
Abstract
Objective:
Endoscopic retrograde cholangiopancreatography (ERCP) in patients who have undergone Billroth II gastroenterostomy (B-II GE) has been challenging, requiring flexibility in technical approaches during execution. The study aims to assess the effectiveness of enhanced techniques in performing ERCP on this patient group in Vietnam.
Method:
A total of 42 Vietnamese patients with B-II GE performed an ERCP using a duodenoscope or a modification of ERCP equipment (a cap-fitted regular forward-viewing endoscope) if the former failed. The effectiveness and safety of the ERCP technique were assessed, particularly in patients who underwent the forward-viewing endoscope method.
Result:
A total of 39 out of 42 patients had the Vater’s papilla identified, among whom 12 patients (30.8%) achieved successful cannulation into the bile duct using a side-viewing endoscope, significantly lower than the success rate using a forward-viewing endoscope (25/27, counted 92.6%, with p < 0.001). After successful cannulation, the rate of stone clearance, the procedural time, and the hospitalization duration of the patients were equivalent between the two methods and were not dependent on the number or size of the stones. On the other hand, post-ERCP complications in patients utilizing forward-viewing endoscopy included acute pancreatitis (22.2%), post-sphincterotomy bleeding (3.7%), septicemia (4.8%), and perforation (0%). These complications were mild and amenable to conservative endoscopic and medical management, and no mortality was observed. The rates of complications and adverse events after ERCP are comparable between the two treatment methods, even though the end-viewing endoscope is used after the failure of the side-viewing endoscope.
Conclusion:
Alter ERCP utilizing a cap-fitted forward-viewing endoscope can be a primary choice for treating common bile duct stones in patients with a Billroth II gastric resection history because of high efficacy and acceptable complications. It requires a high level of procedural expertise that requires multiple training sessions.
Plain language summary
Endoscopic retrograde cholangiopancreatography (ERCP) treating common bile duct stones in Vietnamese patients with a history of Billroth II gastrectomy is challenging due to changes in gastric anatomy and the limited visibility of the side-viewing endoscope. The researchers tried different techniques, including using a special type of forward-viewing endoscope with cap assistance. We found that using a forward-viewing endoscope was more successful in reaching certain areas compared to a side-viewing one. Although there were some complications, they were manageable, and the overall results were similar between the two methods. The study suggests that using a modified approach with a forward-viewing endoscope with cap assistance can be a good option for treating common bile duct stones in patients with a history of Billroth II gastric resection, but it requires skilled practitioners.
Keywords
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) has been a remarkable technological advance in gastrointestinal endoscopy over the past 40 years. It has replaced surgery in most patients with common bile duct stones and treated several pancreatic diseases. 1 ERCP is almost 100% successful in patients with normal gastrointestinal anatomy once the papilla is reached 2 ; however, in terms of patients with Billroth II gastroenterostomy (B-II GE) who often face challenges in performing stone extraction using retrograde pancreaticobiliary endoscopy with a side-viewing endoscope due to anatomical changes and a higher risk of complications when accessing the Vater’s papilla. Therefore, biliary complications such as stenosis or stones are often treated surgically or through the percutaneous transhepatic approach. A few reported cases of using a conventional duodenoscope or double-balloon enteroscopy to perform cannulation in patients after B-II GE. 3 Meanwhile, the use of a forward-viewing endoscope to treat bile duct stones in patients with a history of Billroth II reconstruction may be a good option when performing ERCP, as its effectiveness and safety have been reported by several authors.4–7 However, the routine use of this technique for patients with a surgical history of gastric resection, particularly those with B-II GE, remains a subject of debate.
In Vietnam, ERCP has been popular for 20 years and is performed at central and provincial hospitals. However, applying the ERCP technique in patients with Billroth II gastrectomy is still a significant challenge. ERCP technique for patients with gastrectomy is not widely practiced and can only be performed at large centers with experienced interventionists. Moreover, using a front-viewing endoscope for patients with B-II GE still lacks data. Therefore, this study aims to evaluate the efficacy and safe results of the improved ERCP technique in patients who have had B-II GE in Vietnam.
Methods
Patients
A total of 42 patients with common bile duct (CBD) stones and prior B-II GE between January 2018 and July 2022 at our department were enrolled in this study. Among them, four patients had undergone Billroth II for gastric cancer.
Inclusion criteria
Patients with a history of Billroth II gastric surgery presented with biliary stones based radiographic or biochemical evidence of biliary obstruction upon admission. The study population’s demographic, clinical, and laboratory data were collected from medical records. Medical record data, including sex, age at the time of the procedure, etiology of cirrhosis, cardiovascular disease, pulmonary diseases, medication related to bleeding tendency, pre-procedure laboratory values, ERCP indications, procedural details, and procedure-related adverse events, were reviewed.
Exclusion criteria
Patients underwent gastric surgery without Billroth reconstruction or showed no evidence of biliary stones.
Methods
The study was designed as a retrospective study. The flow diagram is presented in Figure 1. ERCP was started with a gastroscope to look for the papilla by a forward viewing endoscope, followed by navigation by a guidewire if the former was victorious. After that, cannulation was attempted with a duodenoscope. The second option was a forward-viewing endoscopy with cap-assisted (CV 190, CV 170, Olympus, Tokyo, Japan) if the duodenoscope had not worked. 8 The specialized instruments in biliary endoscopy include a cap fitted to the distal end of an endoscope. We used Clevercut3 (Olympus, Center Valley, PA, USA) as a catheter endoscopic sphincterotomy, a Guidewire 0.025 in and 0.035 in (Jagwire™, Boston Scientific, Natick, MA, USA), a Biliary dilator balloon with a diameter of 6 or 8 mm (MAX FORCE, Boston Scientific, Natick, MA, USA), and a stone retriever basket (Trapezoid™ RX, Boston Scientific, Natick, MA, USA). Endoscopic sphincterotomy was performed by either normal sphincterotomy or pre-cut sphincterotomy (Microknife™ XL, Boston Scientific, Natick, MA, USA). Once the chosen duct was selectively cannulated after evaluating the papilla, either a cholangiogram or a pancreatogram was obtained fluoroscopically with an injection of contrast medium into the duct. Endoscopic biliary stenting was carried out using plastic stents conventional 5 or 7 Fr double pigtail stents (Cook Medical, Limerick, Ireland), or removing a bile duct stone. All patients were sedated with intravenous anesthesia (diazepam and pethidine), along with continuous monitoring of blood pressure, heart rate, and oxygen saturation. All patients received intravenous hyoscine butylbromide for inhibiting duodenal spasms.
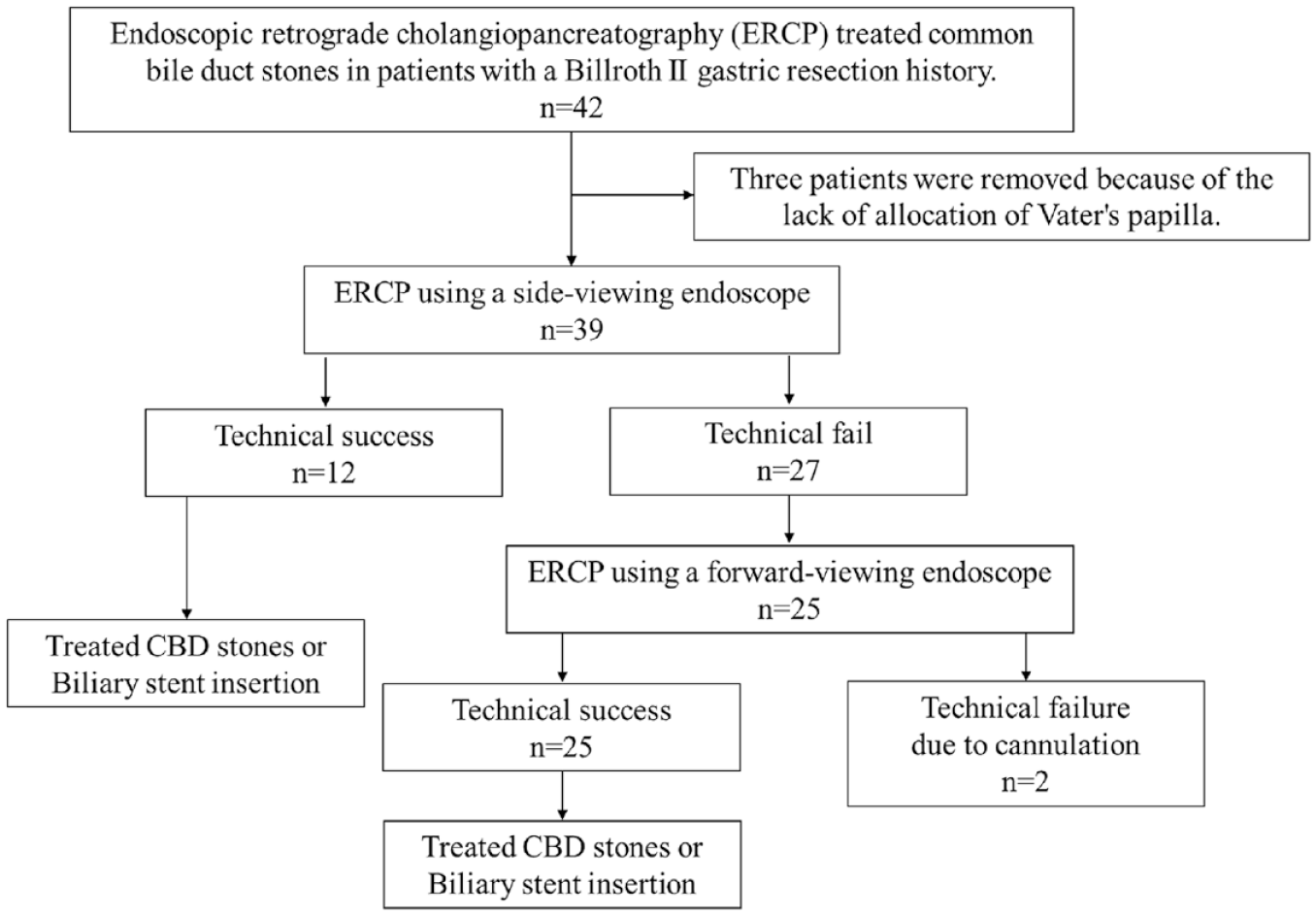
Flow diagram of the study.
Six hours after the ERCP and at 6 a.m. of the next day of the procedure, blood chemistry, including serum amylase, lipase, and total bilirubin level, and simple abdominal radiography were performed for evaluating post-ERCP pancreatitis, cholangitis, and bowel perforation. The adverse events of post-ERCP were defined following the ASGE guideline. 9
The results were evaluated as to the following points: the success rate of reaching the papilla of Vater and the time required, the success rate of selective cannulation of the bile duct, duct clearance, and early complications.
Statistical analysis
Statistical analyses were performed using SPSS version 25.0 (SPSS Statistics, IBM, Armonk, NY, USA) and Gradpad Prism 9.0 software (http://www.graphpad.com) for rates of selective cannulation of the bile duct, complete duct clearance, and early complications. Significance was set at p < 0.05.
Results
Baseline characteristics of B-II GE
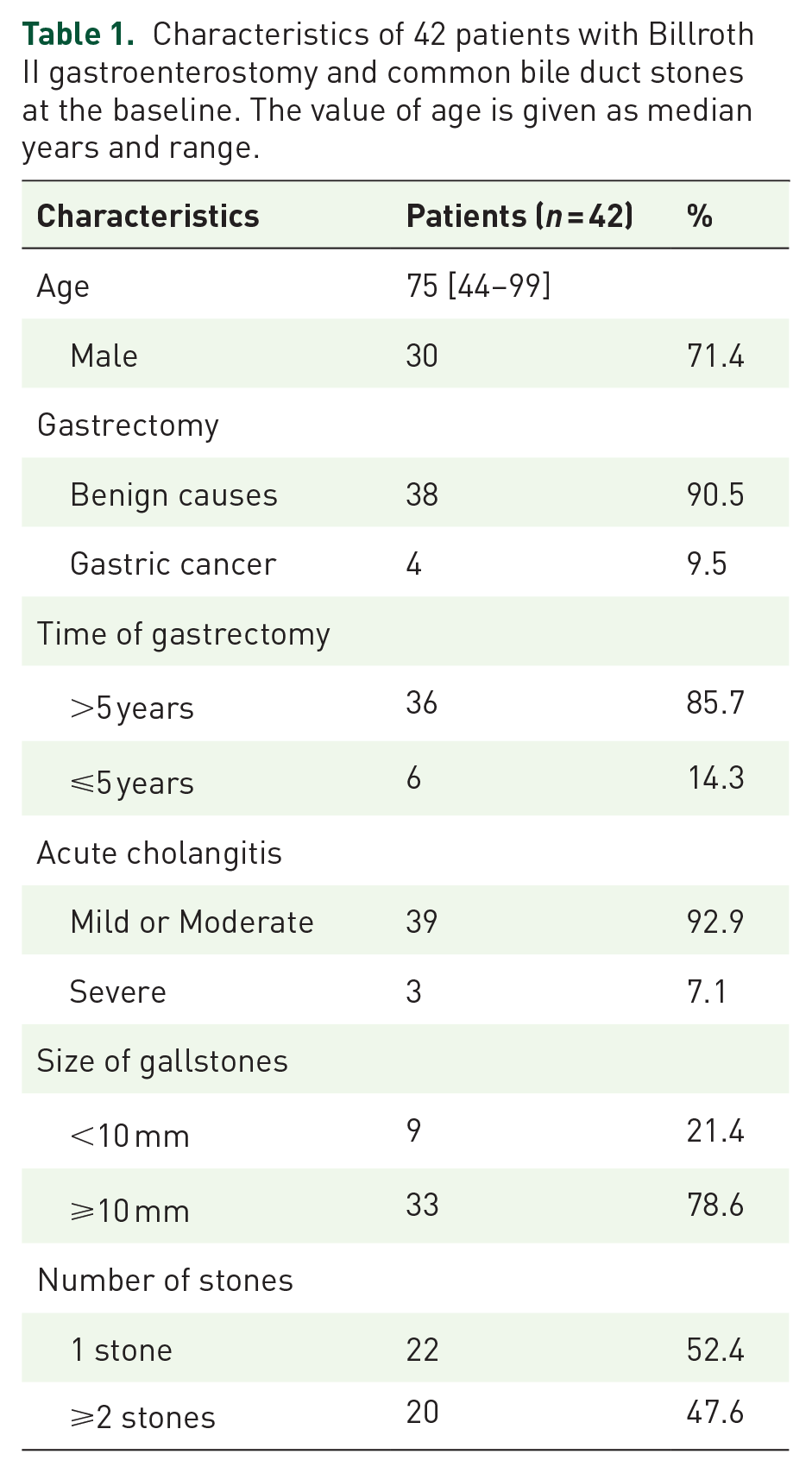
The demographic characteristics of the 42 B-II GE study participants are summarized in Table 1. Of the 42 patients, 30 (71.4%) were male and 12 (28.6%) were female. The mean age of the patients was 75 (44–99 years). Most patients (~90%) underwent gastrectomy for more than 5 years because of benign diseases. As a predictive treatment approach, all patients suffered from acute cholangitis, primarily at mild to moderate levels. Additionally, all individuals presented gallstones based on imaging results, with approximately three-quarters having gallstones larger than 10 mm in size and nearly half having more than one CBD stone. Moreover, half of the patients presented with the symptoms of Charcot’s triad, and most liver function tests were elevated. Still, the elevation can range from mild to moderate (data not shown).
Characteristics of 42 patients with Billroth II gastroenterostomy and common bile duct stones at the baseline. The value of age is given as median years and range.
Results of endoscopic retrograde cholangiopancreatography treatment for gallstones
The results of ERCP are shown in Table 2. Of 42 patients, 39 had Vater’s ampulla located (92.9%). Subsequently, the success rate of cannulation reached 94.9% (37/39 patients, data not shown). Therefore, the overall success rate of the ERCP procedure was 88.1%.
The efficacy of ERCP in the treatment of CBD among the patients with Billroth II gastroenterostomy.

ERCP, endoscopic retrograde cholangiopancreatography; CBD, common bile duct.
Regarding the stone retrieval results, there were 27 out of 37 cases where complete gallstone removal was achieved (73%). In 13.5% (5/37) of the patients, only a portion of the stones could be removed, necessitating the placement of an additional biliary stent. In the remaining cases, stone extraction was unsuccessful, requiring stent placement for bile duct clearance.
Following the ERCP procedure, there was a notable improvement in the patient’s clinical symptoms (data not shown). Moreover, inflammatory, biliary obstruction and liver damage markers also demonstrated statistically significant reductions compared to the pre-ERCP intervention values (WBC 12.5 G/l versus 8.7 G/l; total Bilirubin 52.3 µmol/l versus 27.5 µmol/l; AST/ALT 138/121 U/l versus 37/48 U/l; pre-ERCP and post-ERCP respectively) (Table 3).
Clinical indicators of the inflammatory response, biliary obstruction, and liver injury before and after ERCP intervention in Billroth II gastroenterostomy patients with CBD. The value of WBC is given as medium and standard deviation. The value of total bilirubin, AST, and ALT are given as median (Q1–Q3).

ERCP, endoscopic retrograde cholangiopancreatography; CBD, common bile duct; WBC, white blood cells; AST and ALT, aspartate and alanine amino transferase.
Characteristics and efficacies of the ERCP technique
The characteristics of the ERCP technique are presented in Table 4. Out of 37 technically successful patients, the conventional endoscope (67.6%) was predominantly utilized for the procedure. During the intervention process, 14 patients (37.8%) required pre-cut sphincterotomy to achieve cannulation. Following sphincterotomy, most patients (89.4%) underwent balloon dilation to widen Vater’s ampulla. Subsequently, 32 out of 37 patients had partial or complete stone removal, mainly utilizing stone retrieval balloons. Among them, 14 cases (43.8%) required fragmentation of stones into smaller pieces before extraction.
Type of ERCP intervention in treatment CBD among patients of prior Billroth II gastroenterostomy.

ERCP, endoscopic retrograde cholangiopancreatography; CBD, common bile duct.
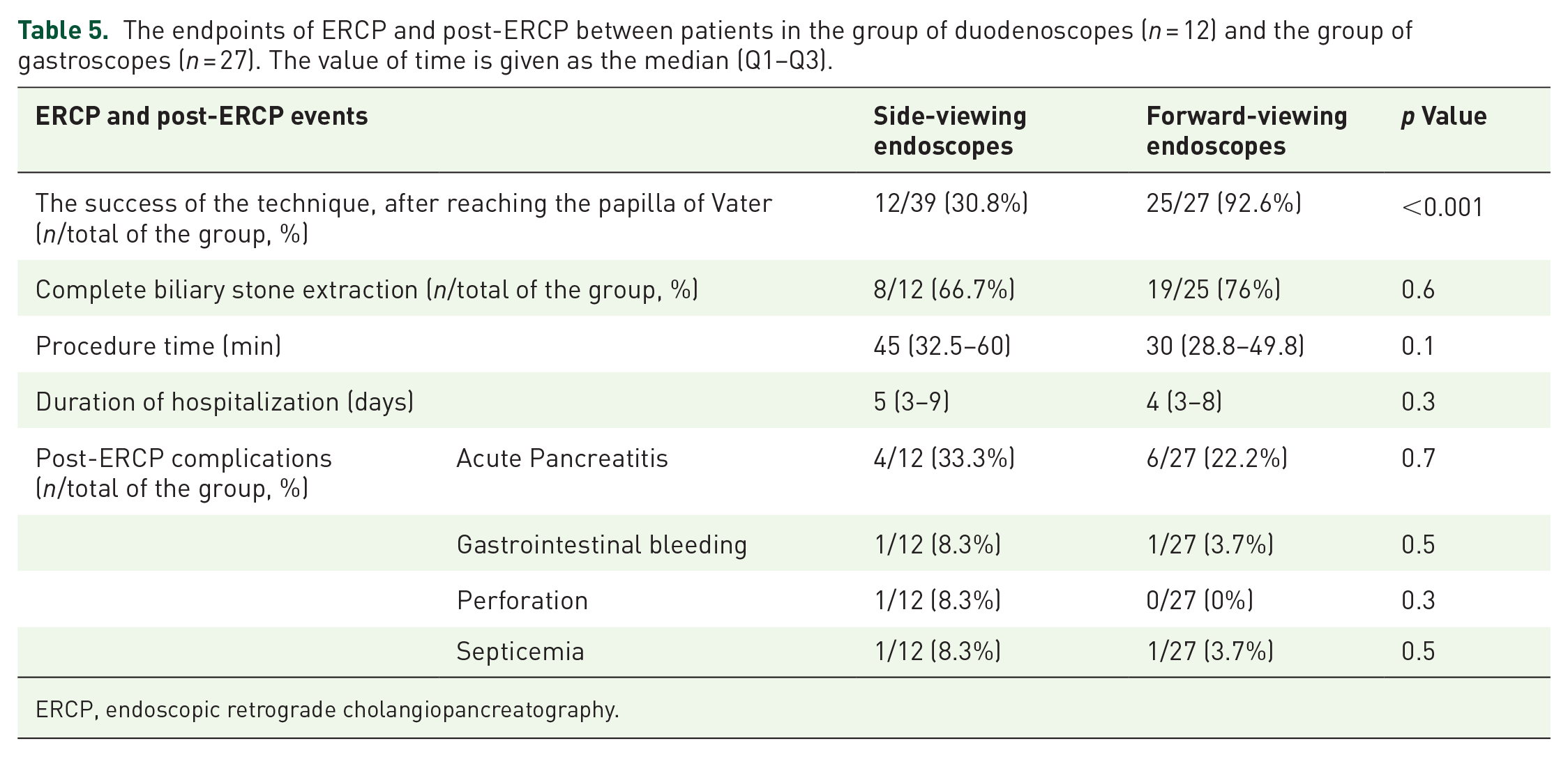
Analysis of the treatment outcomes for patients with bile duct stones and a history of gastric resection, Billroth II reconstruction, using endoscopic interventions was performed: either a side-viewing endoscope or a forward-viewing endoscope, as described in Table 5. When locating the Vater’s papilla, the stone extraction technique using a side-viewing endoscope was successful in 12 out of 39 cases (30.8%), significantly lower than the success rate of the method using a forward-viewing endoscope in 25 out of 27 cases (97.6%), p < 0.001. Subsequently, after successfully cannulating the bile duct, the rates of complete stone removal were similar for both methods, p > 0.05. Moreover, the time required for performing ERCP with a side-viewing endoscope appeared longer than the forward-viewing endoscope, but the analysis did not show statistical significance. The hospitalization duration for patients in both groups using the two techniques also did not differ. Lastly, the analysis under the subgroup of patients based on the size of bile duct stones showed no statistically significant difference in the number of stones in the bile duct between the two patient groups (data was not shown).
The endpoints of ERCP and post-ERCP between patients in the group of duodenoscopes (n = 12) and the group of gastroscopes (n = 27). The value of time is given as the median (Q1–Q3).
ERCP, endoscopic retrograde cholangiopancreatography.
Safety of the technique
The complications of ERCP are described in Figure 2. The most common complication following ERCP is acute pancreatitis, accounting for 23.8% (10 out of 42 patients), but all cases were of mild severity. Other complications were observed at lower rates: post-sphincterotomy bleeding 2/42 (4.8%), duodenal perforation 1/42 (2.4%), and septicemia 2/42 (4.8%). Notably, no cases of mortality were recorded.

The complication of ERCP procedures among the patients with B-II GE using all techniques versus the forward-viewing endoscope with cap-assisted.
Complications and adverse events after ERCP in patients undergoing intervention with a forward-viewing endoscope equipped with a cap are presented in Figure 2 and Table 5. The overall complication rate for the patients using a forward-viewing endoscope was equivalent to that for patients in the study population (Figure 2). The incidence of common complications of ERCP in patients using the forward-viewing endoscope appears to be lower than in patients using the side-viewing endoscope (Table 5); however, the analyses did not reach statistical significance, p > 0.05.
Discussion
Gallstone disease is a common hepatopancreatic disorder, particularly prevalent in Vietnam. Among these patients, around 1–2% have a history of gastric resection surgery. In patients who have undergone Billroth II gastric resection with reconstruction and develop common bile duct stricture, the altered anatomy presents technical challenges for duodenal intubation and selective bile duct cannulation during ERCP procedures. This results in a lower success rate of duct clearance and a higher incidence of complications than conventional ERCP.5,10 Consequently, surgical or percutaneous transhepatic interventions are often preferred in such cases. This led to longer hospital stays, increased costs, extended postoperative treatment time, and a higher risk of complications, particularly in elderly patients. ERCP can be an excellent option for this patient group if the technique can be successfully executed. It offers better treatment effectiveness, shorter hospitalization duration, and fewer complications.
Factors preventing scope insertion into the descending portion of the duodenum in Billroth II gastric resection cases include a long afferent loop and sharp anastomosis angles. The manual compression method and specialized scopes have proven effective in addressing challenging intubation of the descending duodenum. Successful retrograde endoscopic pancreatic procedures necessitate specialized instruments and experienced experts. Different techniques, such as double-balloon enteroscopy or anterior-viewing endoscopes with caps attached to their tips, have been reported worldwide. 11 However, data is limited, especially regarding forward-viewing endoscopes in Vietnam patients with Billroth II gastric resection.
This study demonstrates the efficacy of ERCP in 42 patients with Billroth II gastric resection, including 25 patients who underwent end-viewing endoscopy with a cap attached. Available tools were used, including forward-viewing endoscopes, colonoscopes, and side-viewing endoscopes. The forward-viewing endoscope easily navigates into the duodenum, ensuring safety due to its ability to visualize the intestinal lumen; however, cannulation and sphincterotomy are challenging due to the lack of an Elevator. In addition, forward-viewing endoscopes have a small working channel, causing difficulties in interventions such as double guidewires or a stone fragmentation basket/stone retrieval basket. On the other hand, the side-viewing endoscope encounters difficulties while advancing into the duodenum, and there is a higher risk of duodenal perforation. A hybrid approach combining the advantages of both forward-viewing and side-viewing endoscopes increased success rates and reduced complications, particularly severe ones like perforation, acute pancreatitis, or severe bleeding. 8 Initially, the papillae of all patients were examined by a gastroscope, and subsequently, a guidewire navigator was used. The cannulation was attempted by a duodenoscope with a side-viewing endoscope, consequently by a forward-viewing endoscope if the former failed. The study’s utilization rate of forward-viewing and side-viewing endoscopes was 67.6% and 32.4%, respectively. Highlightly, only one-third of patients were suitable for duodenscopy in ERCP treatment of common bile duct (CBD).
Efficacy of modification in ERCP-treated common bile duct stones
The overall success rate of the ERCP technique was 88.1% (37 out of 42 patients). Our results are similar to those of Wu et al., 12 who performed CBD stone fragmentation on 10 patients with B-II GE using a dual-balloon endoscope, achieving a success rate of 9 out of 10 patients.
Despite anatomical changes post-gastrectomy and Billroth II reconstruction, which impact stomach anatomy and Vater’s ampulla position, endoscopy and guidewires improve ampullary detection and interventions. Of the 39 patients who accessed Vater’s ampulla, 37 achieved successful stone retrieval (accounting for 94.4%), wholly or partially. Our study’s success rates in cannulation and stone clearance align with those reported globally.13,14 Complete stone removal was achieved in 73% of cases, with partial extraction in 13.5%. These rates are lower than typical patients but align with other gastrectomy-related reports. In five cases, initial removal wasn’t possible due to severe systemic conditions; these patients received biliary stents for temporary relief. Post-ERCP, clinical indicators, bile duct inflammation, and obstruction significantly improved. Technical success and stone removal showed no difference between the end-viewing endoscope and duodenoscope groups (Data not shown).
The study’s Oddi’s sphincter balloon dilation rate was 89.2%, differing from traditional sphincterotome cutting. Due to Vater’s ampulla access, Billroth II gastrectomy patients can’t have Oddi’s sphincterotome cut with a sphincterotome. Our technique’s safety and effectiveness were evaluated by foreign authors.15,16 Pre-cut sphincterotomy with a needle knife is used when bile duct cannulation is challenging. 17 A total of 38.4% underwent pre-cut sphincterotomy due to Billroth II’s challenging cannulation with a forward-viewing endoscope. We prefer stone retrieval balloons (64.5%) due to altered gastrectomy anatomy, making cannulation more challenging. We actively fragment larger stones before retrieval with the balloon, as it offers more control over the guidewire than baskets.
In this study, among 42 patients with Billroth II gastric resection, 39 cases were found in the Vater’s papilla. After that, 12 individuals were successfully treated with CBD stones. Consequently, among the rest of the patients, 25 underwent front-viewing endoscopy with a cap attached, achieving a much higher treatment success rate (92.6%) (Table 5). Moreover, the treatment outcomes for bile duct stones using the forward-viewing endoscope are equivalent to those using the side-viewing endoscope. Patients undergoing ERCP with the forward-viewing endoscope seemed to have a shorter procedure time and earlier discharge compared to patients undergoing ERCP with the side-viewing endoscope. Therefore, the forward-viewing endoscope has improved ERCP’s effectiveness and success rate in patients with a history of gastric resection.
Safety of ERCP treating CBD stone in patients’ prior Billroth II gastrectomy
Performing CBD stone extraction through retrograde endoscopic pancreatic procedures in patients who have undergone Billroth II gastrectomy is challenging due to the altered gastrointestinal anatomy. Prior studies have reported a duodenal perforation rate ranging from 1.8 to 10.2%. 18 Our research encountered a single duodenal perforation (2.4%) in an 83-year-old female patient using a side-viewing endoscope. The perforation occurred while advancing the endoscope through the adhered and immobile duodenal stump. We promptly managed the situation by applying eight clips and successfully completing the stone extraction procedure. The patient was discharged in stable condition after 5 days. Additionally, two cases (4.8%) experienced mild to moderate gastrointestinal bleeding at the pre-cut sphincterotomy site, and conservative treatment was effective. While pre-cut sphincterotomy using a needle knife is associated with higher bleeding risk, we noted that in Billroth II gastrectomy patients, it offers a more favorable condition for cannulation. This technique requires skilled endoscopists. Nonetheless, acute pancreatitis is the most common complication of ERCP for treating stones in patients with a history of gastric resection, with an incidence rate of 23.8%. This rate is higher than the incidence of acute pancreatitis after ERCP in regular patients, 19 and the reason was the altered position of the Vater’s papilla and the biliary-pancreatic axis after gastric resection, which increases the risk of entry into the pancreatic duct. Importantly, all cases of acute pancreatitis were mild and resolved independently. Hence, our study suggests that ERCP for CBD stone treatment in Billroth II gastrectomy patients may pose complications similar to those of conventional ERCP techniques. However, these complications are generally mild and manageable through endoscopic interventions and conservative measures.
Cap-assisted endoscopy is a well-established technique used in mucosectomy for early gastric cancer and aiding the detection of ‘blind area’ lesions in the gastrointestinal tract.8,20 It also offers the advantage of maneuvering anatomical structures, like the papilla in our patients, to facilitate endoscopic therapy. The cap stabilizes the endoscope while allowing ample room for treatment. Further research is needed to determine if routine cap use improves cannulation rates in ERCP patients with a B-II GE history. In our study, we employed cap-assisted endoscopy with all patients using a forward-viewing endoscope, which could potentially reduce ERCP procedure complications. ERCP using a forward-viewing endoscope with a cap has a lower complication rate after the intervention than using a side-viewing endoscope, especially with a significant reduction in the risk of perforation (Table 5). Although the analysis results indicate that this difference was not statistically significant, it might be due to the small size of the study sample, lacking sufficient power for analysis.
In Vietnam, this pioneering study explores the effectiveness of utilizing forward-viewing or side-viewing endoscopes in ERCP for treating common bile duct stones in patients with a history of gastric resection in Vietnam. The findings are promising, but several limitations should be noted. Firstly, the sample size is modest (n = 42). While the study demonstrates a noteworthy success rate and reduced complications, a larger sample is required to establish direct correlations between specific endoscope types and treatment outcomes. Secondly, being a single-center study, its generalizability to the broader population might be limited. Thirdly, the study’s retrospective-prospective design over an extended period may not fully capture the impact of the enhanced ERCP technique using cap-assisted forward-viewing endoscopes. Lastly, the study exclusively examines patients with Billroth II gastric reconstruction without encompassing other variations such as Billroth I or Braun procedures.
In conclusion, our study highlights that utilizing cap-assisted forward-viewing endoscopes for ERCP could be a primary and practical approach to treating common bile duct stones in patients with a Billroth II gastric resection history in Vietnam. While it yields high treatment efficacy with acceptable complications, it’s worth noting that this technique demands a high level of procedural expertise. Therefore, conducting multiple training sessions to enhance the skills of interventionists is crucial.
Footnotes
Acknowledgements
We thank all patients and healthy individuals for their participation. We would also like to express our gratitude to the medical teams, nurses, and anesthesiologists who successfully and safely performed the ERCP procedures for the patients.