not have a FIT test done in primary care) were collated from the existing SBCE database (January 2022–January 2024). The database contains all patients who have had a SBCE at Sheffield Teaching Hospitals. Search terms like IDA and anaemia were used to identify eligible patients. All patients included in the control group were referred for an SBCE for further evaluation of their recurrent/refractory IDA. Patient demographics and medical history were collected to look for the correlation between age, sex, comorbidities (ischaemic heart disease, diabetes, hypertension, atrial fibrillation and stroke), medication (anticoagulation, antiplatelet, NSAID) and the level of haemoglobin on small bowel pathology. Sample size calculation was based on previous studies which have used a similar sample size. The reporting of this study conforms to the STARD checklist. 21
Small bowel capsule endoscopy
AnX Robotica magnet system and Navicam capsule (single camera capsule, frame rate 2–6/s: Wuhan, China) were used for small bowel examinations. All patients were offered the capsule endoscopy within 1 week prior to their endoscopic procedures. All capsule studies were read by a single professor in gastroenterology with decades of experience in endoscopy and small bowel capsules (>1000 lifetime CE reported). The reader was blinded to the FIT results and the endoscopic findings. A capsule endoscopy was deemed positive if it identified small bowel pathology which could potentially cause IDA. These lesions were classified as angioectasias, ulcers, erosions, strictures, active Crohn’s and fresh blood of unknown aetiology. All identified lesions were classified using the adapted Saurin classification and only those lesions with a suspected bleeding potential (P1 – angioectasia, erosions and ulcers) and a high bleeding potential (P2 – bleeding angioectasia, active Crohn’s, inflammatory stricture, fresh blood with no clear source, neoplasia, large eroded polyps) were included in the final analysis.22,23
Statistical analysis
Statistical analyses were conducted using GraphPad Prism version 10.0.2 for Mac (GraphPad Software, San Diego, CA, USA). A two-tailed p-value less than 0.05 was considered statistically significant. Descriptive statistics were used to summarise continuous data as median (IQR) and categorical data as total numbers (percentages). Fisher’s exact test was used to compare the diagnostic yield of SBCE in IDA. The correlation between different variables such as age, sex, comorbidities, medication and level of IDA was assessed with small bowel pathology using multivariant logistic regression analysis. The sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) in predicting small bowel pathology were calculated for different levels of FIT.
Results
Patient characteristics
There were 179 patients in total. Out of these, 88 patients were recruited prospectively. Nine patients were excluded from the prospective group after their endoscopic evaluation because of malignancy (colorectal carcinoma = 8, metastatic gastric lymphoma = 1). There were 79 prospective patients and 100 controls included in the final analysis (Figure 1). The median age was 64.5 years (IQR 51–75); haemoglobin 101 g/L (IQR 90–111) and ferritin µg/L 11(7–20). There were 54% of female patients in total. There were 16 patients on NSAIDs, 37 on anticoagulation and 12 on antiplatelets at the time of their investigations. A detailed breakdown of patient characteristics in the prospective and the control group has been mentioned in Table 1.

Flowchart shows the selection of patients for the study.
Patient characteristics of Group 1 (IDA and FIT) and Group 2 (IDA and no FIT).

FIT, faecal immunochemical test; IDA, iron deficiency anaemia; IQR, interquartile range; NSAID, non-steroidal anti-inflammatory drugs.
Capsule endoscopy results
There were 179 patients with IDA and significant small bowel pathology was identified in 72 (40.2%) of the patients. Group 1 included prospective patients with IDA who had a FIT test done in primary care. Group 2 included a retrospective cohort of control patients with recurrent or refractory IDA and no FIT sampling was done in primary care.
In Group 1, there were 35 (44.3%) patients with significant findings on SBCE which was potentially contributing to IDA. These findings included angioectasia in n = 21 (26.6%) patients which was the most common finding. The other findings included erosions and ulcers = 6 (7.6%); inflammatory strictures = 3 (3.8%); active Crohn’s n = 1 (1.3%); visible blood with no clear source n = 3 (3.8%) and bleeding angioectasia n = 1 (1.3%). In Group 2, there were 37 (37%) patients with significant findings on SBCE which was potentially contributing to IDA. These findings included angioectasia in n = 20, bleeding angioectasia n = 1, new Crohn’s disease, neoplasia n = 4, erosions and ulcers n = 7, large eroded polyp n = 3 and ulcerated stricture n = 1. There was no significant difference in the diagnostic yield between the two groups (95% CI: 0.73–2.51; p = 0.35) (Table 2). In some patients, more than one finding was identified on SBCE. In these cases, the P2 pathology was included in the analysis for diagnostic yield. No patients had more than one P2 pathology.
Small bowel findings detected by SBCE in patients with IDA and FIT results (Group 1).
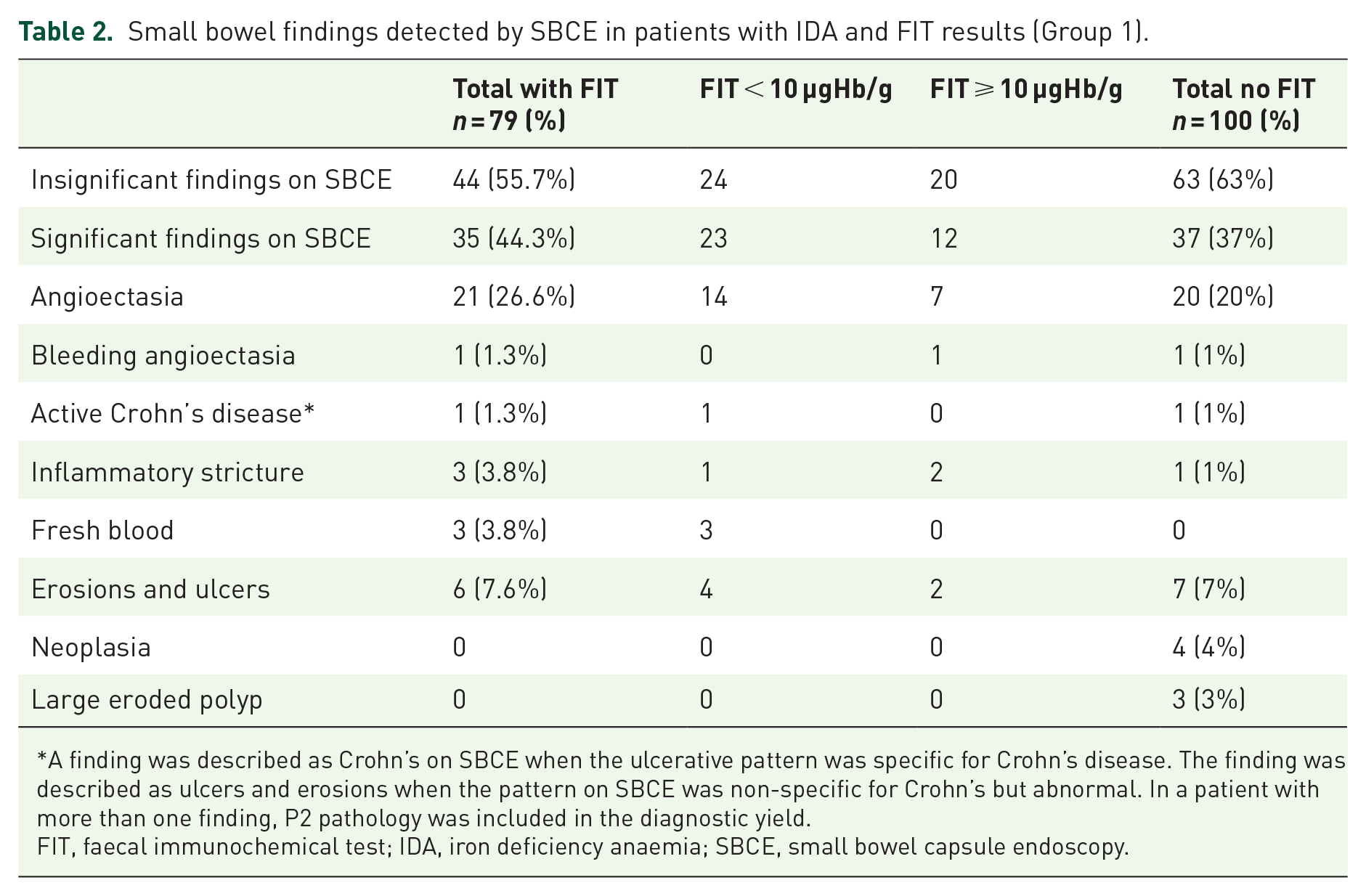
A finding was described as Crohn’s on SBCE when the ulcerative pattern was specific for Crohn’s disease. The finding was described as ulcers and erosions when the pattern on SBCE was non-specific for Crohn’s but abnormal. In a patient with more than one finding, P2 pathology was included in the diagnostic yield.
FIT, faecal immunochemical test; IDA, iron deficiency anaemia; SBCE, small bowel capsule endoscopy.
FIT results and capsule endoscopy
In all, 79 patients had IDA and a FIT test done. The median time from obtaining FIT results to complete investigations (SBCE and dual endoscopy) was 8 weeks. All patients with a FIT level >10 µgHb/g were investigated within 4 weeks. In total, there were 35 (44%) patients with significant findings on SBCE which was the most likely contributing to IDA. Out of these, 12 patients had a FIT > 10 µgHb/g and 23 had a FIT < 10 µgHb/g (p = 0.36). The sensitivity of FIT > 10 µgHb/g was 0.37 (95% CI: 0.25–1.63); specificity 0.51 (0.37–0.64); PPV 0.34 (0.21–0.50); NPV 0.54 (0.40–0.68) for detecting small bowel pathology. These results were also calculated for different FIT levels as shown in Table 3.
Performance of FIT for the detection of significant small bowel lesions.

FIT, faecal immunochemical test; NPV, negative predictive value; PPV, positive predictive value.
Several variables were significantly associated with positive findings using univariant logistic regression analysis on our retrospective cohort of 100 patients. Age (OR 1.06; 95% CI: 1.03–1.11) was the only factor that was significant in multivariable logistic regression for the small bowel pathology in patients with IDA (Table 4).
Factors predicting small bowel pathology.

AF, atrial fibrillation; CKD, chronic kidney disease; HTN, hypertension; IHD, ischaemic heart disease; T2DM, type-2 diabetes. The bold numbers are the significant values hence written in bold.
Discussion
In the study, we have shown that significant small bowel pathology was identified in over a third of the patients with IDA on SBCE. There was also no significant difference in the diagnostic yield between the prospective group with IDA (first presentation and recurrent IDA) and the retrospective group with recurrent and/ or refractory IDA. All identified lesions were standardised using the adapted Saurin classification and only those lesions with a suspected bleeding potential (P1) or a high bleeding potential (P2) were included in the final analysis. Our findings are supported by previous literature which has consistently shown a high diagnostic yield of small bowel pathology in patients with IDA.18,24,25 In spite of these findings, small bowel investigations are only recommended for patients with recurrent or refractory anaemia. 14 The study has also shown that age is a predictor of small bowel pathology which is also supported by previous literature suggesting that there is an increased likelihood of small bowel pathology in older patients with IDA. 26
In the study, FIT has a low sensitivity, specificity, PPV and NPV for small bowel pathology at all levels. These findings are supported by a previous meta-analysis which included five studies. In the meta-analysis, the overall sensitivity for SB pathology in patients with a FOBT test was 0.60 (95% CI: 0.50–0.69) and specificity was 0.72 (95% CI: 0.52–0.86). 27 When only the four studies that used FIT in the analysis were included the sensitivity of FIT for SB pathology on CE was 0.48 (95% CI: 0.36–0.61) and the specificity was 0.60 (95% CI: 0.42–0.76).27–31 A more recent study by Judge et al. has shown that a combination of anaemia and positive FIT was statistically significant in predicting SB pathology (R = 0.39, p = 0.009); PPV of 66.7%, and an NPV of 82.1% (OR 9.14, 95% CI: 1.39–60.12, p = 0.025). 32 The reason for this difference could be the timing of the FIT test. Judge et al. performed all FIT tests within 24 h of the SBCE. Small bowel lesions such as angioectasia do bleed intermittently and hence the timing of the FIT can potentially have an impact on lesion detection. Previous literature suggests that in patients with overt GI bleeding, the diagnostic yield of SBCE is higher when performed close to the bleeding episode.33,34 In a study by Kobayashi et al., 30 the timing of the FIT influenced the association between FIT results and SB pathology in patients with obscure bleeding. In our study, although the diagnostic yield of SBCE was comparable to other studies, FIT had low accuracy in predicting small bowel pathology. This could be because, in our cohort of patients, the median time from obtaining the FIT results to having endoscopic investigations was 8 weeks.
One of the limitations of our study is the small sample size of the FIT group. However, the diagnostic yield of potentially significant pathology was comparable to previous studies.
Currently, there is no validated tool used for grading capsule endoscopy referrals. With the expanding role of CE, there is an increasing demand for rationalising these referrals and also for grading them as urgent or routine.
Conclusion
Patients with IDA have a high diagnostic yield on SBCE. There is a pressing need for biomarkers to help triage SBCE referrals; however, FIT is not a reliable biomarker for the presence of small bowel pathology in patients with IDA.